

")
Publication History
Submitted: May 02, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0120
Citation
Asbin Bandhari, Syeda Hajra Batool, Aatiqa Tariq, Abdullah Hassan, Pooja Bhanarjee & Parshu Ram (2023). A Comprehensive Analysis of Neurosurgeons’ Conversations to Preserve Non-Traditional Brain Networks. Dinkum Journal of Medical Innovations, 2(06):207-216.
Copyright
© 2023 DJMI. All rights reserved
207-216
A Comprehensive Analysis of Neurosurgeons’ Conversations to Preserve Non-Traditional Brain NetworksReview Article
Asbin Bandhari 1*, Syeda Hajra Batool 2, Aatiqa Tariq 3, Abdullah Hassan 4, Pooja Bhanarjee 5, Parshu Ram 6
- Nepal Medical College and Teaching Hospital (NMC), Nepal: asbinbandhari@gmail.com
- Lahore Garrison University, Pakistan; meetwithsyeda@gmail.com
- Hazara University, Mansehra, Pakistan; atiqa.tariq@yahoo.com
- King Edward Medical University, Mayo Hospital, Lahore; wajiulhassan1022@gmail.com
- Nepal Medical College and Teaching Hospital (NMC), Nepal: poojabanarjee1@gmail.com
- Nepal Medical College and Teaching Hospital (NMC), Nepal: parshuram88@outlook.com
* Correspondence: meetwithsyeda@gmail.com
Abstract: Despite being well-established in neuroscience, the significance of large-scale brain networks in higher-order human functioning has not yet permeated neurosurgery thought due to worries about therapeutic applicability. In this work, we carried out the first comprehensive review investigating the clinical utility of non-conventional, large-scale brain networks, such as the networks for default mode (DMN), ventral attention (VAN), salience (SN), central executive (CEN), and dorsal attention (DAN). Included were studies that documented evidence of emotional, cognitive, or neurologic abnormalities related to injury or malfunction in these networks. After screening 22,697 PubMed articles, we included and scrutinized 551 full-text papers. In different proportions (36–56%), cognitive deficits were the most prevalent symptom of network disturbances. These were most commonly associated with disruption of the DMN (n = 213) or a combination of the DMN, CEN, and SN networks (n = 182). When CEN was disrupted, there were a higher percentage of motor symptoms (12%), whereas SN disruption was associated with emotional symptoms (35%), language/speech deficiencies (24%), or both. Cognitive deficits were largely caused by disruptions to the attention networks (VAN/DAN) with other networks or each other (56%). There is a wealth of data that supports the clinical significance of non-conventional, large-scale brain networks and indicates that neurosurgical patients should benefit by maintaining these neural networks.
Keywords: neurosurgeons, discussions, connectome, neurosurgery, brain tumor, attention network
- INTRODUCTION
Historically, neurosurgeons have dedicated a significant amount of their time to trying to avoid damage to the brain’s “eloquent” regions. In resective brain surgery, we may now preserve motor and linguistic functions while increasing the degree of resection because to groundbreaking developments in intraoperative brain mapping and neuroimaging technologies [1,2]. Nonetheless, it is also evident that patients with gliomas frequently exhibit more subtle abnormalities in higher-order complex activities following surgery [3,4,5, 6]. Brain tumor surgery frequently causes disruptions to complex neuro-behavioral skills, including memory, attention, executive functioning, and emotion, which can make it difficult for patients to reintegrate into society and the workforce [7]. As a result, some people are becoming more interested in minimizing the cognitive impact of supratentorial, intra-axial brain tumor surgery [8]. Prior to this, there has been some confusion about precisely what can and cannot be done during surgery to prevent these issues, which has hindered our capacity to maximize post-operative cognitive morbidity. The neurosurgical community has traditionally retained a less extensive knowledge with anatomy responsible for higher-order activities, despite a significant increase in our study and subsequent understanding of the brain anatomy responsible for language and motor functions over the last few decades. Big brain networks are one idea that has come out of the neuroscience area that could help with this problem. These networks are frequently studied using changes in blood oxygenation as a proxy for functional connectivity. They include repeatable regions that show highly synchronized activity based on certain functions or at rest [9, 10]. In a structural network, functionally related regions are virtually always connected by large-scale white matter connections, as evidenced by the discovery made more recently [11,12,13,14,15]. This shows that regions that fire together are also interconnected together. More accurate maps and localisation of complicated patient symptomology that is not limited to discrete cortical regions have been made possible by information on the structural and functional connectome [16, 17]. The significance of the large-scale brain networks has not yet permeated conventional neurosurgical thought, despite a substantial corpus of research in the field of neuroscience endorsing this idea. The lack of a systematic review of the clinical evidence and significance pertaining to non-traditional, large-scale brain networks other than language and motor systems may be one reason for this stagnation. This could lead some people to conclude that these networks are unimportant for neurosurgery. As different neurological disorders and their symptomology may frequently be better understood by taking into account their impact on networks [16], neglecting to take brain network architecture into account impedes our community’s successful progress toward customized neurosurgical treatments. Here, we therefore make an effort to allay these worries by doing a thorough review that looks at and summarizes the substantial amount of research that is currently accessible on the subject. We also raise the very real possibility that the characteristics reported in previous articles also apply to brain tumor patients and may need to be further investigated in the future. We present and debate the significance of non-traditional eloquent areas in neurosurgery through a succinct systematic review, particularly in relation to impairment or dysfunction in the large-scale brain networks: the ventral attention network (VAN), salience network (SN), dorsal attention network (DAN), default mode network (DMN), and central executive network (CEN).
- MATERIALS AND METHODS
In compliance with the Recommended Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) standards, a systematic review was carried out. A thorough screening procedure was carried out with the use of the digitized PubMed repository. Some of the following keywords were used in a search string: “default mode OR central executive OR salience network OR sensorimotor OR language” AND “memory OR language OR speech OR motor function OR attention OR depression OR neurologic deficit.” August 1, 2021, was the date of this search, which covered the years 2011–2023. Included were articles that illustrated the significance of large-scale, non-traditional brain networks in relation to general illness states or clinical symptoms. The following criteria were met by the included articles: (1) they specified fMRI or DTI techniques; (2) they talked about the DMN, CEN, SN, DAN, VAN, or related connections and network names; and (3) they talked about network dysfunction or damage in relation to neurologic, cognitive, or emotional deficits. We also looked at articles that provided a clear definition of a disease state by comparing it to healthy controls based on certain network changes. If the aforementioned requirements were satisfied, all article kinds—including reviews and conference abstracts—were included. Only healthy patients or well-known networks, including language or motor networks, were not allowed to appear in any of the articles. Researches that could not offer a text in English or that were solely methodological in nature were also disqualified. M.S. finished the title and abstract screening, while N.D. finished the full-text review. Based on particular elements addressed, such as the network implicated, the type of damage or malfunction of the network, the illness state, and the specific clinical symptoms implicated, the included full-texts underwent a thorough qualitative analysis (N.D.). Every item received a grade of M.D. according to the category of evidence that was presented.
- RESULTS AND DISCUSSION
1315 articles underwent full-text review out of 22,697 that were screened in total (Figure 1).

Figure 1: PRISMA Flow Chart
A summary of the 551 full-text papers that made up the final analyses is provided. The majority of the included studies (n = 524, 95%) indicated class III evidence and were of intermediate research quality. Rather than using DTI to assess network damage or structural integrity (n = 52, 9%), functional connectivity analyses, such as resting-state fMRI, were mostly used to investigate networks for dysfunction (n = 436, 79%). In n = 63 (11%) investigations, combined structural-functional analyses were used to investigate the link between network dysfunction and the underlying structural network damage. The majority of diagnoses (n = 124) reported in the included studies were for depression. Subsequently, there were 81 cases of schizophrenia, 64 cases of Parkinson’s disease, 46 cases of Alzheimer’s disease, 40 cases of stroke, 29 cases of epilepsy, and 21 cases of tumors. The bulk of the articles found in the current study were represented by the DMN (n = 213, 39%). Numerous studies looked at the consequences of network interruptions in combination; therefore they were further divided into the most frequently evaluated combinations. With n = 182, 33%, a triple network model including the DMN, CEN, and/or SN was the next most often investigated network. Comparably, only one study [18] looked at the attention networks (VAN and DAN) alone; most studies (n = 93, 17%) looked at the attention networks in conjunction with the other brain networks or with each other. In the current analysis, only a small number of studies (n = 25, 5%) were found on the CEN. Nevertheless, some studies that addressed the superior longitudinal fasciculus—a significant fiber bundle connecting the CEN—were disregarded because they did not address the CEN specifically. Deficits in cognitive functions (n = 226, 41%), including executive functioning, memory, and attention processing, were the most often found effects of network disruptions. Deficits in emotional processing were seen in 26% (n = 143) of the investigations after this, primarily in relation to affective features in depression and/or anxiety. Numerous studies were found to show deficiencies in multiple outcomes, including language or speech (4%), motor alone (4%), emotion and cognition (6%), motor and cognition (5%), and many other abnormalities together (7%). The CEN and SN displayed the greatest range of symptoms in terms of frequency; there was a discernible increase in motor symptoms with the CEN (12%) and language processing or speaking issues with the SN (24%). The most common cause of cognitive impairments was disruption of the attention networks (VAN/DAN) alone or in combination with other networks (56%). In this study, we offer the results of the first thorough examination of the literature on significant non-traditional large-scale brain networks in the context of neurosurgery. A large corpus of reliable research has connected disruptions in non-traditional networks to serious deficits in the domains of emotion, neurology, and cognition. The material that is at present accessible seems to indicate that disruption of major brain network regions or the fibers that connect them will induce at least some inadequacies, even though the precise mechanism underlying a given neurologic impairment is yet unknown. However, this material has only been mentioned in passing and has not yet been properly investigated in a way that may demonstrate its therapeutic significance for standard neurosurgical cognitive processes. Drawing on previous studies and current neurosurgical techniques, we will attempt to briefly summarize the relative relevance of these neuroanatomic substrates below, because they are frequently met during reconstructive brain surgery. We will also explain how features that show up in many articles can be very relevant to brain tumor patients. It is noteworthy that this analysis provides, as a first step, a thorough synopsis of the potential therapeutic utility of these networks and how regularizing their presence in neurosurgical cognitive processes could eventually result in a more sophisticated and customized approach to connectome-based neurosurgery. The organizing concept of the structural and functional brain connectome has been found to be based on brain networks. Though many neurosurgical experts may not be familiar with them, it’s important to keep in mind that the default mode, central executive, salience, dorsal attention, and ventral attention networks are well-established among the greater neuroscientific community. Over the past 20 years, these networks have also been the subject of in-depth research. These networks are made up of highly synchronized cortical areas and the white matter bundles that run between them. In the context of reconstructive brain surgery, patients’ ability to support complex human functions and their level of metabolic efficiency depend on the preservation of the structural integrity of large-scale networks. The DMN, CEN, and SN are the three canonical resting-state networks that define an axis by which the other networks align for complex neuro-behavioral activities and reside at the top of the network hierarchy (Figure 2).
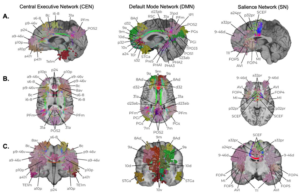
Figure 2 Cognitive Control Networks. The anatomic locations of the Default Mode Network (DMN), Salience Network (SN), and Central Executive Network (CEN) are presented in sagittal (A), axial (B), and coronal slices (C). Individual parcellations are indicated according to the established Glasser Parcellation Scheme of the Human Connectome Project [24] based on network affiliation [25].
Results from the current work strongly suggest that disturbance of these networks can regularly result in cognitive and emotional deficiencies, which are also assumed to be the cause of a variety of neuro-psychiatric diseases including depression [19], despite the fact that this has only been briefly explored earlier [8]. On the other hand, attention networks primarily function in tangent relationships with other large-scale networks to process stimuli both top-down and bottom-up, and to realign attention according to both internal and external incentives (Figure 3) [11,20,21]. It should come as no surprise that interference with the VAN or DAN, when combined with the other higher-order networks, most frequently results in cognitive deficits such memory loss [23] and spatial neglect [22]. It is probably safe to say that these five networks are more significant than previously thought, and it is worth considering whether they need to be preserved given that they appear to be a common feature that explains much of the human functioning we understand in neuroscience and are frequently encountered during reconstructive brain surgery.
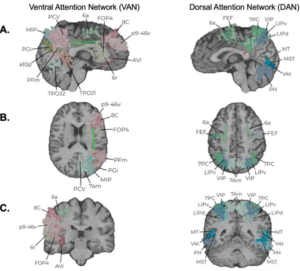
Figure 3 Attention Networks. The anatomic locations of the Dorsal Attention Network (DAN) and Ventral Attention Network (VAN) are presented in sagittal (A), axial (B), and coronal slices (C). Individual parcellations are indicated according to the established Glasser Parcellation Scheme of the Human Connectome Project [24] based on network affiliation [25].
There isn’t a single randomized controlled study that demonstrates better neurological outcomes come from sparing one of these five large-scale, unconventional networks after surgery. Despite this drawback, there is a substantial body of research supporting the notion that disruption or injury to these networks results in emotional, neurological, or cognitive disorders, and they ought to be taken into account. In the context of neuro-psychiatric illnesses, where a distinct neuroanatomic substrate or lesion is not easily identifiable, the majority of prior literature has concentrated on network disturbances. In these cases, the pathophysiology is unmistakably characterized by widespread dysfunction across multiple spatially distant regions involved in interacting networks [26, 27]. But due to similar network abnormalities that change neuronal connections, psychiatric symptoms can frequently be the predominant and only symptoms of brain tumors as well [28,29], a fact that has just lately come to light. Because there are definite deficiencies and broad consequences linked to the disruption of these five non-traditional networks when important network regions or fibers are severed, decisions made during reconstructive brain surgery may also benefit from taking these non-traditional networks into account, even though the mechanisms of disruption may differ slightly [30, 31].
According to this evaluation, a substantial percentage of research showed emotional and cognitive impairments within the framework of several interconnected brain networks. This is not surprising, since the majority of higher-order activities depend on several dynamic interactions amongst higher-order networks, including the DMN, CEN, and SN, rather than being limited to a single area of brain tissue. An increasing number of lines of evidence [19, 30–32] have shown how important these cognitive control networks are, including those involving brain tumors, strokes, and mental health patients. All of these findings point to the possibility that disruption in these networks—which frequently occurs after damage to the medial frontal lobe—may result in abnormally distributed cognitive resources among networks, which could lead to cognitive and psychomotor disorders [30,31, 33]. Butterfly gliomas, which frequently encircle non-traditional networks like the DMN and/or SN, provide an illustration of this. When they are injured during surgery, they can cause akinetic mutism and post-operative abulia [33]. Even while there are obvious advantages to having a better understanding of the brain connectome architecture in neurosurgical patients, there are still a number of areas that need investigation in order to fully utilize this knowledge. Significantly, it remains unclear how we are to determine whether a network that has been overtaken by a tumor can be saved. In certain cases, attempting to salvage a network may not be surgically viable or practical, while in other cases, leaving residual tumor in a network may not be ultimately worth it if the tumor is disturbing a core network region. In addition, it’s not evident if a tumor may be removed while maintaining the integrity of the underlying network, as an auditory neuroma, for instance, could [34]. Given that a large percentage of the human brain is known to preserve some degree of redundancy, this is an excellent subject for connectomics research in the future [35]. Because most functions are bi-hemispherically processed, a significant portion of this redundancy most certainly originates in the contralateral hemisphere. Preserving the transcallosal fibers in this network (also known as “crossed FAT”) while operating in the SMA with a tumor entering the salience network may help patients recover from SMA syndrome [36]. However, our experience has shown that, in certain cases—such as with the default mode network—the other side of a network does not always adequately make up for losses in the core of the network, and this should be taken into account going forward. To generate therapeutically useful metrics that can quantify these neurological properties, improved statistical modeling tools of the brain connectome are being developed; nevertheless, additional clinical research is required [37]. The entire network’s functionality is probably disrupted if this network’s central portion or important fibers that connect it to all other frontal and parietal parcellations are damaged. It is uncertain, nevertheless, whether part of the frontal cluster or peripheral parcellations may be sacrificed without impairing network functionality as a whole, and there are instances in which surgically severing these regions from the network results in moderate clinical abnormalities. These are just a few of the crucial issues that need to be the focus of upcoming studies. But it’s vital to understand that the reason these answers are still unknown is that, until now, there hasn’t been a standard terminology for analyzing these networks, and there haven’t been enough resources available for fruitful conversations and the development of technological improvements in this field. Going forward, frequent neurosurgical thought processes that take into account non-traditional brain networks will offer more chances to maximize the patient’s onco-functional balance after reconstructive brain surgery.
- CONCLUSION
A significant amount of credible evidence points to the possibility that serious neurological, cognitive, or emotional deficiencies could be brought on by injury or failure in the non-traditional, large-scale brain networks. Many aspects of complex human functioning are currently understood by the neuroscientific community to be explained by the default mode, central executive, salience, dorsal attention, and ventral attention networks. As such, the question of whether it is necessary to preserve these non-traditional “eloquent” regions should be considered in routine neurosurgical thought going forward. To improve our knowledge of and capacity to improve cognitive outcomes after brain surgery, increased use of thorough pre- and post-operative neurocognitive assessments is still important. These results should be correlated with information on network disruptions in larger trials.
REFERENCES
- Young, J.S.; Lee, A.T.; Chang, E.F. A Review of Cortical and Subcortical Stimulation Mapping for Language. Neurosurgery 2021, 89, 331–342.
- Vigneswaran, K.; Sawaya, R. Role of Resection of Glioblastoma: Can Technology Overcome Biology? Neurosurgery 2020, 67, 4–14.
- Drewes, C.; Sagberg, L.M.; Jakola, A.S.; Solheim, O. Perioperative and Postoperative Quality of Life in Patients with Glioma–A Longitudinal Cohort Study. World Neurosurg. 2018, 117, e465–e474.
- Dhandapani, M.; Gupta, S.; Mohanty, M.; Gupta, S.K.; Dhandapani, S. Trends in cognitive dysfunction following surgery for intracranial tumors. Surg. Neurol. Int. 2016, 7, S190–S195.
- Herbet, G.; Moritz-Gasser, S. Beyond Language: Mapping Cognition and Emotion. Neurosurg. Clin. N. Am. 2019, 30, 75–83.
- Rijnen, S.J.M.; Kaya, G.; Gehring, K.; Verheul, J.B.; Wallis, O.C.; Sitskoorn, M.M.; Rutten, G.M. Cognitive functioning in patients with low-grade glioma: Effects of hemispheric tumor location and surgical procedure. J. Neurosurg. 2019, 133, 1671–1682.
- Starnoni, D.; Berthiller, J.; Idriceanu, T.-M.; Meyronet, D.; d’Hombres, A.; Ducray, F.; Guyotat, J. Returning to work after multimodal treatment in glioblastoma patients. Neurosurg. Focus FOC 2018, 44, E17.
- Dadario, N.B.; Brahimaj, B.; Yeung, J.; Sughrue, M.E. Reducing the Cognitive Footprint of Brain Tumor Surgery. Front. Neurol. 2021, 12, 711646.
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The brain’s default network: Anatomy, function, and relevance to disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38.
- Sarah Gul Rehman & Deepak Singh. Thalassemia Consequences and Survival Rates in South Asian Kids and Adults. Dinkum Journal of Medical Innovations, 2(05):194-200.
- Rubab Rasheed & Manisha Nagpal. Psychosocial issues in Parents and Patients with Thalassemia. Dinkum Journal of Medical Innovations, 2(05):188-193.
- Dua Zahra & Parshu Ram Chaudhary. Women’s Nutritional Variability and Domestic Food Safety in Rural and Semi-Urban Communities. Dinkum Journal of Medical Innovations, 2(05):182-187.
- Pradip Rijal. Advances of NGS in Understanding of Epilepsy Genetics and Recent Discoveries of Gene in Monogenic Epilepsies. Dinkum Journal of Medical Innovations, 2(05):170-181.
- Pradip Rijal, Aatiqa Tariq & Syeda Hajra Batool. The Study of Differential Expression of Genes Controlling Reproductive Function in Immune Cells of PCOS Women. Dinkum Journal of Medical Innovations, 2(05):157-169.
- Fox, M.D. Mapping Symptoms to Brain Networks with the Human Connectome. N. Engl. J. Med. 2018, 379, 2237–2245.
- O’Neal, C.M.; Ahsan, S.A.; Dadario, N.B.; Fonseka, R.D.; Young, I.M.; Parker, A.; Maxwell, B.D.; Yeung, J.T.; Briggs, R.G.; Teo, C.; et al. A connectivity model of the anatomic substrates underlying ideomotor apraxia: A meta-analysis of functional neuroimaging studies. Clin. Neurol. Neurosurg. 2021, 207, 106765.
- Bezdicek, O.; Ballarini, T.; Růžička, F.; Roth, J.; Mueller, K.; Jech, R.; Schroeter, M.L. Mild cognitive impairment disrupts attention network connectivity in Parkinson’s disease: A combined multimodal MRI and meta-analytical study. Neuropsychologia 2018, 112, 105–115.
- Kaiser, R.H.; Andrews-Hanna, J.R.; Wager, T.D.; Pizzagalli, D.A. Large-Scale Network Dysfunction in Major Depressive Disorder: A Meta-analysis of Resting-State Functional Connectivity. JAMA Psychiatry 2015, 72, 603–611.
- Allan, P.G.; Briggs, R.G.; Conner, A.K.; O’Neal, C.M.; Bonney, P.A.; Maxwell, B.D.; Baker, C.M.; Burks, J.D.; Sali, G.; Glenn, C.A.; et al. Parcellation-based tractographic modeling of the dorsal attention network. Brain Behav. 2019, 9, e01365.
- Corbetta, M.; Shulman, G.L. Control of goal-directed and stimulus-driven attention in the brain. Nat. Rev. Neurosci. 2002, 3, 201–215.
- Corbetta, M.; Shulman, G.L. Spatial neglect and attention networks. Annu. Rev. Neurosci. 2011, 34, 569–599.
- Mallas, E.J.; De Simoni, S.; Scott, G.; Jolly, A.E.; Hampshire, A.; Li, L.M.; Bourke, N.J.; Roberts, S.A.G.; Gorgoraptis, N.; Sharp, D.J. Abnormal dorsal attention network activation in memory impairment after traumatic brain injury. Brain 2021, 144, 114–127.
- Glasser, M.F.; Coalson, T.S.; Robinson, E.C.; Hacker, C.D.; Harwell, J.; Yacoub, E.; Ugurbil, K.; Andersson, J.; Beckmann, C.F.; Jenkinson, M.; et al. A multi-modal parcellation of human cerebral cortex. Nature 2016, 536, 171–178.
- Yeo, B.T.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zollei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165.
- Liu, J.; Xu, X.; Zhu, C.; Luo, L.; Wang, Q.; Xiao, B.; Feng, B.; Hu, L.; Liu, L. Disrupted Structural Brain Network Organization Behind Depressive Symptoms in Major Depressive Disorder. Front. Psychiatry 2020, 11, 565890.
- Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends Cogn. Sci. 2011, 15, 483–506.
- Bartolomei, F.; Bosma, I.; Klein, M.; Baayen, J.C.; Reijneveld, J.C.; Postma, T.J.; Heimans, J.J.; van Dijk, B.W.; de Munck, J.C.; de Jongh, A.; et al. How do brain tumors alter functional connectivity? A magnetoencephalography study. Ann. Neurol. 2006, 59, 128–138.
- Madhusoodanan, S.; Ting, M.B.; Farah, T.; Ugur, U. Psychiatric aspects of brain tumors: A review. World J. Psychiatry 2015, 5, 273–285.
- Briggs, R.G.; Allan, P.G.; Poologaindran, A.; Dadario, N.B.; Young, I.M.; Ahsan, S.A.; Teo, C.; Sughrue, M.E. The Frontal Aslant Tract and Supplementary Motor Area Syndrome: Moving towards a Connectomic Initiation Axis. Cancers 2021, 13, 1116.
- Young, J.S.; Gogos, A.J.; Aabedi, A.A.; Morshed, R.A.; Pereira, M.P.; Lashof-Regas, S.; Mansoori, Z.; Luks, T.; Hervey-Jumper, S.L.; Villanueva-Meyer, J.E.; et al. Resection of supplementary motor area gliomas: Revisiting supplementary motor syndrome and the role of the frontal aslant tract. J. Neurosurg. 2021, 1–7.
- Darby, R.R.; Joutsa, J.; Burke, M.J.; Fox, M.D. Lesion network localization of free will. Proc. Natl. Acad. Sci. USA 2018, 115, 10792–10797.
- Burks, J.D.; Bonney, P.A.; Conner, A.K.; Glenn, C.A.; Briggs, R.G.; Battiste, J.D.; McCoy, T.; O’Donoghue, D.L.; Wu, D.H.; Sughrue, M.E. A method for safely resecting anterior butterfly gliomas: The surgical anatomy of the default mode network and the relevance of its preservation. J. Neurosurg. 2017, 126, 1795–1811.
- Darby, R.R.; Joutsa, J.; Fox, M.D. Network localization of heterogeneous neuroimaging findings. Brain 2018, 142, 70–79.
- Dadario, N.B.; Zaman, A.; Pandya, M.; Dlouhy, B.J.; Gunawardena, M.P.; Sughrue, M.E.; Teo, C. Endoscopic-assisted surgical approach for butterfly glioma surgery. J. Neurooncol. 2022, 156, 635–644.
- Jenkins, L.M.; Drummond, K.J.; Andrewes, D.G. Emotional and personality changes following brain tumour resection. J. Clin. Neurosci. 2016, 29, 128–132.
- Duffau, H. Mapping the connectome in awake surgery for gliomas: An update. J. Neurosurg. Sci. 2017, 61, 612–630.
Publication History
Submitted: May 02, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0120
Citation
Asbin Bandhari, Syeda Hajra Batool, Aatiqa Tariq, Abdullah Hassan, Pooja Bhanarjee & Parshu Ram (2023). A Comprehensive Analysis of Neurosurgeons’ Conversations to Preserve Non-Traditional Brain Networks. Dinkum Journal of Medical Innovations, 2(06):207-216.
Copyright
© 2023 DJMI. All rights reserved