

")
Publication History
Submitted: January 04, 2023
Accepted: January 20, 2023
Published: February 01, 2023
Identification
D-0100
Citation
Muhammad Ayan & Ayesha Pervaiz Cheema (2023). Patients’ Perceptions of Post-Mastectomy Mammary Reconstruction: Contributing Variables. Dinkum Journal of Medical Innovations, 2(02):42-49.
Copyright
© 2023 DJMI. All rights reserved
42-49
Patients’ Perceptions of Post-Mastectomy Mammary Reconstruction: Contributing VariablesOriginal Article
Muhammad Ayan1, Ayesha Pervaiz Cheema 2*
- Lahore Medical and Dental College, Pakistan; ayan89564@gmail.com
- Lahore Medical and Dental College, Pakistan; ayeshacheema@gmail.com
* Correspondence: ayeshacheema@gmail.com
Abstract: To determine the perception and degree of awareness of patients regarding breast reconstruction and to identify the factors that affected patients’ decisions to undergo breast reconstruction. A cross-sectional hospital-based study was conducted. Sixty female breast cancer patients admitted to the hospital in Pakistan, were included by consecutive sampling. Data was collected through interviews using a predesigned questionnaire and a validated tool -Scale for Motive for and against Breast Reconstruction (SMBR)–and was analyzed using SPSS (v 26.0). Altogether, 60 patients were included, of whom 14 (23.3%) were willing to undergo BR. Those who desired BR were younger (38 vs. 50 years, p=0.001), and highly educated (p = 0.001) compared with patients that were not interested in the procedure. The main reasons to undergo BR were to physically look as before mastectomy (Mdn 6; IQR 5–6) and to have breast symmetry (Mdn 5.5; IQR 5–6) while the main deterrent was fear of complications from the BR procedure (Mdn 6; IQR 5–6.25). Age and educational level were significant predictors of the desire to utilize breast reconstruction. Furthermore, misconception about BR and the lack of knowledge is one of the factors preventing breast cancer patients from undergoing BR. Spreading awareness and providing accurate information regarding the procedure will allow women with BC to learn more about post-mastectomy reconstruction and thus further encourage them to undergo the BR.
Keywords: breast reconstruction, breast cancer, mastectomy
- INTRODUCTION
Breast cancer is one of the most commonly diagnosed cancers in women, with an estimated annual incidence of 2.3 million cases [1]. Pakistan has the highest prevalence of breast cancer in Asia, with one out of every nine women affected. In Pakistan, there were 25,928 breast cancer cases recorded in 2020, accounting for 14.5 percent of total cancer cases. According to the most recent demographic trends, this rate is likely to rise further in the coming years [2]. Treatment strategy for breast cancer is selected on a case-by-case basis. Total mastectomy is one of the major treatments for patients that cannot undergo breast-conserving surgery and for those that choose this modality as a prophylactic measure. Approximately 45% of women diagnosed with early-stage breast cancer undergo mastectomy. However, the loss of a breast after mastectomy can have severe detrimental effects on one’s body image, sexual function, and mental health [3, 4]. To counter the detrimental effects of mastectomy, breast reconstruction may be offered to post-mastectomy patients. According to recent studies, women who undergo breast reconstruction enjoy improved body image, psychological well-being, and sexual relationships as compared to women selecting mastectomy without BR [5, 6]. Breast reconstruction (BR), a surgical procedure of restoring a breast’s form and appearance, can be performed immediately after mastectomy or as a delayed procedure. Different methods are available for breast reconstruction which includes implants, autologous tissue, or a combination of both [7]. Although the number of patients undergoing breast reconstruction has increased over the last decade, it is still quite low, ranging from 5% to 42%. A survey conducted by the American Society of Plastic Surgeons shows that approximately 80% of women are unaware of the availability of a wide range of options for breast reconstructions [8]. In a 10-year audit of breast reconstruction at Agha Khan University, Pakistan, by Samiullah Abdullah et al., 64 breast reconstructions were performed on 60 patients. Out of 60 patients with breast reconstruction, 51 (85%) had immediate reconstruction and 9 (15%) had delayed reconstruction. 31 patients (51.7%) received autogenous reconstructions, while 29 patients (48.33%) had implant-based reconstructions. When compared internationally, the numbers are quite low [9]. Various factors serve as potential barriers to undergoing breast reconstruction, the most common being fear of cancer relapse [10]. Another contributing factor is general surgeons’ failure to explain post-mastectomy breast reconstruction choices [11]. The process of breast reconstruction decision usually has several steps and women prefer having more time and information before the final decision. Thus, women do not always feel well prepared and the decision for breast reconstruction can be a complicated one made under stressful conditions [12]. In Pakistan, there is a lack of sufficient literature in this field. This study is the first of its type to assess the patients’ perception of breast reconstruction and the factors associated with their desire to undergo this procedure. The results of this study should help to increase awareness.
- MATERIALS AND METHODS
We conducted a cross sectional among female breast cancer patients admitted to the hospital in Pakistan for a period of four months (August 2022 to November 2022). The total number of patients required for the study was estimated using 10% absolute precision, 95% confidence level, and an expected percentage of undergoing Breast reconstruction as 16.5% [13]. The estimated required sample size was 53, and a total of 60 individuals participated in this study. A non-probability consecutive sampling method was implemented. The interviewers were trained and guided by the supervisors on the correct way to approach the participants provided the hospital setting of the study. We developed our questionnaire based on a previously published survey. It was tested before distribution through a pilot study, and responses were used for refinement and face validity was assessed by two experts. The questionnaire comprised 42 variables divided into 4 parts. The first part of the questionnaire consisted of questions related to demographic characteristics of the patients. The second part consisted of the questions related to breast cancer, including time since BC diagnosis, forms of treatment received, and family history of BC. The third part was related to the patient’s perception of breast reconstruction. It includes questions regarding prior knowledge of BR, the extent of knowledge about BR, and how they heard about BR. The fourth part consisted of Scale for Motive for and against Breast Reconstruction (SMBR) [14]. The questionnaire was translated in Urdu to facilitate the conversation between participants and researchers. Descriptive statistics were undertaken using frequency and proportions for categorical variables and median (Mdn) and interquartile range (IQR) for quantitative variables to summarize socio-demographic characteristics. Patients willing to undergo BR and those unwilling to undergo BR were compared for all the studied variables. Cross-tabulations were created to compare other studied variables. Chi-square values were presented as P values. If the values in a cell were less than five during any comparison, then the Fisher exact value was presented. The analysis was performed with a 95% confidence interval using SPSS version 26.0. Results were considered significant when the p-value was less than 0.050.
- RESULTS
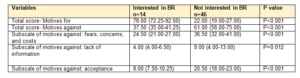
A total of 60 patients were included in this study, with a median age of 49 years (range 27-58). Of them, 30 (50%) had no formal education. The monthly income of 30 (50%) was 15,000 – 49,999 PKR. Overall, 14 (23.3%) patients were interested in undergoing BR. As seen in Table 1, those who desired BR were younger (38 vs. 50 years, p=0.001), and highly educated (p = 0.001) compared with patients that were not interested in the procedure. Also, household income was associated with patients’ willingness to undergo BR (p=0.002). In contrast, relationship status and motherhood were not found to be associated with the desire to undergo BR. The highest percentage of the patients not interested in BR had been diagnosed with BC between the last year and five years later (P=0.002). As seen in Table 2, no significant association was found between knowledge regarding BR and the desire to undergo this procedure. Only 4 (6.67%) out of the total number of patients had their general surgeons explain to them about BR options. The results of the SMBR questionnaire are shown in Table 3 and Table 4. Overall, patients who desired BR stated that their main reasons to undergo this procedure were “to physically look as before mastectomy” (Mdn 6; IQR 5–6) followed by “to improve my self-esteem” (Mdn 5.5; IQR 5–6), “to feel more secure” (Mdn 5.5; IQR 4–6) and “to have breast symmetry” (Mdn 5.5; IQR 5–6). On the other hand, the main reasons stated against undergoing BR in this group were “Worry about the high economical cost” (Mdn 4.5; IQR 3–5), “Fear of complications from the BR procedure” (Mdn 4; IQR 4–4), “Belief that doing daily-life activities would be difficult while recovering from BR”(Mdn 4; IQR 2.5-4) “Fear from pain after undergoing BR” (Mdn 4; IQR 3.5–4) “Fear about cancer returning” (Mdn 4; IQR 2.5–4). In contrast, none of the reasons for undergoing BR achieved a median higher than 2 in the group that did not desire to undergo this procedure. For these patients, the main reasons against undergoing BR were “fear of complications from the BR procedure” (Mdn 6; IQR 5–6.25), “Because I am tired of undergoing surgical procedures” (Mdn 6; IQR 5–7), “Because it is not important to me” (Mdn 6; IQR 5–7), “Not necessary at my age” (Mdn 6; IQR 4.75–7), and “Not knowing the different surgical procedures available for breast reconstruction” (Mdn 5; IQR 2–6).
Table 1: Demographic characteristic according to interest in breast reconstruction (BR)

Table 2: Perception of breast reconstruction
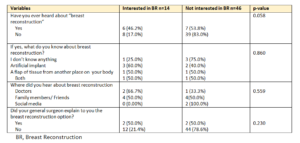
Table 3: Responses for the Scale for Motives for and Against Breast Reconstruction (SMBR)
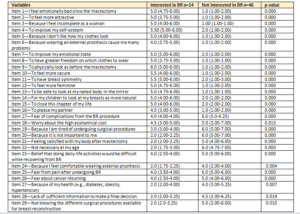
Table 4: Overall scores for the Scale for Motives for and Against Breast Reconstruction (SMBR)
- DISCUSSION
Limited studies are available regarding the proportion and attitude of patients of breast reconstruction in Pakistan. In this study, a large proportion of patients (76.7%) did not desire to undergo BR. This is in line with that of many other populations Nicaragua (77%) 15 and the USA (78%) 16 and more than the UK (50%) [17], Mexico, India, and Saudi Arabia. Women who desired to undergo BR in this study were younger than those who did not want to undergo BR. They also had a higher education status. Regarding their body image they felt less sexually attractive, more deformed, and less feminine since the mastectomy. These are not surprising as other researchers have shown that undergoing BR is associated with a young age. Moreover, specific reasons to undergo BR reported by females were to look physically the same as before mastectomy, to feel more secure, to have breast symmetry, and to be able to look themself naked in the mirror, close their this chapter of life, and for their children. This is similar to other research [17, 18], so we can say that Breast reconstruction is tied to cosmetic reasons but we can see that another factor of motherhood can be seen here. In our cohort, Economical and socioeconomic status was highly associated with the desire for uptake of BR just like that of many other populations [19-21]. In contrast to the USA and UK, where breast reconstruction is an integral part of the treatment of Breast Cancer [22, 23], this service is not covered in Pakistan’s Health system. So, this makes a lot of sense considering that the monthly income of 50% was 15,000 – 49,999. Furthermore, the fact that only 13 (21.67%) of research participants have heard about BR suggests that there may be a major information gap that prevents the acceptance of this procedure. Given that some of the most important reasons against having the operation were “not understanding the different surgical options accessible” and “lack of proper knowledge to make a decisive decision,” this may have a big impact on patients who expressed interest in BR. Since patients indicated that concern about cancer returning was one of the major obstacles to using BR, it was also assumed that BR might have a negative impact on their prognosis. Like earlier articles, we believe that by providing patients with enough knowledge regarding BR, such a false belief may be easily disproved. It is noteworthy that alerting patients undergoing mastectomy surgeries about the possibility of BR is not required under the current national consensus recommendations for the diagnosis and management of breast cancer [24, 25]. Only 4 (6.67%) of the participants in this study could recall talking to a doctor about the procedure, which underscores the need for institutional actions to address the population’s poor access to information. To increase the use of this method and lessen care disparities, it is important to inform all breast cancer patients undergoing total mastectomy therapy about the possibility of having BR. Sharing information should be followed by a discussion about the procedure’s practicality, the numerous procedures available taking into account specific clinical aspects, as well as the predicted risks and benefits in order to strengthen the collaborative decision-making process. Such a conversation should be held regardless of the patient’s financial situation, age, marital status, or kind of healthcare coverage. We have not yet fully analyzed the reasons behind doctors’ propensity to under-inform patients about this procedure in Pakistan public healthcare facilities, but it may be due to some of the cultural and religious beliefs of Pakistani doctors and also because most of the mastectomy surgeries are done in public Hospitals of Pakistan where surgeries and health care is free of cost so the most appropriate health care is not being provided. This idea is supported by the findings of Alderman et al., who found a link between a physician’s perception of access barriers and the low referral rate for this procedure. In contrast to what was seen in our study, higher rates of BR conversations with doctors have been reported in other populations. Since it has been shown in the past that giving patients with enough information is associated with improved BR uptake, addressing the information gap in this demographic may be crucial to enhancing national BR adoption and improving therapy for this population. There are various limitations to this study. First off, the data might have been skewed in some way as it was self-reported by the participants. The survey that our study team constructed specifically addressed interest in and information distribution about BR, and there is no data on its effectiveness, even though previously validated questionnaires were used as much as possible. Thirdly, given the small sample size, the findings only accurately represent the experiences of one tertiary care hospital. As a result, it’s probable that the findings cannot be extrapolated to other countries.
- CONCLUSION
Age and educational level were significant predictors of the desire to utilize breast reconstruction. Furthermore, the lack of knowledge and misconception about BR is one of the factors preventing breast cancer patients from undergoing BR. Spreading awareness and providing accurate information regarding the procedure will allow women with BC to learn more about post mastectomy reconstruction and thus further encourage them to undergo the BR.
REFERENCES
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin [Internet]. 2021 May 1 [cited 2022 Jun 8];71(3):209–49.
- Zaheer S, Shah N, Maqbool SA, Soomro NM. Estimates of past and future time trends in age-specific breast cancer incidence among women in Karachi, Pakistan: 2004-2025. BMC Public Health [Internet]. 2019 Jul 25 [cited 2022 Jun 8];19(1):1–9.
- Bajonero-Canonico P, Ferrigno AS, Saldaña-Rodriguez JA, Hinojosa-Gonzalez DE, de la O-Maldonado CG, de la Cruz-de la Cruz C, et al. Factors associated with the desire to undergo post-mastectomy breast reconstruction in a Mexican breast cancer center. Support Care Cancer [Internet]. 2021 May 1 [cited 2022 Apr 21];29(5):2679–88.
- Alinejad Mofrad S, Fernandez R, Lord H, Alananzeh I. The impact of mastectomy on Iranian women sexuality and body image: a systematic review of qualitative studies. Support Care Cancer [Internet]. 2021 Oct 1 [cited 2022 Apr 22];29(10):5571–80.
- Howes BHL, Watson DI, Xu C, Fosh B, Canepa M, Dean NR. Quality of life following total mastectomy with and without reconstruction versus breast-conserving surgery for breast cancer : A case-controlled cohort study *. Br J Plast Surg [Internet]. 2016;61:1–8.
- Hart AM, Pinell-White X, Losken A. The Psychosexual Impact of Postmastectomy Breast Reconstruction. Ann Plast Surg [Internet]. 2016 Nov 1 [cited 2022 Apr 22];77(5):517–22.
- Toyserkani NM, Jørgensen MG, Tabatabaeifar S, Damsgaard T, Sørensen JA. Autologous versus implant-based breast reconstruction: A systematic review and meta-analysis of Breast-Q patient-reported outcomes. J Plast Reconstr Aesthet Surg [Internet]. 2020 Feb 1 [cited 2022 Apr 22];73(2):278–85.
- Aljaaly HA, Mortada H, Trabulsi NH. Patient Perceptions and Determinants of Choice for Breast Reconstruction after Mastectomy among Saudi Patients. Plast Reconstr Surg Glob Open [Internet]. 2021 [cited 2022 Jun 8];9(9).
- Abdullah S, Ahsan A, Khan TS. Breast reconstruction at The Aga Khan University – A 10 year audit. J Pak Med Assoc. 2016;66 3)(10).
- Nozawa K, Ichimura M, Oshima A, Tokunaga E, Masuda N, Kitano A, et al. The present state and perception of young women with breast cancer towards breast reconstructive surgery. Int J Clin Oncol [Internet]. 2015 Apr 1 [cited 2022 Jun 8];20(2):324–31.
- Barnsley GP, Sigurdson L, Kirkland S. Barriers to breast reconstruction after mastectomy in Nova Scotia. Can J Surg [Internet]. 2008 [cited 2022 Jun 8];51(6):447.
- Manne SL, Topham N, Kirstein L, Virtue SM, Brill K, Devine KA, et al. Attitudes and Decisional Conflict regarding Breast Reconstruction Among Breast Cancer Patients. Cancer Nurs [Internet]. 2016 Nov 1 [cited 2022 Apr 21];36(6):427.
- Awan BA, Samargandi OA, Alghamdi HA, Sayegh AA, Hakeem YJ, Merdad L, et al. The desire to utilize postmastectomy breast reconstruction in Saudi Arabian women. Predictors and barriers. Saudi Med J [Internet]. 2015 Mar 1 [cited 2022 Nov 9];36(3):304–9.
- Miaja Ávila M, Moral de la Rubia J, Villarreal-Garza C. Qualitative phase of the development of a scale of motives for and against breast reconstruction (SMBR). Psicooncologia. 2018;15(2):327–44.
- Nimra Naseem, Rubab Zahra, Umm-e-Aimen & Tahir Rana. Literature Review on Comparison of the effect of Single Oral Dose 150 Mg Pregabalin Premedication to Single Oral Dose 100mg Tramadol in Elective Inguinal Hernia Surgery. Dinkum Journal of Medical Innovations, 2(01):01-11.
- Tahira Amanat, Umm-e-Aiman, Tayyaba Firdus & Zahida Bukhari. A Systematic Literature Review on Suicidal Cases in Pakistan. Dinkum Journal of Medical Innovations, 2(01):12-17.
- Tahira Amanat, Tayyaba Firdus & Zahida Bukhari. A Systematic literature review on Relationship of Inadequate Birth Weight and Adolescent Diabetes Mellitus. Dinkum Journal of Medical Innovations, 2(01):18-21.
- Marie Diack, Derak Stewart, Parshu Kirby & David Moris. Challenges with Parent/Caregiver Medication Administration in Peadiatrics and the Importance of Patient Education: A Systematic Review. Dinkum Journal of Medical Innovations, 2(01):22-28.
- Marie Diack, Derak Stewart & Parshu Kirby. Predisposing Factors and Effects of Re-Procedure after Cardiac Resection. Dinkum Journal of Medical Innovations, 2(01):29-34.
- Brennan ME, Spillane AJ (2013) Uptake and predictors of postmastectomy reconstruction in women with breast malignancysystematic review. Eur J Surg Oncol 39:527–541.
- Wilkins EG, Alderman AK (2004) Breast reconstruction practices in North America: current trends and future priorities. Semin Plast Surg 18:149–155.
- Offodile AC, Guo L (2016) Disparate British breast reconstruction utilization: is universal coverage sufficient to ensure expanded care? Plast Reconstr Surg – Glob Open 4:e738.
- Héquet D, Zarca K, Dolbeault S, Couturaud B, Ngô C, Fourchotte V, de la Rochefordière A, Féron JG, Fitoussi A, Bélichard C, Reyal F, Laki F, Hajage D, Sigal B, Asselain B, Alran S, Institut Curie Breast Cancer Group, Roman Rouzier (2013) Reasons of not having breast reconstruction: a historical cohort of 1937 breast cancer patients undergoing mastectomy. Springerplus 2:325.
- Lardi AM, Myrick ME, Haug M, Schaefer DJ, Bitzer J, Simmen U, Güth U (2013) The option of delayed reconstructive surgery following mastectomy for invasive breast cancer: why do so few patients embrace this offer? Eur J Surg Oncol 39:36–43.
Publication History
Submitted: January 04, 2023
Accepted: January 20, 2023
Published: February 01, 2023
Identification
D-0100
Citation
Muhammad Ayan & Ayesha Pervaiz Cheema (2023). Patients’ Perceptions of Post-Mastectomy Mammary Reconstruction: Contributing Variables. Dinkum Journal of Medical Innovations, 2(02):42-49.
Copyright
© 2023 DJMI. All rights reserved