

")
Publication History
Submitted: March 04, 2023
Accepted: March 20, 2023
Published: April 01, 2023
Identification
D-0113
Citation
Imran Mehfooz Khan, Aron Kumar & Pradeep Sahejpal (2023). Extensive Management Medical Incidents Provided to Gallbladder Cancer Using Cholecystectomy Specimen. Dinkum Journal of Medical Innovations, 2(04):150-156.
Copyright
© 2023 DJMI. All rights reserved
150-156
Extensive Management Medical Incidents Provided to Gallbladder Cancer Using Cholecystectomy SpecimenReview Article
Imran Mehfooz Khan 1*, Aron Kumar 2, Pradeep Sahejpal 3
- King Edward Medical University, Lahore: mehfoozimrankhan02@gmail.com
- Nepal Medical College and Teaching Hospital (NMC), Nepal: aronkumar@gmail.com
- Nepal Medical College and Teaching Hospital (NMC), Nepal: pradeepking10@gmail.com
* Correspondence: mehfoozimrankhan02@gmail.com
Abstract: A cholecystectomy involves the surgical removal of the gallbladder. In order to ascertain the prevalence of GBC, cholecystectomy specimens are examined. A very uncommon illness, GBC affects more women than men. Finding out how common gallbladder cancer is in hospitals during a five-year period is the aim of this study. On the basis of earlier data, the current investigation was carried out retrospectively. Information obtained at hospital patient registration served as the primary component of the data. Data on a variety of variables, including age, sex, and procedure type, were collected retroactively from the hospital record and utilized for statistical analysis. All patients who were missing relevant data, like demographics or a proper diagnosis confirmation, were removed. Only 7 cases (0.4%) out of 1835 cholecystectomy specimens have adenocarcinoma. Females (6 cases, 85.71%) are more likely than males (1 case, 14.78%) to get gallbladder cancer. Acute cholecystitis (66, or 3.6%), xanthogranulomatous cholecystitis (30, or 1.6%), gangrenous cholecystitis (6, or 0.34%), follicular cholecystitis (3, or 0.016%), and one case (0.05%) each of cholesterolosis, foci of chronic inflammation, hemorrhagic infarction, and empyema gallbladder comprised the majority of cases (1703, or 92.8%). Thirteen patients (0.79%) had partial or complete autolysis. The most frequent condition found in cholecystectomy specimens is chronic cholecystitis, which is followed by xanthogranulomatous cholecystitis, gangrenous cholecystitis, follicular cholecystitis, acute cholecystitis, and empyema gallbladder. Although extremely uncommon, gallbladder cancer is more common in women than in men.
Keywords: cholecystitis, gall blader, management, medical cases, cholecystectomy specimen
- INTRODUCTION
Diseases of the gallbladder constitute a global health concern [1]. The gallbladder (GB) can be harmed by infectious, hereditary, and neoplastic illnesses [2, 3]. These diseases cause signs and symptoms that call for open or laparoscopic cholecystectomy surgery. Compared to other GB diseases, proinflammatory GB problems are more prevalent and can present as various forms of cholecystitis. References [4,5]. With a 5-year survival rate of approximately 5%, gallbladder carcinomas are aggressive in nature [6]. Gallbladder cancer is thought to advance progressively from metaplasia through dysplasia to carcinoma because it is thought to occur in the setting of prolonged, chronic inflammation [7]. For a number of reasons, cholecystectomy is a prevalent treatment; as laparoscopy advances, the procedure’s frequency increases. Consequently, the likelihood of gallbladder cancer being unintentionally discovered increases. Gallbladder carcinoma is a prevalent malignancy that is ranked seventh among all digestive tract tumors [8]. A tumor discovered by accident following a cholecystectomy or following a histological analysis of a gallbladder sample removed for a benign gallbladder condition is known as incidental gall bladder cancer (IGBC). The pathology department in Patna reports an incidence of 0.19 to 3.3 percent of IGBC cases [9]. The delivery of a histologic study of gallbladder specimens in tertiary hospital settings in Pakistan is behind schedule due to a shortage of personnel and an excessive workload [10, 11]. According to generally recognized guidelines, the majority of gallbladder specimens should be carefully inspected in order to rule out cancer [12]. Intestinal metaplasia accounted for 0.2 percent and reactive atypical for 0.5 percent of cases in Western individuals. Most people who suffer from these premalignant conditions are in their later years. This implies that the likelihood of a malignant alteration rises with age [13, 14]. Although there is a substantial global correlation between gall bladder cancer and CC, the exact etiology is uncertain. Those with untreated cholelithiasis had an estimated 0.2–0.5 percent likelihood of developing cancer during a 20-year period [15]. Numerous risk factors, such as heredity, dietary variations, endo and exotics, chronic inflammation, and infection, have been associated with gall bladder cancer [16]. According to Barcia JJ et al., gallbladder cancer (GBC) is primarily a moderately to poorly differentiated adenocarcinoma [8]. Chronic inflammation is closely associated with the malignant modification of cells. Prolonged inflammation breaks down DNA, which leads to repeated tissue growth and repair. This response predisposes cells to neoplastic transformation by releasing cytokines and growth factors [17]. Early detection of unintentional gall bladder cancer improves the prognosis. Because gall bladder cancer often manifests late, its prognosis is dismal [9]. The most significant prognostic factors for gall bladder cancer are its clinical and pathological phases. The tumor’s size, location inside the gall bladder, presence or absence of dysplastic mucosa, and grade are additional crucial factors that affect surgical options and forecast success [15]. Despite being better than a preoperative suspected carcinoma, the prognosis for an incidental carcinoma (IC) is still not good: The literature reports 5-year survival rates of 35 percent against 5 percent, with a median survival time in suspected cases of 26.5 versus 9.2 months [18]. Khoo JJ et al. in Johor, Malaysia found 9 (0.8%) cases of gallbladder cancer in a study of 1122 cholecystectomy specimens, including 77.77 percent of incidental carcinoma and 22.22 percent of clinically suspected carcinoma. Each of the seven patients with incidental cancer had one occurrence of clinically probable gallbladder carcinoma; three of the patients were males and four were females [19]. This study highlights the prevalence and presentation patterns of all patients with gallbladder cancer (GBC) that were evaluated over a five-year period at our tertiary hospital. Our study, which takes a retrospective approach, intends to ascertain the frequency and prevalence of GBC during a five-year period in tertiary care facilities.
- LITERATURE REVIEW
Gallbladder issues are prevalent, but gallbladder cancer is rare. The most reliable method for estimating the frequency of gallbladder problems is ultrasonography. The formation of cholesterol gallstones is influenced by a number of permanent variables, such as inheritance, family history, age, and gender. Conversely, obesity, rapid weight reduction, and inadequate physical exercise are among the modifiable risk factors for cholesterol gallstones [1]. All GBC instances in Malaysia were identified using clinical and radiological approaches, regardless of whether the events occurred before to or during surgery [6]. Regular histological testing is essential to ensure early cancer detection and a better prognosis since long-term stones are more prone to develop premalignant and malignant diseases [2]. The gallbladder mucosa undergoes a transition from cholecystitis, hyperplasia, and metaplasia to malignancy as the gallstone grows in size. Different types and volumes of gallstones might result in precancerous lesions [3]. The upper gastrointestinal tract condition cholelithiasis and microbial infections are two examples of environmental factors that might cause gallbladder cancer. There is a close correlation between the incidence and death rate of gallbladder cancer; the majority of deaths happen in nations where gallstones are prevalent. Sometimes gallbladder cancer is discovered too late because of its modest signs. Surgical removal is the only way to get rid of it. By coincidence, some patients having a cholecystectomy for cholelithiasis also end up having gallbladder cancer [14]. Cholelithiasis is the most frequent comorbidity associated with gallbladder cancer. Multiple family “porcelain” gallbladder, Peutz-Jeghers syndrome, polyposis/Gardner syndrome, and abnormal pancreato-biliary ductal union have all been linked to gallbladder cancer [16]. After cholecystectomy, histological results can vary greatly. Although gall bladder CC and AC/empyema were the most common disorders, gall bladder cancer was an uncommon incidence [12]. Improved ultrasonic methods and more targeted diagnostic markers could improve results. Secondary prophylaxis should be taken into consideration once the benefits of delaying gallbladder removal in high-risk patients and Aboriginal regions have been demonstrated. Once developing mutations and external environmental factors have been identified, primary prevention will be implemented. Those who have gallbladder cancer now have a better chance of surviving because of recent advancements. Identifying the main risk factors, implementing suitable early staging, and performing a thorough surgical excision are all necessary for better results [14]. The global incidence and distribution of gallbladder cancer, along with a summary of its primary causes and some suggestions for prevention, are detailed here. North Indians, Mexicans, and Andeans have greater rates of gallbladder cancer. Across all demographic groupings, women are up to three times more likely than males to get gallbladder cancer. There are comparatively low incidence rates in other parts of the world. The continent of South America has the highest GBC death rate. According to reports from Brazil, Colombia, Ecuador, Peru, and Ecuador, intermediate values between 3.7 and 9.1 per 100,000 have been observed [16]. Gallbladder carcinoma is one cancer that has a significant fatality rate. Unfortunately, specimens from the gallbladder are usually discarded if a malignancy is discovered following a cholecystectomy. As a result, premalignant illnesses such as carcinomas in their early stages are overlooked [20]. The term incidental gall bladder carcinoma (IGBC) refers to the unintended finding of cancer during a laparoscopic cholecystectomy or when a gall bladder specimen extracted for benign gall bladder disorders is examined histologically. At presentation, the mean age of the women with IGBC was 50 years old, and the majority of them were in their fifth decade of life. Gallstones were present in 85% of IGBC patients. Cholelithiasis is a well-known, substantial risk factor for gall bladder cancer [9]. PSC, a carcinogenic “field effect” of systemic inflammation, supports the participation of CGI and subsequent oncogenesis by increasing the risk of GB malignancies that result from a metaplasia-dysplasia-carcinoma sequence [21]. Gallbladder polypoidal tumors, which affect 5% of individuals, are sometimes misinterpreted as gallbladder cancer. Inflammatory polyps, leiomyomas, and adenomas make for two thirds of polyps. While gallbladder polyps are sometimes linked to biliary colic, most of them are incidentally discovered during abdominal imaging tests and do not cause any symptoms. The presence of concomitant gallstones, large polyps (>11 millimeters), a single or septate mass, a patient older than fifty, and—most importantly—rapid growth of the polyps are all indicators of malignancy [24].
- MATERIALS AND METHODS
Over the course of six months, we carried out a retrospective investigation in the pathology department at King Edward Medical University in Lahore. With a 95% confidence level, 2% absolute precision, and an estimated percentage of gallbladder carcinoma of 74.28 percent, the sample size of 1835 patients was determined. Information obtained at hospital patient registration served as the main source of the data. Data on a variety of variables, including age, sex, and procedure type, were collected retroactively from the hospital record and utilized for statistical analysis. All patients who were missing relevant data, like demographics or a proper diagnosis confirmation, were removed. SPSS-26 was utilized for data entry. Mean and standard deviation will be provided for age and other quantitative parameters. Using the Fisher exact test, dichotomous univariate analysis was conducted. Differences were deemed statistically significant if P was less than 0.05.
- RESULTS AND DISCUSSION
1835 cholecystectomy specimens were examined over six months. The patients’ ages ranged from 13 to 19. The average age at the time of presentation was 41.07. Females were impacted more frequently (1501 cases, or 81.8 %), while males were only affected in 334 cases (18.2%). Adenocarcinoma is found in only 7 cases (0.4%) out of 1835 cholecystectomy specimens. Gallbladder cancer is more common in females (6, 85.71%) than in males (1 case, 14.78%). Chronic cholecystitis accounted for the majority of the cases (1703, or 92.8%), followed by acute cholecystitis (66, or 3.6%), xanthogranulomatous, cholecystitis (30, or 1.6%), gangrenous cholecystitis (6, or 0.34%), follicular cholecystitis (3, or 0.016%) and one case (0.05%) each of cholesterolosis, foci of chronic inflammation, hemorrhagic infarction and empyema gallbladder. 13 cases (0.79%) were partially or fully autolyzed. In our study, we examined 1835 cholecystectomy specimens from the previous five years in the department of pathology (Histopathology) at Mayo Hospital in Lahore to see the prevalence of gallbladder cancer. The results of our study showed that the mean age of patients was 41.07±12.577. The prevalence of gallbladder cancer in all cholecystectomy specimens is 0.4% as in tertiary hospital Pernambuco, Brazil [25]. A total of 1,370 gallbladder GC samples were sent for histological investigation, with seven (0.41%) being discovered to be malignant and just three cases (0.15%) having primary GBC in tertiary care hospital of Malaysia same as in our research [6]. Gallbladder cancer is predominantly present in females (85.71%) than in males as in many international studies (14.78%) [6]. We have also seen that chronic cholecystitis present in the majority of the cases (92.8%), followed by acute cholecystitis (3.6%), xanthogranulomatous cholecystitis (1.6%), gangrenous cholecystitis (0.34%), follicular cholecystitis (0.016%), and one case (0.05%) each of cholesterolosis, foci of chronic inflammation, hemorrhagic infarction and empyema gallbladder [2]. A total of two hundred eighty-two gall bladder specimens were examined at IUH in Hyderabad. Seventy-five of them were males, while the remaining two hundred and seven were females. CC was the most common histopathological finding in 64. In our study, we did not take gallstones’ relation with the prevalence of gallbladder carcinoma under consideration because it would complex our specific study.
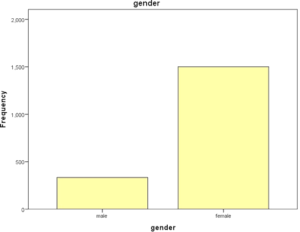
Figure 1: Gender of participants
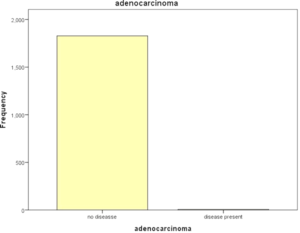
Figure 2: Adenocarcinoma cases
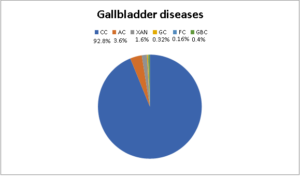
Figure 3: Gall bladder diseases
- CONCLUSION
The most frequent condition found in cholecystectomy specimens is chronic cholecystitis, which is followed by xanthogranulomatous cholecystitis, gangrenous cholecystitis, follicular cholecystitis, acute cholecystitis, and empyema gallbladder. Although extremely uncommon, gallbladder cancer is more prevalent in women than in men.
REFERENCES
- Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver 2012; 6: 172-87
- Gupta K, Faiz A, Thakral RK, Mohan A, Sharma VK: The spectrum of histopathological lesions in the gallbladder in cholecystectomy specimens. Int J Clin Diagnostic Pathol. 2019, 2:146-151. 10.33545/pathol.2019.v2.i1c.22
- Singh A, Singh G, Kaur K, Goyal G, Saini G, Sharma D: Histopathological changes in gallbladder mucosa associated with cholelithiasis: a prospective study. Niger J Surg. 2019, 25:21-25. 10.4103/njs.NJS_15_18.
- Gupta OP, Khan S: Incidents and complications in laparoscopic cholecystectomy: a retrospective analysis of 336 cases. Int J Contemporary Med Surg Radiol. 2019, 4:1-5 10.21276/ijcmsr.2019.4.2.1
- Thukral S, Roychoudhury AK, Bansal N, Rani E: Histopathological spectrum of gall bladder lesions in a tertiary care hospital in the Malwa belt: a +hospital-based study. Ann Pathol Lab Med. 2018, 5:878-881. 10.21276/apalm.2192
- Chin KF, Mohammad AA, Khoo YY. Impact of routine histopathological examination on cholecystectomy specimens from an Asian demographic. Ann R Coll Surg Engl 2012; 94: 165-9.
- Segovia Lohse HA, Cuenca Torres OM. Prevalence and sequence of metaplasia- dysplasia- carcinoma of the gallbladder. A single-center retrospective study. Cir Esp 2013; 91(10): 672-5.
- J. Barcia, A. Rodrıǵ uez, L. Siri, A. Masllorens, P. Szwebel, G. Acosta Gallbladder carcinoma in the “Hospital de Clinicas” of Uruguay: 1998–2002. A clinicopathologic study of five cases in 802 cholecystectomies Ann. Diagn. Pathol., 8 (1) (2004), pp. 1-5
- Waghmare RS, Kamat RN. J Assoc Physicians India. 2014 Sep;62(9):7936.
- Sarah Rehman, Saira Rana & Mehru-Nisa. Knowledge, Influence of Factors, and Management Strategies among Family Members with Behavioral Conditions. Dinkum Journal of Medical Innovations, 2(03):79-84.
- John Petter. Anti-Depressant Consumption, Patterns, Prevalence, and Risk Considerations among Women in the Fertile Age Range. Dinkum Journal of Medical Innovations, 2(03):85-90.
- Rabia Saeed. Academic Honesty in Undergraduate Students in Pakistan. Dinkum Journal of Medical Innovations, 2(03):91-96.
- Ayesha Nasir. Common Bacteria Involved in Fascial Space Infection and Antibiotics Sensitivity. Dinkum Journal of Medical Innovations, 2(03):97-110.
- Maira Younas & Mehreen Younas. Rehabilitation of Venous Ulcers in Individuals Undergoing the Trendelenburg Technique as Opposed to Trendelenburg with Stab Avulsion. Dinkum Journal of Medical Innovations, 2(03):111-119.
- Lazcano-Ponce E C, Miquel J f, Muinoz N, Herrero, Ferreeio C, Wistuba, I I, Alonso de Ruiz P, et al. Epidemiology and molecular pathology of gall bladder cancer. C A Cancer J Clin, 2001; 51: 349.
- Goetze TO. Gallbladder carcinoma: Prognostic factors and therapeutic options. World J Gastroenterol, 2015; 21(43): 12211-12217.
- Borreca D, Balcet F, Bona A, Bossotti M, Paolis PD. Radical Surgery for Incidental Gallbladder Carcinoma. Which Subset of Patients is Really Suitable for? J Gastrointest Dig Syst, 2015; 5: 1-4.
- J. Khoo, N.A. Misron A clinicopathological study of nine cases of gallbladder carcinoma in 1122 cholecystectomies in Johor, Malaysia Malays. J. Pathol., 30 (1) (2008)
- J. Islam, S. Akter, A.R. Talukder, M.S. Haque Role of routine histopathology of gallbladder specimen from gallstone disease to detect unsuspected carcinoma J. Bangladesh Coll. Phys. Surg., 37 (4) (2019), pp. 186-190
- Chapman R, Fevery J, Kalloo A, Nagorney DM, Boberg KM, Shneider B, Gores GJ. Diagnosis and management of primary sclerosing cholangitis. Hepatology. 2010;51:660–678.
- Goetze TO, Paolucci V. Benefits of reoperation of T2 and more advanced incidental gallbladder carcinoma: analysis of the German registry. Ann Surg. 2008;247:104–108.
- Goetze TO, Paolucci V. [Incidental T1b-T3 gallbladder carcinoma. Extended cholecystectomy as an underestimated prognostic factor-results of the German registry] Chirurg. 2014;85:131–138.
- Myers RP, Shaffer EA, Beck PL. Gallbladder polyps: epidemiology, natural history and management. Can J Gastroenterol. 2002;16:187–194.
- Martins-Filho ED, Batista TP, Kreimer F, MARTINS AC, Iwanaga TC, LEÃO CD. Prevalence of incidental gallbladder cancer in a tertiary-care hospital from Pernambuco, Brazil. Arquivos de gastroenterologia. 2015 Jul;52:247-9.
Publication History
Submitted: March 04, 2023
Accepted: March 20, 2023
Published: April 01, 2023
Identification
D-0113
Citation
Imran Mehfooz Khan, Aron Kumar & Pradeep Sahejpal (2023). Extensive Management Medical Incidents Provided to Gallbladder Cancer Using Cholecystectomy Specimen. Dinkum Journal of Medical Innovations, 2(04):150-156.
Copyright
© 2023 DJMI. All rights reserved