

")
Publication History
Submitted: July 23, 2025
Accepted: August 11, 2025
Published: August 30, 2025
Identification
D-0486
DOI
https://doi.org/10.71017/djmi.4.8.d-0486
Citation
Katrina M. Pattaguan & Aurelio P.S. Reyes (2025). Purple Urine Bag Syndrome in an Elderly Female with Cerebrovascular Disease. Journal of Medical Innovations, 4(08):538-541.
Copyright
© 2025 The Author(s).
538-541
Purple Urine Bag Syndrome in an Elderly Female with Cerebrovascular DiseaseCase Study
Katrina M. Pattaguan 1*, Aurelio P.S. Reyes 2
1,2 Veterans Memorial Medical Center, North Avenue, Quezon City, Philippines.
* Correspondence: katrina.pattaguan@gmail.com
Abstract: Purple urine bag syndrome is an unusual condition of urinary tract infections resulting in purple discoloration of the urine and was first described by Barlow and Dickson in 1978. Considering its rarity, this condition has remained to be under recognized throughout the years. Interestingly, despite the common occurrence of urinary tract infections in patients with risk factors for PUBS, this syndrome is not commonly encountered, because it requires the simultaneous presence of other possible various factors like having a high tryptophan in the diet being an essential amino acid, presence of phosphatase and sulphatase producing bacteria, alkaline urine, chronic debilitation, constipation and chronic catheterization. A 93-year-old female managed as a case of Acute Cerebral Infarction, chronically bedridden due to previous history of cerebrovascular infarct and unable to perform essential activities of daily living without assistance. Patient was managed as a case of acute cerebrovascular infarct in a previously bedbound condition and foley catheter was inserted upon admission. She then developed fever and back pain on the 6th hospital day and purple urine discoloration was noted on the catheter bag on the 8th day of admission. Laboratories showed leukocytosis with neutrophilic predominance on blood count and urinalysis showed alkaline urine (pH of 8) with the urinary sediments of white blood cells 60-70/high power field. Collected specimen for urine cultures showed heavy growth of Escherichia coli (>100,000 cfu/mL) sensitive to Ceftriaxone. Purple urine bag syndrome, although a harmless occurrence can be alarming to the patient and caregivers given the inexplicable sudden purple discoloration of the urine in the catheter bag. This being an under recognized phenomenon can lead to unwanted morbidity and mortality if not timely managed. The prevention and control of the hospital acquired catheter-associated UTIs (CAUTIs) through various measures have become the thrust in the management of PUBS. Health workers must have increased awareness of this phenomenon as prevalence of PUBS can be higher than actual reported cases.
Keywords: purple urine bag syndrome, elderly female, cerebrovascular disease
- INTRODUCTION
Purple urine bag syndrome is an unusual condition of urinary tract infections resulting in purple discoloration of the urine and was first described by Barlow and Dickson in 1978 [1,2] Considering its rarity, this condition has remained to be under recognized throughout the years. Interestingly, despite the common occurrence of urinary tract infections in patients with risk factors for PUBS, this syndrome is not commonly encountered, because it requires the simultaneous presence of other possible various factors like having a high tryptophan in the diet being an essential amino acid, presence of phosphatase and sulphatase producing bacteria, alkaline urine, chronic debilitation, constipation and chronic catheterization [3,4,5]. This condition maybe be benign, but this poses a great distress to the patient and caregivers as it can lead to unwanted morbidity and mortality. We present, an elderly female patient, chronically bedridden, managed as a case of Acute Cerebral Infarction with an indwelling catheter and chronic constipation admitted at Veterans Memorial Medical Center, which to our knowledge, is the first case in our institution and second in the country.
- CASE DESCRIPTION
We report a 93-year-old female managed as a case of Acute Cerebral Infarction, chronically bedridden due to previous history of cerebrovascular infarct and unable to perform essential activities of daily living without assistance. Patient was also noted to have chronic constipation which was addressed by giving laxatives. Patient was managed as a case of acute cerebrovascular infarct in a previously bedbound condition and foley catheter was inserted upon admission. She then developed fever and back pain on the 6th hospital day and purple urine discoloration was noted on the catheter bag on the 8th day of admission. Pertinent physical examination manifested diffuse tenderness upon palpation of the hypogastric area of the abdomen. Laboratories showed leukocytosis with neutrophilic predominance on blood count and urinalysis showed alkaline urine (pH of 8) with the urinary sediments of white blood cells 60-70/high power field. Collected specimen for urine cultures showed heavy growth of Escherichia coli (>100,000 cfu/mL) sensitive to Ceftriaxone. After ruling out other causes of fever and infection, patient was managed as a case of catheter related urinary tract infection and was empirically started on Ceftriaxone which was eventually completed for 7 days based on the culture results. The foley catheter was likewise simultaneously changed. Lactulose was continued to address patient’s constipation. The purple urine gradually disappeared by day 3 of antibiotics and complete clinical resolution was seen upon completion of the antibiotics.
- DISCUSSION
Urinary tract infections are the most common type of healthcare-associated infection and 75% of which are urinary catheter related. This makes catheter related urinary tract infections as the most common nosocomial infection with a prevalence of 8.3-42.1% [6,7]. A study published by an author showed the prevalence of PUBS to be as high as around 9.8% in hospitalized patients with long-term catheter use [8]. The mechanism of this phenomenon (see figure 2) is explained by the conversion of tryptophan into indigo and indirubicin, which are color blue and red respectively. Intestinal bacteria will metabolize tryptophan to indole which is absorbed into the portal circulation and converted to indoxyl sulphate/phosphate which is eventually excreted in the urine in high concentration. In the event of an existing urinary tract infection in the presence of an alkaline urine, responsible bacteria like Escherichia coli, Providencia stuartii, Klebsiella pneumoniae produce sulphatase/phosphatase and metabolize indoxyl sulfate/phosphate to indoxyl. Through oxygenation, indoxyl in turn produces indigo (blue) or indirubin (red), which when mixed together spontaneously yields the purple discoloration [5]. Risk factors of this syndrome include female gender, advanced age, immobilization, chronic catheterization, high urinary bacterial load, alkaline urine and poor hygiene, which are all present in our patient [9,10]. Chronic constipation, as seen in our patient and intestinal obstruction were also noted to be largely associated with PUBS. This higher occurrence in such patients was attributed to decrease in intestinal motility leading to bacterial overgrowth in the intestine, hastening metabolism of tryptophan to indole, yielding high levels of indigo and indorubicin in which combination is responsible for its purple discoloration [4]. A study described the use of PVC Plastic catheter on patients with PUBS and the duration from the last catheterization and appearance of urine purple discoloration was on average 65 days [11,12]. In our patient, PUBS became apparent after less than one week of admission and catheter insertion. The management of PUBS points towards the identification of the underlying pathogen, which in most cases is bacterial urinary tract infection and treatment with the appropriate antibiotic. Along with this, preventing or addressing the constipation with the administration of laxatives (e.g. lactulose) is also essential so to decrease the nidus for bacterial overgrowth. Changing the urinary catheter along with the collection bag regularly is part of the prevention of its occurrence and genitourinary sanitation is as well prudent to its treatment [10]. PUBS is generally a benign process and offers a good prognosis if timely and appropriately addressed.

Figure 01: Purple urine discoloration shown in the catheter bag and tubing’s
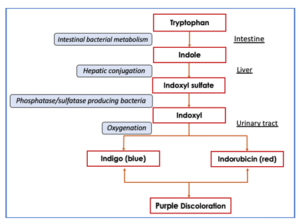
Figure 02: Diagram describing the pathogenesis of Purple Urine Bag Syndrome
- CONCLUSION
Purple urine bag syndrome, although a harmless occurrence can be alarming to the patient and caregivers given the inexplicable sudden purple discoloration of the urine in the catheter bag. This being an under recognized phenomenon can lead to unwanted morbidity and mortality if not timely managed. The prevention and control of the hospital acquired catheter-associated UTIs (CAUTIs) through various measures have become the thrust in the management of PUBS. Health workers must have increased awareness of this phenomenon as prevalence of PUBS can be higher than actual reported cases. Familiarity with this syndrome will prompt immediate intervention leading to lesser hospital stay, avoidance of complications and unnecessary additional expenses.
REFERENCES
- Su FH, Chung SY, Chen MH, et al. Case analysis of purple urine-bag syndrome at a long-term care service in a community hospital.Chang Gung Med J. 2005;28:636–42.
- Chitrasen Yadav, Prof. Pradeep Vaidya, Dr. Laligen Awale, Dr. Geha Raj Dahal, Sanjeeb Jha & Krishna Yadav (2024). Evaluation of Surgical Site Infections and Patterns of Microorganisms involved in Emergency Laparotomy in TUTH . Dinkum Journal of Medical Innovations, 3(08):557-569.
- Dealler SF, Hawkey PM, Millar MR. Enzymatic degradation of urinary indoxyl sulfate by Providencia stuartii and Klebsiella pneumoniae causes the purple urine bag syndrome. J 1988;26:2152‑6.
- Jones RA, Deacon HJ, Allen SC. Two cases and a short discussion of purple urine bag syndrome. CME Geriatr Med. 2003;5:84‑
- Dealler SF, Hawkey PM, Millar MR. Enzymatic degradation of urinary indoxyl sulfate by Providencia stuartii and Klebsiella pneumoniae causes the purple urine bag syndrome. J Clin Microbiol. 1988 Oct;26(10):2152-6.
- Al Montasir A, Al Mustaque A: Purple urine bag syndrome. J Fam Med Primary Care. 2013;2(1):104–5.
- Centers for Disease Control and Prevention. (2015).
- Dealler SF, Hawkey PM, Millar MR. Enzymatic degradation of urinary indoxyl sulfate by Providencia stuartii and Klebsiella pneumoniae causes the purple urine bag syndrome.J Clin Microbiol. 1988;26:2152.
- Su FH, Chung SY, Chen MH, et al. Case analysis of purple urine-bag syndrome at a long-term care service in a community hospital. Chang Gung Med J. 2005;28:636–42.
- Khan F, Chaudhry MA, Qureshi N, Cowley B. Purple urine bag syndrome: an alarming hue? A brief review of the literature. Int J Nephrol. 2011;2011:419213.
- Kannan L, Bauman AA. Purple urine in a patient with UTI and constipation. Oxf Med Case Reports. 2023 Feb 27;2023(2).
- Neniwal VK, Swain S. et al. Purple urine bag syndrome: An unusual manifestation of urinary tract infection, our experience at a tertiary care center. Curr Urol. 2023 Jun;17(2):125-129.
Publication History
Submitted: July 23, 2025
Accepted: August 11, 2025
Published: August 30, 2025
Identification
D-0486
DOI
https://doi.org/10.71017/djmi.4.8.d-0486
Citation
Katrina M. Pattaguan & Aurelio P.S. Reyes (2025). Purple Urine Bag Syndrome in an Elderly Female with Cerebrovascular Disease. Journal of Medical Innovations, 4(08):538-541.
Copyright
© 2025 The Author(s).