

")
Publication History
Submitted: December 04, 2021
Accepted: December 20, 2021
Published: January 01, 2022
Identification
D-0090
Citation
Humza Sohail, Markus Peter Chan & Umaima Nagari (2022). Myocarditis after receiving the Covid-19 Vaccine in an Enormous Medical Facility. Dinkum Journal of Medical Innovations, 1(01):07-12.
Copyright
© 2022 DJMI. All rights reserved
07-12
Myocarditis after receiving the Covid-19 Vaccine in an Enormous Medical FacilityOriginal Article
Humza Sohail 1*, Markus Peter Chan 2, Umaima Nagari 3
- King Edward Medical University, Pakistan; hamza@gmail.com
- China Medical University, Taiwan; markus-chan8987@cmu.edu.tw
- Fatima Jinnah Medical University, Pakistan; umaimanigari9r5@fjmu.edu.pk
*Corresponding author: sohail.hamza@gmail.com
Abstract: A messenger RNA (mRNA) vaccine against coronavirus illness 2019 has been associated in publications with myocarditis; however, the incidence and consequences of myocarditis after immunization have not been fully investigated. We searched the Medical Companies database, the largest healthcare organization in Israel, for myocarditis symptoms in people who had at least one dose of the BNT162b2 mRNA vaccine (Pfizer-BioNTech). To diagnose myocarditis, heart specialists used the precise description provided by the Centers for Disease Control and Prevention (CDC). We compiled the appearance, course of treatment, and prognosis from the patient’s digitized medical record. We used a Kaplan-Meier analysis to track the incidence of myocarditis up to 42 days after the vaccine’s initial administration. Overall, 76% of myocarditis patients had mild cases, 22% had intermediate cases, and one case had cardiogenic shock along with it. The BNT162b2 mRNA immunization was estimated to have been administered to 2.13 cases per 100,000 individuals attending a large medical center; male patients between the ages of 16 and 29 had the highest prevalence. The bulk of instances of myocarditis were moderately to mildly severe.
Keywords: myocarditis, covid-19 vaccination, medical facility
- INTRODUCTION
On December 20, 2020, a national campaign was launched in Israel to deliver the BNT162b2 messenger RNA (mRNA) vaccine (Pfizer–BioNTech) against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). As of May 5, 2021, 54.6% of Israelis have obtained all recommended vaccinations, while 58.2% of the population had received at least one dosage [1]. Concerning a potential connection between vaccination against coronavirus disease 2019 (Covid-19) and myocarditis, the Centers for Disease Control and Prevention (CDC) released a statement on May 27, 2021, for both the BNT162b2 and the mRNA-1273 vaccine (Moderna) [2]. The Israeli Ministry of Health announced on June 2, 2021, that during the period from December 2020 to May 2021, or roughly when the immunization program started, 148 cases of myocarditis had been found in Israel. A potential correlation between the second vaccination dosage and myocarditis in male patients aged 16 to 30 years was observed in the report [3]. More recently, Israeli researchers found that immunization increased the 42-day risk of myocarditis by a factor of 3.24 when compared to the risk among those who were not vaccinated, with the majority of cases occurring in young male patients [4]. After receiving the BNT162b2 mRNA vaccine, we assessed the incidence of myocarditis in one health care organization (HCO) in Israel. Based on a review of patient charts, we also reported the clinical course and severity of the condition.
- METHODOLOGY
The database of Health Services, the biggest HCO in Israel, served as the study’s foundation. Care for 4.7 million patients (52% of the total population) is provided by this health care system, whose membership is roughly representative of the Israeli community in terms of socioeconomic position and the frequency of comorbid disorders [5]. While both in-network and out-of-network hospitals offer inpatient care, the organization handles patients’ outpatient needs. A previous description of the database we used for this investigation may be found here [6]. The Israeli Ministry of Health collects and shares daily all information related to SARS-CoV-2 immunization, testing, and diagnosis in a centralized manner with medical professionals. The institutional review board gave their approval to the study. The study was exempt from obtaining patients’ written informed consent because it was based on retrospective data. The data was gathered and the study was designed by the authors. We assessed patients who were enrolled in Health Services and received vaccinations between December 20, 2020, and May 24, 2021, in this retrospective analysis. From electronic health data, we were able to identify possible cases of myocarditis that had happened 42 days after the first dosage of the vaccination. In order to provide for around 21 days of follow-up following each of the two vaccination doses, a follow-up duration of 42 days following the first dose was selected. The patient’s electronic health record was examined in order to determine the validity of each suspected case. The case definition was first created in 2003 to be used in calculating the frequency of illnesses following smallpox vaccination [7-9]. Patients were monitored for 42 days following immunization in order to calculate the incidence of myocarditis. Patients’ data were censored in the event of unrelated cause death, HCO membership cancellation, or trial period end (May 24, 2021). Only 0.01% of the patients experienced mortality, so a competing-risks analysis was not carried out. In order to calculate the cumulative incidence of myocarditis, we used the Kaplan–Meier technique. Means (±SD) were used to summarize continuous data, while counts (percentages) were used to summarize categorical variables.
- RESULTS AND DISCUSSION
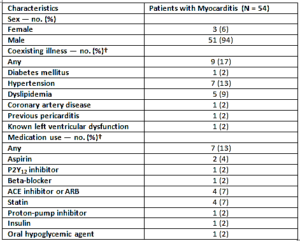
94% of patients received two treatments between December 2020 and May 2021. In the 42 days following the initial vaccination dose, 159 possible instances of myocarditis were first found using ICD-9 codes. 54 of these instances were found to have satisfied the study criteria for a myocarditis diagnosis after adjudication. Of these, 41 cases were deemed to be of mild severity, 12 of intermediate severity, and 1 of fulminant severity. There were records of all the patients who had been suspected of having myocarditis in the community. For 55 out of 81 prospective cases (68%) that were not recoding events and for 38 out of 54 cases (70%) that satisfied the study criteria, discharge summaries from the index hospitalization were available. Table 1 lists the medical characteristics of the myocarditis patients. Ninety-four percent of the patients were men and boys, with a median age of 27. Prior to receiving the vaccination, two patients—125 and 186 days earlier, respectively—had developed Covid-19. Of the patients, 13% were undergoing treatment for chronic disorders, whereas the majority (83%) had no comorbid medical issues. Prior to vaccination, one patient experienced modest left ventricular dysfunction. More information is provided below:
Table 1: Characteristics of study population
Per 100,000 vaccinated individuals, the estimated overall incidence of myocarditis within 42 days of receiving the first dose was 2.13 cases (95% confidence interval [CI], 1.56 to 2.70), with an incidence of 4.12 (95% CI, 2.99 to 5.26) among patients who were male and 0.23 (95% CI, 0 to 0.49) among those who were female. For mild myocarditis, the incidence per 100,000 people was 1.62 (95% CI, 1.12 to 2.11), for intermediate myocarditis, it was 0.47 (95% CI, 0.21 to 0.74), and for fulminant myocarditis, it was 0.04 (95% CI, 0 to 0.12) (Table 2).
Table 2: Incidence of Myocarditis

Table 3 displays the clinical and laboratory characteristics of myocarditis. Chest pain was the initial symptom in 82% of patients. At admission, most patients had normal vital signs; just one patient had hemodynamic instability, and none of the others needed mechanical circulatory support, inotropic support, or vasopressor support at the time of presentation. Twenty of the 38 patients (53%) whose ECG data were available at the time of admission had ST-segment elevation on the electrocardiogram (ECG); the results of the ECG were normal in 8 of the 38 patients (21%); the remaining patients had minor abnormalities such as T-wave changes, atrial fibrillation, and nonsustained ventricular tachycardia. In 41 patients with accessible data, the median peak troponin T level was 680 ng per liter (IQR, 275 to 2075), while in 28 patients with available data, the median creatine kinase level was 487 U per liter (IQR, 230 to 1193). One patient developed extracorporeal membrane oxygenation due to cardiogenic shock while in the hospital. The other patients did not require mechanical ventilation, inotropic support, or vasopressor assistance. But 3% of patients experienced atrial fibrillation and 5% experienced nonsustained ventricular tachycardia. In total, 65% of the patients were released from the hospital with no further plans for care. The day following their release, a patient with a history of cardiac illness passed away for an undisclosed reason. Three consecutive admissions for recurrent pericarditis were made by a patient with a history of pericarditis who had been hospitalized with myocarditis; there was no additional myocardial involvement following the initial episode (Table 3). In this work, we used a large Israeli health provider database to evaluate the incidence and clinical course of myocarditis following receipt of the BNT162b2 mRNA Covid-19 vaccination. In the 42 days following the initial vaccination dose, we calculated the incidence of myocarditis to be 2.13 instances per 100,000 vaccinated individuals using recognized diagnostic criteria. Patients who were male and between the ages of 16 and 29 had the highest incidence. The majority of patients had mild to moderate severity. Throughout the postvaccination period, myocarditis diagnoses were made; however, there seemed to be a spike in cases about three to five days following the second vaccination dose. After being released from the hospital, one patient with underlying heart disease died of an unidentified cause, while another patient experienced cardiogenic shock. Of the patients with myocarditis who received echocardiography, 29% exhibited initial left ventricular dysfunction; of those who had further testing after being discharged, the left ventricular function had returned to normal. Our results may serve as points of reference, even though we are unable to directly compare the incidence of myocarditis following immunization in our study with the incidence in other investigations. The CDC has estimated that the incidence of myocarditis following any Covid-19 vaccination is 0.48 cases per 100,000 overall and 1.2 cases per 100,000 among vaccine recipients between the ages of 18 and 29 years, based on data from the Vaccine Adverse Events Reporting System [10]. The age of the patients in each research and the various time periods for adverse event identification are two other notable distinctions between the two estimations. An frequency of 8.2 cases of myocarditis per 100,000 male service members (a total of 23 cases) was reported in a report from the U.S. military Covid-19 vaccination campaign. This estimate is roughly twice the number among men of all ages in our study. Compared to 29% in our study, researchers in the military study found left ventricular dysfunction in 17% of the men (all cases in the mild or mild-to-moderate range) [11]. This difference may be due to various coexisting conditions, age groups, and shorter follow-up periods in the military study. According to Barda et al.’s Israeli study [4], for every 100,000 vaccinated individuals, there were an additional 2.7 occurrences of myocarditis. The HCO database that was used in this study was also used in our investigation, however the incidence figures are different. Given that our research’s median age was 44 years (IQR, 30 to 63), the main causes of this discrepancy are the two study groups’ disparate age distributions and the significant age-related heterogeneity of post-vaccination myocarditis. Initially, an endomyocardial biopsy, which was done on a single patient, yields a conclusive diagnosis of myocarditis. Although it matches the way myocarditis is diagnosed in clinical practice, the definition of myocarditis utilized in our study does not establish the diagnosis. Second, cases might have gone unnoticed if the diagnosis hadn’t been recorded in the outpatient medical record or if it had been made in an out-of-network hospital and the insurance hadn’t been notified right after. Furthermore, due to our inability to get information on the index hospitalization or the failure to record certain data in the discharge notes, some myocarditis patients may not have met the research criteria for the diagnosis. These problems would probably cause the incidence of myocarditis to be underestimated. Third, information was lacking for a large number of the clinical course-related factors. Fourth, no conclusions about the relationship between the immunization and the future development of myocarditis can be drawn because there was no concurrent enrollment of a comparator group. Lastly, statistics addressing the occurrence of myocarditis following COVID-19 were not to be collected as part of the study design.
Table 3: Clinical and Laboratory Findings

4-CONCLUSION
A median of 2.13 cases per 100,000 vaccinated individuals and 10.69 cases per 100,000 male patients between the ages of 16 and 29 years old were reported to have myocarditis in the 42 days following receipt of at least one dose of the BNT162b2 mRNA vaccine in this retrospective cohort study, which involved individuals aged 16 or older in a major Israeli health care system. In most cases, the degree of myocarditis was mild to intermediate.
REFRENCES
- Luxenburg, O., Singer, C., Myers, V., Wilf-Miron, R., & Saban, M. (2022). Sociodemographic disparities in COVID-19 burden: changing patterns over four pandemic waves in Israel. J Epidemiol Community Health, 76(7), 653-659.
- Das, B. B., Moskowitz, W. B., Taylor, M. B., & Palmer, A. (2021). Myocarditis and pericarditis following mRNA COVID-19 vaccination: what do we know so far?. Children, 8(7), 607.
- Israel Ministry of Health. (2021). Surveillance of myocarditis (inflammation of the heart muscle) cases between December 2020 and May 2021 (including).
- Barda, N., Dagan, N., Ben-Shlomo, Y., Kepten, E., Waxman, J., Ohana, R., … & Balicer, R. D. (2021). Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. New England Journal of Medicine, 385(12), 1078-1090.
- Barda, N., Dagan, N., Ben-Shlomo, Y., Kepten, E., Waxman, J., Ohana, R., … & Balicer, R. D. (2021). Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. New England Journal of Medicine, 385(12), 1078-1090.
- Rotshild, V., Hirsh Raccah, B., Gazawe, M., & Matok, I. (2022). Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study. Cancers, 14(9), 2344.
- Cohen Castel, O., Dagan, E., Keinan–Boker, L., Low, M., & Shadmi, E. (2021). Patients’ perceived continuity of care and adherence to oral anticancer therapy: a prospective cohort mediation study. Journal of General Internal Medicine, 36, 1525-1532.
- Dagan, N., Barda, N., Kepten, E., Miron, O., Perchik, S., Katz, M. A., … & Balicer, R. D. (2021). BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. New England Journal of Medicine, 384(15), 1412-1423.
- [9] Kociol, R. D., Cooper, L. T., Fang, J. C., Moslehi, J. J., Pang, P. S., Sabe, M. A., … & American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology. (2020). Recognition and initial management of fulminant myocarditis: a scientific statement from the American Heart Association. Circulation, 141(6), e69-e92.
- Wallace, M., & Oliver, S. E. (2021). COVID-19 mRNA vaccines in adolescents and young adults: benefit-risk discussion.
- Montgomery, J., Ryan, M., Engler, R., Hoffman, D., McClenathan, B., Collins, L., … & Cooper, L. T. (2021). Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA cardiology, 6(10), 1202-1206.
Publication History
Submitted: December 04, 2021
Accepted: December 20, 2021
Published: January 01, 2022
Identification
D-0090
Citation
Humza Sohail, Markus Peter Chan & Umaima Nagari (2022). Myocarditis after receiving the Covid-19 Vaccine in an Enormous Medical Facility. Dinkum Journal of Medical Innovations, 1(01):07-12.
Copyright
© 2022 DJMI. All rights reserved