

")
Publication History
Submitted: July 23, 2025
Accepted: August 11, 2025
Published: August 30, 2025
Identification
D-0487
DOI
https://doi.org/10.71017/djmi.4.8.d-0487
Citation
Acharya Barsha, Smriti Karki, Anju Pradhan & Punam Paudyal (2025). Utility of Supravital Toluidine Blue Stain as Rapid Staining Technique in Fine Needle Aspiration Cytology. Journal of Medical Innovations, 4(08):542-566.
Copyright
© 2025 The Author(s).
542-556
Utility of Supravital Toluidine Blue Stain as Rapid Staining Technique in Fine Needle Aspiration CytologyOriginal Article
Acharya Barsha 1*, Smriti Karki 2, Anju Pradhan 3, Punam Paudyal 4
- Doctor of Medicine (MD) Pathology, B.P Koirala Institute. Of Health Sciences (BPKIHS), Dharan, Nepal.
- Professor, Department of Pathology, B.P Koirala Institute. Of Health Sciences (BPKIHS), Dharan, Nepal.
- Additional Professor, Department of Pathology, B.P Koirala Institute. Of Health Sciences (BPKIHS), Dharan, Nepal.
- Additional Professor, Department of Pathology, B.P Koirala Institute. Of Health Sciences (BPKIHS), Dharan, Nepal.
* Correspondence: barsha.acharya01@gmail.com
Abstract: In early 1950s, Fine Needle Aspiration Cytology (FNAC) as a technique evolved subsequently. FNAC is a simple, relatively less invasive, easy to perform and cost-effective technique which is used to examine lesions in various anatomical locations. This is a hospital based prospective study conducted in the Cytopathology Lab, Department of Pathology, BPKIHS, Nepal. This study assessed the utility of Toluidine Blue stained as rapid staining technique in FNAC. Sixty-one (61) cases were enrolled in this study. Toluidine blue staining (TBS) was adequate in all 61 cases (100%) because the smear was reaspirated on site in the cases after screening the slides for cellularity. However, Papanicolaou stained slides had 7 (11.47%) inadequate cellularity on smears and underwent repeat FNAC on next visit. Toluidine blue staining showed preserved cell morphology in 55 (90.1%) cases and cell morphology of 6 (9.8%) cases was not preserved. Papanicolaou staining showed preserved cell morphology in 56 (91.8%) cases and cell morphology was not preserved in 5 (8.1%) cases. Toluidine blue stain smears showed crisp chromatin in 48 (79%) cases and smudge chromatin in 13 (21.3%) cases. Papanicolaou staining showed crisp chromatin in 30 (49.1%) cases and smudge chromatin in 31 (51%) cases. Toluidine Blue staining showed clean background in 59 (97%) cases and hemorrhagic background in 2(3.27%) cases. Papanicolaou staining showed clean background in 7(11.4%) cases and hemorrhagic background in 54 (88.5%) cases. Toluidine Blue staining showed atypical/neoplastic cells in 22 (36.05%) cases and lacked atypical cell or showed non-neoplastic cells in 39 (64%) cases. Similarly, Papanicolaou staining showed atypical/neoplastic cells in 19 (31.1%) cases and lacked atypical cell or showed non-neoplastic cells in 42 (69%) cases. The Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Diagnostic Accuracy of Toluidine Blue stained smears in the present study were 100%, 92.8%, 86.36%, 100%, 95.08% respectively. The average time taken to screen the slides for identifying atypicality’s using rapid onsite toluidine blue stain was found to be approximately less than 2 minutes after performing FNAC.
Keywords: supravital toluidine blue, stain, staining technique, fine needle aspiration cytology
- INTRODUCTION
In early 1950s, Fine Needle Aspiration Cytology (FNAC) as a technique evolved subsequently [1]. FNAC is a simple, relatively less invasive, easy to perform and cost-effective technique which is used to examine lesions in various anatomical locations [2]. It helps in diagnosis and eliminating the probability of unnecessary investigations and inappropriate operations, and allows the clinicians to plan and manage accordingly [3]. Diagnostic accuracy of FNAC depends on many factors like: Representativeness of sample, adequacy of sample and good cytomorphological detail without much artifactual distortion [4]. FNAC technique has become more common and popular nowadays. Though it is not a substitute for conventional histopathology, it should be regarded as a very important component of pre-operative/ pre-treatment investigation in combination with clinical, radiological and other laboratory data [5]. Therefore, it is necessary to find out the adequacy of the cells as early as possible, so every aspiration should undergo an evaluation for adequacy. Following an adequacy assessment by rapid on site staining and evaluation and reaspiration of inadequate FNAC sample at first visit limits visit number [7]. It also shortens the time for definitive diagnosis, management and treatment as well as saves time, money and manpower [6]. The smear is stained with different stains for microscopic examination in order to reach a proper diagnosis. Since its inception, Papanicolaou (Pap) stain remains the traditional and preferred stain, not only for the gynecological cytology, but also for the lesions of other organs. There are many stains like H and E, May-Grunwald stain, Papanicolaou stain which are used routinely for staining and interpretation of FNAC smears. However, no universal rapid on-site stain has been identified. George N. Papanicolaou in 1942 developed Pap stain which yields a polychromatic, transparent staining reaction with crisp nuclear and cytological features, but it utilizes a considerable amount of ethyl alcohol for fixation and takes longer time [5]. The traditional Pap stain involves wet fixation and subsequent staining, together requiring at least 30 minutes. Rapid on-site evaluation (ROSE) is a cytomorphological diagnostic procedure which allows quick assessment of sample for adequacy and dramatically reduces the rate of failures as it provides information regarding the need for obtaining additional material or avoiding further repetition of the procedures for cytological evaluation [9]. It is also useful in triage of specimens for ancillary studies and in emergency cases as well as it helps in determining a preliminary diagnosis [10]. For ROSE technique, there are different rapid stains used like Toluidine Blue, Diff-quick, Brilliant Creysl Blue, Modified Ultrafast Pap etc. [11]. Toluidine Blue is a basic metachromatic dye with high affinity for acidic components like nucleic acids and binds to nuclear material tissues with high DNA and RNA, so accentuates good nuclear and nucleolar details [12]. It is a supravital stain which is used for reticulocyte count in Hematology [2]. The diagnostic accuracy of TBS in some studies was about 100 % as compared to 84% of the Papanicolaou stained smears due to high percentage of inadequacy by the conventional PAP staining technique [6]. The sensitivity of Toluidine Blue was 100% and specificity to be 97.28% when compared with the routine stains for inflammatory, benign and malignant diagnosis [11]. Some showed that TBS yielded 100% accuracy in all cases of aspirates whereas PAP stain study gave 78% accuracy and the rate of efficiency for onsite reporting for TBS was 100% while for PAP no onsite report was sent for reporting of fine needle aspiration [13]. Though many conventional stains are being used to stain the FNAC smears like Papanicolaou, Giemsa or Hematoxylin and eosin (H&E) stains, these take a little longer time to prepare and full-length laboratory setup is required to use these stains as well as these are expensive. On the other hand, Toluidine Blue stain is easily available, simple staining technique, least labor intensive, less expensive, reduces exposure to solvents as only alcohol-based fixatives is used, and reliable rapid stain for ROSE which gives the result within 2 minutes of the staining [14]. For Interpretation of Toluidine Blue staining, smears were graded visually depending on cellularity/adequacy, cell morphology, nuclear details and background. These parameters were later on compared with the routinely stained Papanicolaou stained smears [11]. The cell adequacy was based on whether the cells present were enough to make a diagnosis, whether they were distributed uniformly or focally and was expressed as adequate or inadequate accordingly. In case of inadequate sample with onsite evaluation in Toluidine Blue stained smears, repeat on site aspiration, staining and evaluation was done. For Cell morphology, shape of the cell such as round, spindle shaped or elongated, cellular pattern and cytoplasmic membranes were considered. Then the smears were classified as preserved cell morphology or distorted (not preserved) cell morphology. Nuclear features played an important role in differentiating neoplastic lesions from non-neoplastic lesions and the features considered were based mainly on staining quality of nuclear chromatin. Smears were compared on the basis of cells having smudgy chromatin and crisp chromatin. The background was assessed by observing for hemorrhage, inflammation, necrosis, mucinous material and whether these features obscured the cellular morphology or aided in the diagnosis of rapid smears were taken into account. The smears were then compared as having clean background or hemorrhagic background. In the resource limited setting, where there is limited number of manpower available, low cost for well setup laboratory, the use of Toluidine Blue as rapid staining technique will aid as screening tool for adequacy assessment as well as in the preliminary diagnosis which fasten the diagnosis time and will be helpful for the clinician to carry out the treatment [11]. So, this study evaluated the utility of Toluidine Blue stain to determine the adequacy for rapid and early diagnosis of FNAC samples and compare it to Papanicolaou stain. If TBS is found to be as efficient as Pap stain, it can also be used in routine FNAC and not just on-site stain. This study determined the efficacy of Toluidine blue for adequacy on rapid onsite staining technique of FNAC samples in comparison to Papanicolaou stain.
- MATERIALS & METHOD
This is a cross-sectional study performed for a period of 1 year and the Patients with any palpable Lymph node, thyroid swelling, breast lumps, salivary gland swelling subjected to FNAC OPD are included. This proposal was submitted to Institutional Review Committee, BPKIHS. All the FNAC was carried out after obtaining informed consent from the patients. This research was conducted after getting review from the institutional review committee and post graduate protocol committee. Purposive Sampling technique was implied. Well Informed consent was taken from all patients/ patient party and proforma was filled. In this study, patient attending FNAC OPD were asked about detailed clinical history regarding chief complaints, onset of swelling, any significant family history, family history. Informed written Consent was taken before the procedure. Swelling was examined on the basis of site and number on inspection and its size, tenderness and consistency on palpation. Patient were counseled about the procedure along with the limitations of FNAC with informed written consent documented from all the patients. The patient was made comfortable on the bed and skin over the swelling to be aspirated is cleaned by using spirit swab. Lesion was fixed with fingers and FNAC was performed using 23 gauze needles attached with 10ml syringe. By pulling the plunger, negative pressure was applied and the needle was carefully moved to and fro in all the directions in the lump. After the needle was withdrawn, nature of the aspirated material was recorded and the aspirated content was expressed on clean, grease free glass slide with proper labelling of the patient identity number or name. Then by applying a gentle pressure with another glass slide, the smears were made. Usually minimum of 7 slides were made immediately from the aspirated material. Out of seven slides, two were immediately immersed in 95% alcohol for fixation and stained with pap stain. The other three were air dried and stained with Giemsa stain. Two slides were stained with Toluidine Blue stain. Sample collection was done in the FNAC procedure room. Then on the same room, within 45 seconds of time duration, the Toluidine blue stained slides were prepared. All the patients were requested to wait for 5 min after FNA was performed in order to confirm specimen adequacy by rapid staining procedure and on-site evaluation. The under surface of the slides were wiped with tissue paper and screening of the slides under the microscope for the technical adequacy and preliminary diagnostic impression, particularly concerning the presence of atypia in the cells and possible neoplasia were done. Then the slides were immediately evaluated and cross checked by chief guide/co- guides from department of pathology particularly concerning the presence of atypia in the cells and possible neoplasia and the FNAC was repeated in cases of inadequate smears. Now the adequacy, cytomorphology, intensity of Toluidine blue stain preparations was interpreted, documented in the cytology requisition form and were compared later on with conventional Papanicolaou stained smears. On site assessment and evaluation of cellularity of Toluidine Blue stained FNAC samples. Study morphology and background of Toluidine blue stain FNAC samples. Study staining intensity of Toluidine blue stain. Sensitivity, specificity, Negative Predictive Value (NPV) and Positive Predictive Value (PPV) of Toluidine Blue stained FNAC smear in comparison to Pap stain. The collected data was entered in Microsoft Office Excel software 2013. Data analysis was done by using SPSS (Statistical Package for Social Sciences) 11.0 version for statistical analysis. Data was appropriately coded with alpha numeric code. The data were collected onsite and checked after every 10-day entry. For Descriptive Statistics Percentage (%), ratio, mean and standard deviation were calculated along with graphical and tabular presentations were made. For inferential statistics McNemar Test and proportion test were used to find out the significant association between the variables. For diagnostic measurement sensitivity, specificity, positive predictive value, negative predictive value and diagnostic accuracy were calculated. Probability of significance was set at 5% level. According to the study, done by [15], the truly positive diagnosed cases of FNAC samples by Toluidine blue stain has been reported as 78% considering.
Proportion of truly diagnosis (P) = 78%
Complement of P (Q) = 100-P = 22%
Permissible error (L) = 15% of P
= 11.7%
Z alpha at 95% confidence interval= 1.96
Now, using the formula,
Sample size = Z²xPxQ/ L²
= ((1.96) ² x78x22)) / (11.7) ²
=48.156 i.e., 48
Adding, 10 % for non- response, 48+5 = 53 (Any number of samples exceeding the expected sample size will be included in the study).
- RESULTS & DISCUSSION
Table 01: Age categorical distribution of cases
| Age in years | Frequency | Percentage (%) |
| <= 10 | 8 | 12.7 |
| 11-20 | 10 | 15.9 |
| 21-30 | 15 | 23.8 |
| 31-40 | 12 | 19.04 |
| 41-50 | 5 | 7.9 |
| 51-60 | 5 | 7.9 |
| 61-70 | 1 | 1.59 |
| 71-80 | 5 | 7.9 |
| 81-90 | 2 | 3.17 |
| Total | 63 | 100 |
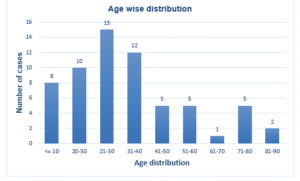
Figure 01: Age categorical distribution of cases
Table 02: Calculation of Mean and standard deviation
| Age in years | |
| Maximum | 90 |
| Minimum | 1 |
| Mean | 34.85 |
| Standard Deviation | 20.976 |
In this study, among all the patients, 45 (73.8) were females and 16 (26.2%) were males with ratio of Male: Female (M: F) = 1:2.8.
Table 03: Gender wise distribution of the patient
| Gender | Frequency | Percentage |
| Male | 16 | 26.2 |
| Female | 45 | 73.8 |
| Total | 61 | 100 |
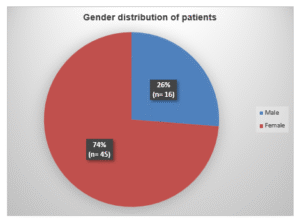
Figure 02: Gender wise distribution of the patients
Among 61 cases studied, the most common site of aspiration was cervical Lymph node with frequency of 25 (41%) followed by breast lump 16 (26.2%) followed by ‘others’ swelling Site wise distribution.
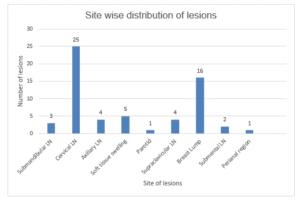
Figure 03: Site wise distribution of lesions (n=61)
Of the 61 cases included in the study, among 38 cases of lymph node, 5 (13.1%) cases, 1 (6.25%) case out of 16 cases of breast lump and 1(20%) case of soft tissue swelling out of total 5 cases were attempted twice onsite due to inadequate cellularity after screening the slides for adequacy on toluidine blue stained smears.
Table 04: Number of attempts of FNAC onsite
| Sr. No | Site | Total number of cases | Number of cases with inadequate material on first attempt onsite | Number of FNAC attempted onsite for adequate material |
| 1. | Lymph Node | 38 (100%) | 5(13.15) | 2 (Twice) |
| 2 | Breast | 16 (100%) | 1 (6.25%) | 2 (Twice) |
| 3. | Soft TIissue | 5 (100%) | 1 (20%) | 2 (Twice) |
| 4. | Parotid | 1 (100%) | 0 | 1 |
| 5. | Perianal Scar | 1 (100%) | 0 | 1 |
| TOTAL | 61 (100%) | 7 (7%) |
Total 7 (11.4%) cases were inadequate on first attempted FNAC shown by Toluidine Blue stained smears. The cases were attempted twice in the same sitting. On second attempt of FNAC, previously inadequate samples in Toluidine Blue stain showed adequate material. On Toluidine blue staining, total number of 61 cases were broadly divided into neoplastic and non-neoplastic lesions. Non neoplastic lesions comprise of 39 (64%) cases and neoplastic lesions comprise of 22 (36.06%) cases.
Table 05: Distribution of lesions on Toluidine Blue stain
| Nature of lesion | Frequency | Percentage (%) |
| Neoplastic | 22 | 36.06 |
| Non-Neoplastic | 39 | 64 |
| Total | 61 | 100 |
On Pap staining, total of 61 cases was broadly divided into non-neoplastic and neoplastic lesions. Non- neoplastic lesions comprise of 41 (67.2%) cases and neoplastic lesions comprise of 20 (32.7%) cases.
Table 06: Distribution of lesions on PAP stain
| Nature of lesion | Frequency | Percentage (%) |
| Neoplastic | 20 | 32.7 |
| Non-Neoplastic | 41 | 67.2 |
| Total | 61 | 100 |
Of the 61 cases included in study, Toluidine blue staining (TBS) was adequate in all 61 cases (100%) because the smear was reaspirated on site after screening the slides for cellularity. Papanicolaou stain had 7 (11.47%) inadequate cellularity on smears and underwent repeat FNAC on next visit. Inadequacy was mainly seen in lymph node, breast and soft tissue. Out of 38 lymph node cases, 5 (13.1%) cases and out of 16 breast cases, 1(6.25%) case showed inadequate cellularity. Similarly, out of 5 soft tissue cases, 1(20%) showed inadequate cellularity in Papanicolaou. The average time taken to screen the slides and identifying the preliminary diagnosis using rapid onsite toluidine blue stain was found to be approximately less than 2 minutes after performing FNAC.
Table 07: On site assessment and evaluation of cellularity of Toluidine blue stained FNAC samples
| S.NO | SITE | TOLUIDINE BLUE
STAIN |
PAPANICOLAOU STAIN | TOTAL
N (%) |
||
| Adequate | Inadequate | Adequate | Inadequate | |||
| 1. | Lymph Node | 38(100%) | 0 | 33(86.8%) | 5(13.1%) | 38(62.29) |
| 2. | Breast | 16(100%) | 0 | 15(93.75%) | 1(6.25%) | 16(26.2%) |
| 3. | Parotid region | 1(100%) | 0 | 1 (100%) | 0 | 1(1.6%) |
| 4. | Soft Tissue | 5 (100%) | 0 | 4 (80%) | 1(20%) | 5(8.19%) |
| 5. | Perianal scar | 1 (100%) | 0 | 1(100%) | 0 | 1(1.6%) |
| Total: | 61(100%) (100%) | 53
(86.8%)
|
7
(11.47%) |
61(100) | ||
On Toluidine blue staining, among 38 cases of lymph nodes, 34(89.4%) showed preserved cell morphology while 4 (10.5%) cases cell morphology was not preserved. Similarly, out of 16 total breast cases, 14 (87.5%) showed preserved cell morphology and (12.5%) cases cell morphology was not preserved. However, 1 (100%) case of parotid region swelling, 5 (100%) cases of soft tissue swelling and 1 (100%) case of perianal scar area swelling showed preserved cell morphology. On Papanicolaou staining, among 38 cases of lymph nodes, 35(92.1%) showed preserved cell morphology while cell morphology of 3 (7.8%) cases was not preserved. Similarly, out of 16 total breast cases, 14 (87.5%) showed preserved cell morphology and cell morphology of 2 (12.5%) cases was not preserved. However, 1 (100%) case of parotid region swelling, 5 (100%) cases of soft tissue swelling and 1 (100%) case of perianal scar area swelling showed preserved cell morphology. Therefore, among total 61 cases in the study, Toluidine blue staining showed preserved cell morphology in 55 (90.1%) cases and cell morphology of 6 (9.8%) cases was not preserved. Hence, among total 61 cases in the study, Papanicolaou staining showed preserved cell morphology in 56(91.8%) cases and cell morphology was not preserved in 5 (8.1%) cases.
Table 08: Cell Morphology
| Sr.NO | SITE | TOLUIDINE BLUE | PAPANICOLAOU | TOTAL | ||
| Preserved
N (%) |
Not preserved
N (%) |
Preserved
N (%) |
Not preserved
N (%) |
|||
| 1. | Lymph Node | 34(89.4%) | 4(10.5%) | 35(92.1%) | 3(7.8%) | 38(62.29%) |
| 2. | Breast | 14(87.5%) | 2(12.5%) | 14(87.5%) | 2(12.5%) | 16(26.2%) |
| 3. | Parotid region | 1(100%) | 0 | 1(100%) | 0 | 1(1.6%) |
| 4. | Soft Tissue | 5(100%) | 0 | 5(100%) | 0 | 5(8.1%) |
| 5. | Perianal area scar | 1(100% | 0 | 1(100%) | 0 | 1(1.6%) |
| TOTAL | 55(90.1%) | 6(9.8%) | 56(91.8%) | 5(8.1%) | 61 (100%) | |
McNemar test showed that discordant pairs (b and c) are equal. So, we do not reject the null hypothesis, H0 b=c (p value 0.12). The agreement of Preservation of quality of Cell morphology is strongly associated in between Toluidine blue stained smears and Papanicolaou stained smears and there is no significant difference in preservation of cell morphology between these two-staining technique.
Table 09: McNemar Test
| PAPANICOLAOU | Total | P value | ||||
| 0.125* | ||||||
| Preserved | Not Preserved | |||||
| TOLUIDINE BLUE | Preserved | 53(a) | 1 (b) | 54 | ||
| Not Preserved | 6 (c) | 1(d) | 7 | |||
| Total | 59 | 2 | 61 | |||
| * McNemar test | ||||||
Among 38 cases of lymph node, Toluidine Blue staining showed crisp chromatin in 30 (79%) cases and smudge chromatin in 8 (21.05%) cases. Similarly, among 16 cases of breast lump,14 (87.5%) cases showed crisp chromatin while 2 (40%) cases showed smudge chromatin.1 (100%) case of parotid region swelling showed crisp chromatin. Among 5 cases of soft tissue swelling 3 (60%) cases showed crisp chromatin while 2 (40%) cases showed smudge chromatin. Similarly, 1 (100%) case of perianal scar region aspirate showed smudge chromatin. Among 38 cases of lymph node, Papanicolaou staining showed crisp chromatin in 19 (50%) cases and smudge chromatin in 19(50%) cases. Similarly, among 16 cases of breast lump, 9 (56.2%) showed crisp chromatin while 7(43.7%) showed smudge chromatin. Similarly, 1 (100%) case of parotid region swelling showed smudge chromatin. Out of 5 cases of soft tissue swelling 1 (20%) case showed crisp chromatin while 4 (80%) cases showed smudge chromatin. Similarly,1 (100%) case of perianal scar region aspirate showed crisp chromatin. Therefore, among a total of 61 total cases in the study, Toluidine blue stained smears showed 48(79%) crisp chromatin and 13 (21.3%) smears showed smudge chromatin. Hence, among a total of 61 cases in the study, Papanicolaou staining showed crisp chromatin in 30 (49.1%) cases and smudge chromatin in 31 (51%) cases.
Table 10: Nuclear Morphology
| TOLUIDINE BLUE | PAPANICOLAOU | TOTAL | ||||
| Sr.NO: | Crisp Chromatin | Smudge Chromatin | Crisp Chromatin | Smudge chromatin | ||
| 1. | Lymph Node | 30(79%) | 8(21.05%) | 19(50%) | 19(50%) | 38
(62.2%) |
| 2. | Breast | 14(87.5%) | 2(12.5%) | 9(56.2%) | 7(43.7%0 | 16
(26.2%) |
| 3. | Parotid region | 1(100%) | 0 | 0 | 1(100%) | 1(1.6%) |
| 4. | Soft Tissue | 3(60%) | 2(40%) | 1(20%) | 4(80%) | 5(8.1%) |
| 5. | Perianal area scar | 0 | 1(100%) | 1(100%) | 0 | 1(1.6%) |
| Total No: | 48(79%) | 13(21.3%) | 30(49.1%)
|
31(51%) | 61
(100%) |
|
McNemar Test showed that discordant pairs (b and c) are not equal. So, we reject the null hypothesis, H0 b ≠ c (p value 0.01). The agreement in quality of the nuclear chromatin is not strongly associated in between toluidine blue stained and Papanicolaou stained smears and has significant differences between them.
Table 11: McNemar Test
| PAPANICOLAOU | Total | P value | ||||
| 0.01 | ||||||
| Crisp chromatin | Smudgy chromatin | |||||
| TOLUIDINE BLUE | Crisp Chromatin
|
26 (a)
|
19 (b)
|
45 | ||
| Smudgy Chromatin
|
6 (c)
|
10 (d)
|
16 | |||
| Total | 32 | 29 | 61 | |||
| * McNemar test | ||||||
On Toluidine Blue staining, among 38 cases of lymph node, 36 (95%) cases showed clean background while 2 (5.2%) cases showed hemorrhagic background. Similarly, 16 (100%) cases of breast lump,1 (100%) case of parotid region swelling, 5 (100%) cases of soft tissue swelling and 1 (100%) case of perianal area scar aspirates showed clean background. On Papanicolaou staining, among 38 cases of lymph nodes, 5 (13.1%) showed clean background while 33 (87%) showed hemorrhagic background. Similarly, 1(100%) case from parotid region swelling, 5 (100%) cases from soft tissue swelling and 1 (100%) case of perianal area scar aspirate showed hemorrhagic background. Therefore, out of 61 total cases in the study, Toluidine Blue staining showed clean background in 59 (97%) cases and hemorrhagic background in 2(3.27%) cases only. Out of 61 total cases in the study, Papanicolaou staining showed clean background in 7(11.4%) cases only and hemorrhagic background in 54 (88.5%) cases.
Table 12: Background Staining
| Sr. No | SITE | TOLUIDINE BLUE | PAPANICOLAOU | Total | ||
| Clean | Hemorrhagic | Clean | Hemorrhagic | |||
| 1. | Lymph Node | 36(95%) | 2(5.2%) | 5(13.1%) | 33(87%) | 38(100%) |
| 2. | Breast | 16(100%) | 0 | 2(12.5%) | 14(87.5%) | 16(100%) |
| 3. | Parotid region | 1(100%) | 0 | 0 | 1(100%) | 1(100%) |
| 4. | Soft Tissue | 5(100%) | 0 | 0 | 5(100% | 5(100%) |
| 5. | Perianal area scar | 1(100%) | 0 | 0 | 1(100%) | 1(100%) |
| Total No: | 59(97%)
|
2(3.27%) | 7(11.4%)
|
54(88.5%) | 61 (100%) | |
McNemar Test showed that discordant pairs (b and c) are not equal. So, we reject the null hypothesis, Ho b ≠ c (p value 0.0 01). The agreement in quality of background staining is not strongly associated in between toluidine blue stained and Papanicolaou stained smears and has significant differences between them.
Table 13: McNemar Test:
| PAPANICOLAOU | Total | P value | ||||
| 0.01 | ||||||
| Clean background | Hemorrhagic background | |||||
| TOLUIDINE BLUE | Clean background
|
7 (a)
|
52 (b)
|
59 | ||
| Hemorrhagic background
|
1 (c)
|
1 (d)
|
2 | |||
| Total | 8 | 53 | 61 | |||
| * McNemar test | ||||||
On Toluidine Blue staining, among 38 lymph node cases, 14 (36.8%) showed atypical cells/ neoplastic cells and 24 (63.5%) showed no atypicality’s. Similarly, out of 16 cases of breast lump, 2 (12.5%) cases showed atypical cells and 14 (87.5%) cases showed no atypicality’s and 1 (100%) case of parotid region swelling also showed no atypical cells. Similarly, 5 (100%) FNAC cases of soft tissue and 1 (100%) case of perianal scar aspirate case showed no atypicality’s/atypical cells. On Papanicolaou staining, among total 38 lymph node cases, 11 (28.9%) cases showed atypical cells/ neoplastic cells and 27 (71.5%) cases showed no atypicality’s. Similarly, out of 16 cases of breast lump, 2 (12.5%) cases showed atypical cells and 14 (87.5%) cases did not show atypicality’s in the cells. Similarly, 1 (100%) case of parotid region swelling also did not show atypicality’s/atypical cells and 5 (100%) cases of soft tissue swelling and 1 (100%) case of perianal scar aspirate showed atypical cells. Therefore, out of 61 total cases included in the study, Toluidine Blue staining showed atypical/neoplastic cells in 22 (36.05%) cases and lacks atypical cell or showed non-neoplastic cells in 39 (64%) cases. Similarly, out of 61 total cases included in the study, Papanicolaou staining showed atypical/neoplastic cells in 19 (31.1%) cases and lacks atypical cell or showed non-neoplastic cells in 42 (69%) cases.
Table 14: Atypical cells / Atypicality
| S.NO: | SITE | TOLUIDINE BLUE STAIN | PAPANICOLAOU STAIN | TOTAL | ||
| Atypical cells seen | Atypical cells not seen | Atypical cells seen | Atypical cells not seen | |||
| 1. | Lymph Node | 14(36.8%) | 24(63.5%) | 11(28.9%) | 27(71.5%) | 38 (62.2%) |
| 2. | Breast | 2(12.5%) | 14(87.5%) | 2(12.5%) | 14(87.5%) | 16 (26.2%) |
| 3. | Parotid region | 0 | 1(100%) | 0 | 1(100%) | 1(1.6%) |
| 4. | Soft Tissue | 5(100%) | 0 | 5(100%) | 0 | 5(8.1%) |
| 5. | Perianal area scar | 1(100%) | 0 | 1(100%) | 0 | 1(2%) |
| Total No | 22(36.06%) | 40(39.6%) | 19(31.1%) | 42(69%) | 61 (100%) | |
Table 15: 2×2 contingency table
| PAPANICOLAOU | Total | |||
| Atypical cells seen | Atypical cells not seen | |||
| TOLUIDINE BLUE | Atypical cells seen | 19(a) | 3 (b) | 22 |
| Atypical cells not seen | 0 (c) | 39 (d) | 39 | |
| Total | 19 | 42 | 61 | |
Sensitivity of Toluidine Blue stained smears = (True positive/ True positive + False negative) ×100%
= (19/19+0) × 100%
= 100%
Specificity of Toluidine Blue stained smears = (True negative/ True negative + False positive) × 100%
= (39/39+3) × 100%
= 92.8%
Positive Predictive Value (PPV) of Toluidine Blue stained smears = (True positive/ True positive + False positive) × 100%
= (19/19+3) × 100%
= 86.36%
Negative predictive Value (NPV) of Toluidine Blue stained smears = (True negative/ False negative +True negative) × 100%
= (39/0+39) × 100%
= 100%
Diagnostic Accuracy= (True positive + True negative) /All cases
= (19+39)/61 × 100%
= 95.08%
McNemar Test showed that discordant pairs (b and c) are equal. So, we do not reject the null hypothesis, H0 b=c (P value= 0.25). The agreement of atypical cells/atypicality’s seen are strongly associated in between onsite Toluidine blue stained findings and gold standard Papanicolaou stained smears findings and there is no difference in the identification of atypical cells between these two stains. However, the average time taken to screen the slides for identifying atypicality’s using rapid onsite toluidine blue stain was found to be approximately less than 2 minutes after performing FNAC.
Table 16: McNemar Test
| PAPANICOLAOU | Total | P value | ||||
| 0.25* | ||||||
| Atypical cells seen | Atypical cells not seen | |||||
| TOLUIDINE BLUE | Atypical cells seen
|
19(a)
|
3 (b)
|
22 | ||
| Atypical cells not seen
|
0 (c)
|
39 (d)
|
39 | |||
| Total | 19 | 42 | 61 | |||
| * McNemar test | ||||||
Table 17: Comparison of various statistical parameters in various studies with the present study
| Various studies | Sensitivity | Specificity | PPV | NPV | Diagnostic accuracy |
| [11] | 100% | 97.2% | – | – | – |
| [19] | 100% | 97% | 27.2% | 97.1% | 100% |
| [16] | 94% | 68% | 75% | 94% | – |
| [20] | 97% | 90% | 91% | 96% | – |
| [25] | 98% | 100% | 100% | 99.8% | 99.2% |
| Current study | 100% | 92.8% | 86.36% | 100% | 95.08% |
DISCUSSION
Fine Needle Aspiration Cytology (FNAC) is a simple, minimally invasive, cost-effective technique for examining superficial and deep swellings in various anatomical locations [1,2]. Its importance has risen as an adjunct to clinical, radiological and laboratory data for better patient prognosis [6]. Despite its popularity, FNAC has limitations including unsatisfactory or non-diagnostic smears causing patient stress. Inadequacy results from cell inspissation in needle lumen, inexperienced technique causing cell distortion, and clotting affecting cellular morphology and stromal component relationship [6]. Adequate aspiration and good staining background are necessary for accurate diagnosis. Rapid on-site evaluation and reaspiration of inadequate samples at first visit limits visit number [7]. Every aspiration should undergo adequacy evaluation [3]. Rapid on-site evaluation (ROSE) determines sample adequacy, increases diagnostic yield, aids specimen triage for ancillary studies, and helps determine preliminary diagnosis in emergencies [3,11]. Quick staining methods for ROSE include diff quik, toluidine blue (TB), brilliant cresyl blue (BCB), ultra-fast Pap stains, and rapid H&E [11]. This study employed Toluidine Blue—an easily available, cost-effective supravital stain used in hematology for reticulocyte count. Mean age was 34.85 years with highest cases in 21-30 years (23.84%) followed by 31-40 years (19.04%). Saba K et al showed mean ages of 32.08 and 31.08 years, concordant with this study [6,13]. One reason may be reactive lymph node conditions affecting these age groups. Agrawal P et al showed mean age of 45 years, possibly due to their larger sample size [11]. Gender distribution showed 45 females and 16 males (M:F ratio 1:1.28; 73.8% and 26.2% respectively). Most common site was cervical lymph nodes 25 cases (41%) followed by breast 16 cases (26.2%), concordant with Saba K et al showing 78.9% cervical LN and 18.5% breast [6], and Agrawal P et al showing 63 (31.5%) lymph node and 40 (20%) breast cases [11]. This reflects wide lymph node distribution, easy accessibility for examination, female predominance, and reproductive age group predilection for breast lumps. Of 61 cases, 7 (11.47%) showed inadequate material on first attempt by Toluidine Blue: 5 (13.1%) lymph nodes, 1 (6.25%) breast, and 1 (20%) soft tissue. Repeat FNAC showed adequate material in all 7, allowing first-visit management decisions in 100% cases. A 1500-case study showed lymph node as commonest inadequacy site with 2% inadequate on TB, Giemsa and PAP, achieving 98% first-visit decisions with two passes [16]. Another 200-patient study showed 28 (14%) unsatisfactory on first attempt: 16 (38%) of 42 thyroid, 10 (10.4%) of 96 breast, and 2 (3.2%) of 62 lymph node cases, with repeat FNAC providing adequate material in 24 (12%), enabling 98% first-visit decisions [8]. Aspirate adequacy was evaluated on-site with inadequate samples reaspirated within 2 minutes. Toluidine Blue achieved 61 (100%) adequate samples after reaspirating the 7 initial inadequate cases. Papanicolaou showed 7 (11.47%) inadequate. Studies showed 100% TB adequacy versus 84-95% Papanicolaou [6,11], and 98-100% TB adequacy [17,18]. ROSE minimizes unsatisfactory samples and false negatives. Parameters evaluated were cell morphology, nuclear features, background staining and atypical cells using visual assessment and McNemar Test. TB showed preserved cell morphology in 55 (90.1%) versus Papanicolaou 56 (91.8%) cases (p=0.125, insignificant). Studies confirmed TB cell morphology equals Papanicolaou [5,12], though one found TB slightly inferior [13]. Quality index scoring systems were used in other studies [11,16]. TB showed crisp chromatin in 48 (79%) versus Papanicolaou 30 (49.1%) cases. TB’s high DNA affinity enhances nuclear absorption, making tumor cell staining prominent in dysplastic/anaplastic cells [19]. Studies showed 84% crisp chromatin with TB, concluding excellent cytological details [11,14], though one found TB less superior to Papanicolaou [13]. Another found TB nuclear staining equally good [12]. Variations may reflect stain preparation, fixation differences, subjective scoring, and inter-observer variation. This study used only visual assessment without scoring systems. TB showed clean background in 59 (97%) versus Papanicolaou 7 (11.4%) cases (p=0.00, significant). RBCs stain faintly with TB without interfering with cellular elements [20]. Two hemorrhagic TB cases likely resulted from using four-day-old stain versus freshly prepared. One study showed Rapid PAP superior background (77.5%) versus TB (33%) [11] but concluded TB most cost-effective, quick, least labor-intensive, and reliable for ROSE, especially in resource-poor settings. TB showed atypical/neoplastic cells in 22 (36.05%) versus Papanicolaou 19 (31.1%) cases. Studies showed difficulty diagnosing 20 (20.8%) TB cases as three-dimensional clusters were misinterpreted as neoplastic and degenerated cells distorted during smearing [16]. Similarly, three lymph node cases showed atypical cells on TB but were non-neoplastic on Papanicolaou. Cytomorphological diagnosis showed no significant difference between non-neoplastic and neoplastic lesions. TB identified 39 (64%) non-neoplastic and 22 (36.06%) neoplastic cases. Papanicolaou showed 19 (31.1%) non-neoplastic and 42 (69%) neoplastic cases.
- CONCLUSIONS
This hospital-based prospective study was conducted in the Cytopathology Lab, Department of Pathology, BPKIHS, Nepal to assess the utility of Toluidine Blue as a rapid staining technique in FNAC and compare its quality with Papanicolaou stained smears based on cell morphology, nuclear features, background and atypicality. Of 61 enrolled cases, Toluidine Blue achieved 100% adequacy through on-site reaspiration, while Papanicolaou showed 7 (11.47%) inadequate cases requiring repeat FNAC on next visit. Cell morphology was preserved in 55 (90.1%) TB versus 56 (91.8%) Papanicolaou cases. TB showed crisp chromatin in 48 (79%) versus 30 (49.1%) Papanicolaou cases. TB showed clean background in 59 (97%) versus 7 (11.4%) Papanicolaou cases. TB identified atypical/neoplastic cells in 22 (36.05%) versus 19 (31.1%) Papanicolaou cases, with 3 lymph node cases misclassified as neoplastic on TB but non-neoplastic on Papanicolaou. Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Diagnostic Accuracy of Toluidine Blue were 100%, 92.8%, 86.36%, 100% and 95.08% respectively. Nuclear morphology and background staining were slightly superior on TB (p=0.01 and p=0.00 respectively). Screening time was under 2 minutes, reducing delays in diagnosis and treatment. Papanicolaou stain requires 30 minutes and full laboratory setup, while TB requires only Toluidine Blue reagent, glass slide, coverslip, distilled water and 95% ethanol. Though Papanicolaou remains the gold standard, Toluidine Blue is a superior option for on-site adequacy assessment and serves as an effective screening technique, particularly in resource-poor settings.
REFRENCES
- Pathology Md. Supravital Stained Wet Mount Study Of Fine Needle Aspirates – As A Rapid Supplementary Diagnostic Procedure A Dissertation submitted to the In partial fulfillment of the requirements for the award of degree.
- Sofi LA, Sherwani RK, Hasan M, et al. On-spot brilliant cresyl blue staining in fine needle aspiration, a novel technique for cytological diagnosis. Acta Cytol 2013; 57: 641–645.
- S P, K V, S A. Utility of rapid brillant cresyl blue stained wet mount preparation in routine fine needle aspiration cytology. IP Arch Cytol Histopathol Res 2020; 5: 63–69.
- Orell SR. Pitfalls in fine needle aspiration cytology. Cytopathology 2003; 14: 173–182.
- Sumathy C SDJ. Supravital Stained Rapid Wet Mount Preparation of Fine Needle Aspirates – A Cytomorphological Study. tejms 2012; 63: 62–66.
- Saba K, Sajjad Y, et al. Role of toluidine blue staining, to reduce the non diagnostic reporting of fine needle aspiration cytology. Biomedical 2016; 32: 198–205.
- Alsohaibani F, Girgis S, Sandha GS. Does onsite cytotechnology evaluation improve the accuracy of endoscopic ultrasound-guided fine-needle aspiration biopsy? Can J Gastroenterol 2009; 23: 26–30.
- Ammanagi AS, Dombale VD, Patil SS. On-site toluidine blue staining and screening improves efficiency of fine-needle aspiration cytology reporting. Acta Cytol 2012; 56: 347–351.
- Wohlschläger J, Darwiche K, Ting S, et al. ‘Rapid on-site evaluation’ (ROSE) in der zytologischen Diagnostik von Lungen- und Mediastinalerkrankungen. Pathologe 2012; 33: 308–315.
- Nasuti JF, Gupta PK, Baloch ZW. Diagnostic value and cost-effectiveness of on-site evaluation of fine-needle aspiration specimens: Review of 5,688 cases. Diagn Cytopathol 2002; 27: 1–4.
- Agarwal P, Toi PC, Subramaniam H, et al. Prospective comparison of cytological specimen adequacy assessment by different rapid staining techniques for rapid on-site evaluation in fine needle aspiration cytology and their cost-effectiveness. Diagn Cytopathol 2019; 47: 469–474.
- Patil P V, Nikumbh DB. Efficacy of toluidine blue staining in cervicovaginal cytology over conventional papanicolaou stain. IP Arch Cytol Histopathol Res 2018; 3: 47–51.
- Saba K, Niazi S, Bukhari MH, et al. Use of supravital toluidine blue staining to improve the efficiency of fine-needle aspiration cytology reporting in comparison to papanicolaou stain. Pakistan J Med Sci 2015; 31: 1146–1151.
- Hewer E, Schmitt AM. Ultrafast Toluidine Blue Staining for Rapid On-Site Evaluation of Cytological Smears. Acta Cytol. Epub ahead of print 2020. DOI: 10.1159/000505254.
- Jayasinghe RD, Hettiarachchi PVKS, Amugoda D, et al. Validity of Toluidine Blue test as a diagnostic tool for high risk oral potentially malignant disorders- a multicentre study in Sri Lanka. J Oral Biol Craniofacial Res 2020; 10: 547–551.
- Veena Raja. Diagnostic accuracy of rapid supravital stain in comparison with conventional stain in breast cytology. April 2018; 541–548.
- Selhi PK, Tyagi R, Bansal P, et al. Hepatic fine-needle aspiration cytology: The role of rapid on-site evaluation in the assessment of hepatic lesions. Turkish J Gastroenterol 2018; 29: 442–447.
- Shield PW, Cosier J, Ellerby G, et al. Rapid on-site evaluation of fine needle aspiration specimens by cytology scientists: A review of 3032 specimens. Cytopathology 2014; 25: 322–329.
- Junaid M, Choudhary MM, Sobani ZA, et al. A comparative analysis of toluidine blue with frozen section in oral squamous cell carcinoma. World J Surg Oncol 2012; 10: 1–5.
- Gupta A, Singh M, Ibrahim R, et al. Utility of toluidine blue staining and brush biopsy in precancerous and cancerous oral lesions. Acta Cytol 2007; 51: 788–794.
Publication History
Submitted: July 23, 2025
Accepted: August 11, 2025
Published: August 30, 2025
Identification
D-0487
DOI
https://doi.org/10.71017/djmi.4.8.d-0487
Citation
Acharya Barsha, Smriti Karki, Anju Pradhan & Punam Paudyal (2025). Utility of Supravital Toluidine Blue Stain as Rapid Staining Technique in Fine Needle Aspiration Cytology. Journal of Medical Innovations, 4(08):542-566.
Copyright
© 2025 The Author(s).