

")
Publication History
Submitted: May 05, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0119
Citation
Nabeela Riaz, Rabia Zulfiqar, Muhammad Naveed Akhter & Msooma Sheikh (2023). Dentinogenesis Imperfecta type II Underwent Whole Mouth Rehabilitation Employing Various Treatment Modalities. Dinkum Journal of Medical Innovations, 2(06):201-206.
Copyright
© 2023 DJMI. All rights reserved
201-206
Dentinogenetic Imperfecta type II Underwent Whole Mouth Rehabilitation Employing Various Treatment ModalitiesCase Study
Nabeela Riaz 1, Rabia Zulfiqar 2*, Muhammad Naveed Akhter 3, Msooma Sheikh 4
- Oral & Maxillofacial Surgery Department, King Edward Medical University, Lahore, Pakistan; nabeelariaz@yahoo.com
- King Edward Medical University, Lahore, Pakistan; rabiazulfiqar77@gmail.com
- Nishtar Medical University, Pakistan; hpereformer@gmail.com
- School of Allied Health Sciences, Children Hospital, Lahore, Pakistan; masoomasheikh375@gmail.com
* Correspondence: rabiazulfiqar77@gmail.com
Abstract: Decontinogenesis imperfecta (DGI) is a complex anomaly in terms of both its course of treatment and its structure. The intensity, the patient’s behavior, and their age all influence the therapy plan. Case Summary: This study reports on the DGI type II (DGI-II) instances of two siblings, each of whom had a different course of treatment depending on their age, behavior, and clinical severity (mixed versus primary dentition). In the initial instance, a patient in the primary dentition experienced significant attrition, which resulted in a decrease in the vertical dimension of occlusion (VDO). The patient was treated by having full overlay dentures made. A patient in the second case has extractions and restorations performed on their early mixed dentition. In both cases, full mouth rehabilitation significantly enhances function and appearance and has been shown to significantly improve the patients’ psychological well-being. A good prognosis for people with DGI requires an early diagnosis, a multidisciplinary approach to preserve the remaining teeth, and rehabilitation for both function and appearance.
Keywords: dental anomaly, decontinogenesis imperfect, mouth rehabilitation, dentinogenesis imperfect
- INTRODUCTION
A hereditary condition affecting the development of teeth, dentinogenesis imperfecta (DGI) affects both the primary and permanent dentition. Patients with DGI have teeth that are yellow-brown or blue-gray in colour and are prone to loss, breakage, and wear [1]. Given that DGI is an autosomal dominant hereditary ailment, a child’s odds of contracting the illness are 50% if one of their parents has the genetic disorder. One in every 6000 to 8000 infants has DGI, one of the most prevalent dentin genetic diseases in humans [2, 3]. DGI was divided into three types by Shields et al. [4]: DGI type I (DGI-I), which is linked to osteogenesis imperfecta (OI) as a result of mutations in the collagen gene; DGI type II (DGI-II), which shares clinical, radiographic, and histological characteristics with OI but does not have OI; and DGI type III (DGI-III), which is uncommon and unique to the triracial Brandywine population in Maryland [4]. The dentin sialophospho protein (DSPP) gene, which is found on chromosome 4q21.3 and exhibits significant expression in odontoblasts, is known to be linked to DGI-II and DGI-III [5]. Diagnostic categories include hypocalcified varieties of amelogenesis imperfecta, dentin dysplasia, congenital erythropoietic porphyria, conditions that cause early tooth loss (e.g., cyclic neutropenia, Chediak–Hegashi syndrome, histiocytosis X, Papillon–Lefevre syndrome), rickets that is vitamin D-dependent and vitamin D-resistant, and disorders resulting in permanent tooth discoloration as a result of tetracycline use [1]. Phosphorphoryn (PP) and dentin sialoprotein (DSP) are the products of the proteolytic cleavage of DSPP. While Qui et al. showed that proteolytic cleavage of DSPP is an essential activating step in the production of dentin [7], Zhang et al.’s study suggested that the interaction between DSP and PP proteins may be required for dentinogenesis [6], which is disturbed in DGI. Moreover, dentin pulp cells in DGI patients lacking DSPP cleavage develop into chondrocyte-like cells, which impairs tissue regeneration and pulpal wound healing (e.g., secondary and tertiary dentin) [8]. The morphological feature known as scalloping connects the dentino-enamel junction and results in the mechanical interlocking of the enamel and dentinal tissues [9, 10]. DGI patients have altered dentin structure; as a result, the damaged dentin lacks scalloping, which causes enamel to shatter and rapidly forms the defective dentin [11]. Through the use of two distinct treatment modalities—one for the primary dentition and the other for the early mixed dentition—these case studies seek to illustrate the goals, methods, and issues found during the management of DGI-II kids from a single household.
- CASE ONE AND CASE TWO
The Paediatric Dental Clinic in Lahore received a 5-year-old child and her mother as patients. The young patient had previously visited the clinic several times for urgent care of dental abscesses. “My daughter is going to school next year, and I am worried about her being harassed due to the colour of her teeth and the way her face looks,” was the mother’s main grievance this time. Following a full-term pregnancy, the child was delivered, and her developmental milestones were all met. There was no historical medical history of drug use, exceptional brittleness of the bones, or any other systemic ailment. The patient had moderate dental hygiene and consumed sweet foods and beverages seldom. According to family history, the mother had an implanted overdenture and was diagnosed with DGI-II. Furthermore, DGI-II would subsequently be diagnosed in two of her siblings. The intraoral exam showed severe attrition/wear of the primary dentition to the level of gingiva with color deviation from normal to yellow–brown with a translucent appearance, as seen in Figure 1.

Figure 1: The 5-year-old girl from the DGI-II family’s proband exhibits clinical oral manifestation of DGI-II. Significant deterioration of the main tooth structure to the gingiva level was seen in the intraoral photos, with a colour variation from normal to yellow-brown and a translucent look. (A) closed-mouth intraoral picture of the anterior aspect. (B) Images taken intraorally of the maxillary arch. (C) Anterior aspect intraoral shot with mouth open. (E) An intraoral picture of the mandibular arch; (D) an intraoral photo of the right side. (F) Left side intraoral picture.
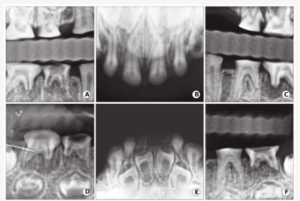
Figure 2: Case 1: The proband of the 5-year-old girl belonging to the DGI-II family has radiographic oral manifestation of DGI-II. Bitewings radiographs (A, C) revealed thin dentine with significant occlusal deterioration. (B, E) The growing lower anterior permanent teeth had enlarged pulp chambers, thin enamel, and incisal attrition with pulp narrowing as seen by upper and lower occlusal radiographs. (D,F) Periapical radiographs of the lower left and right molars showed abscessed second right and left molars with occlusal deterioration.
Radiographic examinations revealed a primary dentition present with severe loss of the enamel associated with severe occlusal attrition. Primary upper and lower left second molars, and primary right first and second molars had pulpal involvement with a periapical radiolucency. The presence of developing permanent buds was also evident with thin enamel, large pulp chambers, and mild cervical constriction of the crowns. The child’s dental age, determined radiographically, was consistent with her chronological age (Figure 2). A 7-year-old male presented to the same clinic with his mother and younger sibling noted in case one. The patient had a severe autism spectrum disorder (ASD), DGI-II, and sickle cell trait (SCT). The child was non-verbal and unable to report tooth pain. The patient mixed dentition, with a past history of primary teeth extracted under oral conscious sedation (OCS). The patient had poor oral hygiene with large amounts of plaque and calculus builds up on anterior teeth. In CASE 2, due to prior ineffective OCS and severe ASD, treatment under General Anesthesia (GA) was accepted as the best method to restore the patient’s oral health. Under GA, a full set of radiographs were taken (Figure 3), along with intraoral photographs (Figure 4), which revealed an irregular/extensive caries pattern extending to the cusp on all permanent first molars due to attrition and poor enamel to dentin strength associated with DGI-II. The patient had amber-hue colored anterior teeth with most enamel missing and attrition down to the gingival margin on all primary first and second molars, and caries were present on the facial surface of all upper and lower anterior incisors as seen in Figure 4.
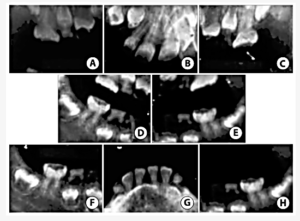
Figure 3 Case 2: Non-digital radiographs obtained while the patient was in the hospital under general anaesthesia (GA) show that both primary and permanent teeth have significant enamel loss and limited pulp space (A–C). (D,E) Fragments of the upper primary canines’ root tips are observed. On the lower permanent first molars, extensive atypical occlusal caries was observed (F,H). (G) Lower primary canines almost exfoliating, with less pulp space in permanent mandibular incisors.
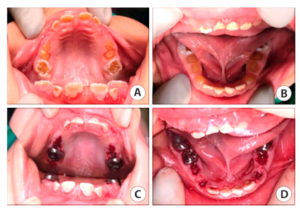
Figure 4: Clinic images for Case 2; the maxillary arch’s intraoral pre-operative picture (A). (B) Mandibular arch intraoral shot taken prior to surgery; part of the mandibular first molars is visible. (C) Post-operative intraoral photo of the maxillary arch shows permanent first molars restored with stainless steel crowns (SSC), facial resin-modified glass ionomer (RMGI) restorations, lingual sealants on permanent incisors, and clots of blood at the extraction sites of all primary teeth that are still present. (D) A post-operative intraoral photo of the mandibular arch shows that primary first molars and canines have been extracted, and SSCs have been placed on second primary molars and permanent first molars (the bottom left permanent first molar is not visible). RMGI positioned on the anterior incisor facial surfaces.
- DISCUSSION
Aside from behavioural control, one of the biggest obstacles in treating children’s DGI disease is providing enough treatment to produce both functional and aesthetically pleasing restoration. Practitioners can safely provide young children with exceptional health care requirements with high-quality restorative treatment if they implement advanced behaviour management in a reasonable manner at an early age [12]. In example one, the kid was managed with tell-show-do, distraction, nitrous oxide, oral conscious sedation, and positive reinforcement. In case two, the youngster had hospital treatment under general anaesthesia because of severe ASD and extreme dental anxiety. DGI-II-affected primary teeth have weak enamel and early dentin exposure, which causes significant attrition that, happens quickly [13]. Consequently, it’s critical to establish an early diagnosis and appropriate treatment. Due to the two children’s behaviour, severity, and age (primary versus mixed dentition), two distinct treatment approaches were offered in this case study, which also addressed the parent’s main concern. The biochemical characteristics of enamel and dentin are weakened as the illness progresses to the gingival level, affecting adhesion strength and reducing the possibilities for restorative care. In the first instance, for instance, the youngster arrived at the clinic at a more advanced stage of the illness, with all of the teeth suffering from significant attrition and some of them being abscessed and irreparable. In that instance, a full overlay denture was the patient’s best long-term treatment option to address both the mother’s primary complaint and the child’s condition. A partial or full removable denture that is made over teeth that are still in place or the roots of teeth that are not prepped with a coping to interface with the denture is known as an overlay denture [14]. A full mouth dental rehabilitation of the patient’s main teeth may have been carried out by using SSC and cosmetic prefabricated crowns if the patient had been seen sooner. In order for parents to be aware of the various problems that may arise when their children move into permanent dentition, it is crucial that DGI patients receive an early diagnosis and education. With the recent eruption of permanent teeth in the second patient, who had an early mixed dentition, we were able to repair the anterior teeth with aesthetic restorations and the posterior teeth with SSCs. Every six months, the patients were scheduled for an oral examination, dental prophylaxis, training on proper oral hygiene, and, in the first instance, denture modification if needed due to the child’s growth potentially requiring relining or denture replacement [14]. When growth is finished, follow-up care should ideally be continued until an implant may be inserted [15]. An additional option for the overlay denture’s manufacture was to include an expansion screw and, if necessary, start expanding to accommodate the denture’s increased transverse dimension. This reduces the need to completely rebuild the appliance.
- CONCLUSION
Getting a good prognosis for DGI requires early diagnosis and treatment. It is crucial to use a multidisciplinary approach to restore the function as well as the appearance of the remaining teeth. When a child with severe DGI receives prosthodontics rehabilitation in the latter stages of their primary dentition, function and aesthetics are greatly enhanced, and the patient’s psychological well-being is also greatly enhanced. We recognise the significance of additional study in this field even though there is no confirmed connection between ASD and SCT with DGI.
REFERENCES
- Barron, M.J.; McDonnell, S.T.; Mackie, I.; Dixon, M.J. Hereditary dentine disorders: Dentinogenesis imperfecta and dentine dysplasia. Orphanet J. Rare Dis.2008, 3, 31.
- Thotakura, S.R.; Mah, T.; Srinivasan, R.; Takagi, Y.; Veis, A.; George, A. The non-collagenous dentin matrix proteins are involved in dentinogenesis imperfecta type II (DGI-II). Dent. Res.2000, 79, 835–839.
- De La Dure-Molla, M.; Philippe Fournier, B.; Berdal, A. Isolated dentinogenesis imperfecta and dentin dysplasia: Revision of the classification. J. Hum. Genet.2015, 23, 445–451.
- Shields, E.D.; Bixler, D.; El-Kafrawy, A.M. A proposed classification for heritable human dentine defects with a description of a new entity. Oral Biol.1973, 18, 543–553.
- Beattie, M.L.; Kim, J.W.; Gong, S.G.; Murdoch-Kinch, C.A.; Simmer, J.P.; Hu, J.C. Phenotypic variation in dentinogenesis imperfecta/dentin dysplasia linked to 4q21. Dent. Res.2006, 85, 329–333.
- Zhang, H.; Xie, X.; Liu, P.; Liang, T.; Lu, Y.; Qin, C. Transgenic expression of dentin phosphoprotein (DPP) partially rescued the dentin defects of DSPP-null mice. PLoS ONE2018, 13, e0195854.
- Qin, C.; Cook, R.G.; Orkiszewski, R.S.; Butler, W.T. Identification and characterization of the carboxyl-terminal region of rat dentin sialoprotein. Biol. Chem.2001, 276, 904–909.
- Guo, S.; Lim, D.; Dong, Z.; Saunders, T.L.; Ma, P.X.; Marcelo, C.L.; Ritchie, H.H. Dentin Sialophosphoprotein: A Regulatory Protein for Dental Pulp Stem Cell Identity and Fate. Stem Cells Dev.2014, 23, 2883–2894.
- Radlanski, R.J.; Renz, H. Developmental movements of the inner enamel epithelium as derived from micromorphological features. J. Oral. Sci.2006, 114 (Suppl. 1), 343–348.
- Jiang, Y.; Spears, I.R.; Macho, G.A. An investigation into fractured surfaces of enamel of modern human teeth: A combined SEM and computer visualisation study. Oral Biol.2003, 48, 449–457.
- Sarah Gul Rehman & Deepak Singh. Thalassemia Consequences and Survival Rates in South Asian Kids and Adults. Dinkum Journal of Medical Innovations, 2(05):194-200.
- Rubab Rasheed & Manisha Nagpal. Psychosocial issues in Parents and Patients with Thalassemia. Dinkum Journal of Medical Innovations, 2(05):188-193.
- Dua Zahra & Parshu Ram Chaudhary. Women’s Nutritional Variability and Domestic Food Safety in Rural and Semi-Urban Communities. Dinkum Journal of Medical Innovations, 2(05):182-187.
- Pradip Rijal. Advances of NGS in Understanding of Epilepsy Genetics and Recent Discoveries of Gene in Monogenic Epilepsies. Dinkum Journal of Medical Innovations, 2(05):170-181.
- Pradip Rijal, Aatiqa Tariq & Syeda Hajra Batool. The Study of Differential Expression of Genes Controlling Reproductive Function in Immune Cells of PCOS Women. Dinkum Journal of Medical Innovations, 2(05):157-169.
Publication History
Submitted: May 05, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0119
Citation
Nabeela Riaz, Rabia Zulfiqar, Muhammad Naveed Akhter & Msooma Sheikh (2023). Dentinogenesis Imperfecta type II Underwent Whole Mouth Rehabilitation Employing Various Treatment Modalities. Dinkum Journal of Medical Innovations, 2(06):201-206.
Copyright
© 2023 DJMI. All rights reserved