

")
Publication History
Submitted: May 03, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0122
Citation
John H. Marshal, Robert Downey & Olivia James (2023). Adult Participant with Corpus Callosum Infarction and Thyroid Storm Exacerbate. Dinkum Journal of Medical Innovations, 2(06):229-235.
Copyright
© 2023 DJMI. All rights reserved
229-235
Adult Participant with Corpus Callosum Infarction and Thyroid Storm ExacerbateCase Study
John H. Marshal 1*, Robert Downey 2, Olivia James 3
- The First Hospital of Jilin University, China: marshal_hjohn@jlu.edu.cn
- The First Hospital of Jilin University, China: downyrobert@jlu.edu.cn
- The First Hospital of Jilin University, China: oliviajames@jlu.edu.cn
* Correspondence: marshal_hjohn@jlu.edu.cn
Abstract: A 38-year-old male patient with a history of hyperthyroidism was brought to the hospital due to palpitations, fever, excessive perspiration, and a mild decline in left limb muscle power. The findings of the laboratory tests verified the diagnosis of TS. Following treatment, the patient’s clinical symptoms progressively became better. However, the bilateral pathological symptoms were favorable at the same time that his left limb muscle strength gradually declined. The pons and corpus callosum showed signs of acute cerebral infarction on magnetic resonance imaging (MRI) of the head. Thyroid storm was diagnosed, along with significant basilar artery blockage or stenosis and acute cerebral infarction of the corpus callosum and pons. The patient was given 20 mg of propranolol three times a day by nasal feeding, 300 mg of hydrocortisone intravenously, and 200 mg of propylthiouracil tablets three times a day. In order to stop platelets from aggregating, aspirin and clopidogrel were given, while atorvastatin calcium was given to reduce cholesterol and stabilize plaques. The patient was able to walk beside the bed with assistance after his left limb muscle strength returned to a grade 4+ level. Thyroid function was improved at the same time. Patients with thyroid storm should have thorough physical examinations, and head imaging tests should be enhanced to detect brain damage early.
Keywords: cerebral infarction, corpus callosum, hyperthyroidism, thyroid storm (TS)
- INTRODUCTION
Thyroid storms are uncommon, sometimes fatal endocrine emergencies that result in widespread organ malfunction and are predominantly brought on by elevated levels of thyroid hormones in the bloodstream [1]. It mainly affects patients who have long-term untreated or insufficiently treated hyperthyroidism [2]. Though it can strike at any age, TS is more common in women [3]. A prevalent condition that mostly affects middle-aged and older people is cerebral infarction. Young people rarely get cerebral infarction, which is frequently a result of cerebral arteritis, hyperthyroidism, and moyamoya disease. One percent of young individuals with hyperthyroidism experienced an ischemic stroke, according to a recent epidemiological study [4]. Thyroid storm plus acute ischemic stroke, however, is an uncommon symptom that raises the mortality rate. Reducing death and morbidity rates requires early detection and prompt treatment. The most important associative fiber linking homologous sites in both hemispheres is the corpus callosum, which is situated at the base of the interhemispheric fissure [5]. The anterior and posterior circulations both send blood to the well supplied corpus callosum. Thus, in clinical practice, corpus callosum infarction is uncommon. To the best of our knowledge, this is the first case report of thyroid storm complicated by acute corpus callosum infarction anywhere in the globe.
- CASE PRESENTATION
A 38-year-old man was brought to our hospital with palpitations and irritable symptoms that he had been experiencing for four years. For one day, the guy’s symptoms had gotten worse due to fatigue, fever, and profuse perspiration. Two years prior, the patient presented with symptoms of proptosis, tremors, frustration, and cervical elongation. These findings led to the diagnosis of hyperthyroidism. On the other hand, the patient did not routinely review or take her medication. He had runny nose and sinus congestion two days earlier, but he decided not to investigate more. The day before, he felt exhausted, palpitations, fever (38.5°C), profuse sweating, vomiting, headache, and dizziness. He denied ever having high blood pressure, diabetes, or coronary heart disease. He’d smoked for twenty-six years, about 20 cigarettes a day, and he drank on occasion. Upon examination, the body temperature was 38.5°C, the pulse rate was 143 beats per minute, the respiration rate was 22 beats per minute, and the blood pressure was 142/92 mmHg (1 mmHg=0.133 kPa). He was restless, had mild exophthalmos, slurred speech, dry skin, and trembling in his limbs. A vascular murmur, firm palpation, diffuse bilateral thyroid enlargement (grade II), feeble movement, and the absence of a noticeable tremor were all found during auscultation. His breathing sounds were harsh in both lungs, and he had phlegm and wet rales at the base of both lungs. The cardiac border was normal, the heart rate was 143 beats per minute, the rhythm and heart sounds were normal, and there were no murmurs or additional heart sounds detectable in the auscultation area of each valve. There were no clinical signs on either side, and the muscle strength of the left leg was grade 4, whereas the right limb had grade 5. No glaringly obvious positive indicators were found during the remainder of the inspection. There were normal blood and coagulation levels along with normal levels of procalcitonin, high-sensitivity C-reactive protein, myocardial damage markers, urine, and stool. On a head CT scan, suspicious hypodense shadows were observed in the pons and corpus callosum (Fig. 1).
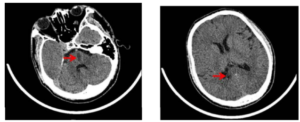
Figure 1: Computed tomography of the head revealed suspicious hypodense shadows in the pons and corpus callosum
Sputum retention in the trachea, bronchitis in the right upper lobe, bilateral lower lobe inflammation, and the right main and upper lobe bronchi were all discovered by a lung CT scan. The Burch-Wartofsky scoring scale, Acute Physiology and Chronic Health Evaluation II, and Sequential Organ Failure Evaluation scores were 80, 11, and 5 points, respectively, when paired with the patient’s medical history, physical examination, and pertinent tests. It turned out to be a thyroid storm. The patient got three daily nasal feedings of 200 mg propylthiouracil, one daily intravenous infusion of 300 mg hydrocortisone, and three daily nasal feedings of 20 mg propranolol. Additional symptomatic treatments included enteral feeding, rehydration, anti-infection, and paracetamol cooling. After receiving treatment for six days, the patient’s condition improved generally; there was no tremor in the limbs, a first-degree thyroid enlargement, and a normal heart rate and body temperature. A neurological examination revealed, however, that the neck was soft, the corners of the mouth were not crooked, the tongue was centered, the corners of the mouth were not crooked, and the strength of the muscles in the left and right limbs was grade 3 for the left and grade 5 for the right. He had normal and symmetrical deep and superficial sensations, as well as normal muscular tone in his extremities. He had a 4 on the National Institutes of Health Stroke Scale. Acute and subacute lacunar infarctions of the corpus callosum and pons, as well as multiple lacunar cerebral infarctions in the brain, were discovered by the head MRI scan and diffusion testing (Fig. 2).
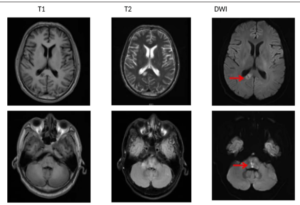
Figure 2: The head MRI scan and diffusion examination revealed an acute and subacute lacunar infarction of the corpus callosum and pons and multiple lacunar cerebral infarctions in the brain
- DISCUSSION
In clinical practice, thyroid storms are an uncommon endocrine emergency that can be lethal if left undiagnosed and untreated.(6) Infection, surgery, mental strain, iodine load, non-adherence to medicine, and other acute medical conditions are frequently identified as triggers of TS [7–11]. A survey conducted in Japan found that hospitalized patients with thyroid storm had an annual incidence of 0.2/100,000, a mortality rate of 10%–30%, and a mortality rate that was twelve times higher than that of people with thyrotoxicosis [12, 13]. Numerous neurological conditions, including chronic hyperthyroid myopathy, hyperthyroid hypokalemic periodic paralysis, and hyperthyroid myasthenia gravis, are linked to hyperthyroidism. The first instance of hyperthyroidism exacerbated by acute cerebral infarction was reported by Kushima et al. in 1991 [14]. A case of thyroid storm exacerbated by acute cerebral infarction was reported by Harada et al. in 2012 [15]. The following was discovered by the literature review: (1) During a thyroid storm, there is a large rise in the secretion of thyroid hormones, an overexcitation of sympathetic nerves, and an increase in the concentration of catecholamines in the blood, which results in minor artery spasms and increased blood viscosity. Long-term stimulation with high doses of thyroid hormone has also been shown by Czarkowsk et al. to lessen blood vessel toughness, which causes the arteries to harden [19]. Thyroid hormones can induce excessive sweating, raise heat production and oxygen consumption, and encourage oxidative phosphorylation all at the same time. This lowers the body’s effective blood volume and hemoconcentration, which eventually results in the development of cerebrovascular illnesses. The autoimmune condition known as hyperthyroidism is typified by the generation of many autoantibodies. The presence of thyroid autoantibody antigen targets in cerebral blood vessels, which trigger an inflammatory response in the blood vessel wall, was verified by Moodley et al. These cause cerebral infarction by damaging vascular endothelial cells, causing platelets to adhere to one another and aggregate to form thrombus [20, 21]. Furthermore, Zhang et al. demonstrated a correlation between cerebral artery stenosis and higher thyroid antibody levels [22]. (3) Hyperthyroidism can result in blood hypercoagulability, reduce the duration of activated partial thromboplastin time, raise fibrinogen levels, activate factor VIII and factor X, and encourage the development of intravascular microemboli [8,9,23,24]. (4) Up to 40% of patients with TS have atrial fibrillation, while the incidence of atrial fibrillation in hyperthyroidism is 13.8% [25]. According to research by Chaker et al., atrial fibrillation was found to be more common in patients with greater thyroxine (FT4) concentrations. The body secretes a lot of thyroid hormones when there is a thyroid storm. Consequently, atrial fibrillation-related cerebral infarction needs to be taken into account [26]. This patient had a two-year history of hyperthyroidism, had not had regular treatment, and had smoked for sixteen years. We hypothesize that degeneration and sclerosis of vascular endothelial cells result from persistent, chronic inflammatory activation. A thyroid storm brought on by infection can result in hemoconcentration, vasospasm, and severe cerebral infarction. Nonetheless, there are limitations to this study and uncertainty regarding the connection between thyroid storm and stroke. The possibility that this patient’s thyroid storm and acute cerebral infarction happened by accident cannot be ruled out. Thus, further investigation is still required to fully understand the pathophysiology of thyroid storm aggravated by ischemic stroke in the future. The pericallosal, anterior cerebral, posterior cerebral, anterior communicating, and posterior choroidal arteries all share a common blood supply with the corpus callosum, contributing to its rich blood supply [27]. Because the corpus callosum has a lot of collateral circulation, clinical cases of corpus callosum infarction are uncommon. According to Li et al., corpus callosum infarction occurred in 59 out of 1629 ischemic stroke patients, representing a 3.6% incidence rate [28]. The patient’s head MRA revealed a minor vision of the proximal end of the right anterior cerebral artery A2 segment, as well as partial visualization of the bilateral vertebral arteries and basilar artery. The anterior and posterior circulations are impacted by vascular lesions, which cause the corpus callosum to infarct. The most common symptoms of acute corpus callosum infarction are impairments of limb mobility, language, or cognition and mental state. The patient had slurred speech and left hemiplegia, which aligns with the clinical manifestations of acute corpus callosum infarction. The death rate is greater if an abrupt cerebral infarction complicates a thyroid storm. Thus, therapy ought to start as soon as a thyroid storm is thought to be present. Agents that reduce excessive thyroid hormones, such as iodine and anti-thyroid medications (ATDs), are the mainstay of treatment for thyroid syndrome (TS). Furthermore, glucocorticoids and beta-blockers are frequently utilized in the clinical management of TS [29]. Early inhibition of thyroid hormone secretion and suppression of the peripheral T4 to T3 transition are critical for the successful treatment of thyroid storm. According to some academics, cerebral artery angiography revealed that the stenosis site also returned to normal after treatment for patients with thyroid storm complicated by acute cerebral infarction, and the patients’ neurological damage was reversible with the improvement of hyperthyroidism [30–31]. This suggests that the key to treating thyroid storm is making progress in the illness. In this instance, as the thyroid storm subsided, the cerebral infarction symptoms progressively got better. There are a few accounts of thyroid storm complicated with various problems in addition to TS complicated with acute cerebral infarction. A few academics have documented instances of diabetic ketoacidosis that are worsened by TS [32]. It is noteworthy that inflammation might be a significant factor in the onset and progression of acute cerebral infarction and thyroid storm. The body may release large amounts of pro-inflammatory cytokines suddenly during thyroid storm, which would cause a significant inflammatory reaction. Research indicates that pyruvate kinase M2 (PKM2) contributes significantly to the pathogenesis of some inflammatory illnesses. Additionally, PKM2-mediated immunometabolic reprogramming induces an overabundance of pro-inflammatory cytokines to be released, leading to exaggerated inflammatory reactions. PKM2 may therefore have therapeutic implications for the inflammatory response that takes place during thyroid storm and may be a viable target for the treatment of associated inflammatory illnesses [33]. When there is an acute cerebral infarction, the brain’s resident immune cells, or microglia, get activated. They then release a range of proinflammatory cytokines and reactive oxygen species (ROS), which can exacerbate thyroid crisis. Restoring normalcy to the abnormal activation of microglia in response to inflammation could be a viable therapeutic goal for improving cerebral infarction outcomes [34]. Furthermore, researchers have discovered elevated inflammatory markers in people with thyroid nodules and other thyroid disorders like Hashimoto’s thyroiditis. Increased neutrophil-to-lymphocyte ratios (NLRs) or red blood cell distribution widths (RDWs) have been proposed by Gulali et al. as potential markers of Hashimoto’s thyroiditis [35, 36]. As an additional diagnostic technique, elevated mean platelet volume (MPV) can be utilized to distinguish between benign and malignant thyroid nodules [37].
- CONCLUSION
In conclusion, individuals with thyroid storm should undergo a thorough physical examination, and head imaging tests should be enhanced to detect cerebral infarction early. Patients with a history of hyperthyroidism should also have routine screenings for cerebrovascular illness, and prompt action to lessen the likelihood or severity of the condition should be taken into consideration. Thyroid function should be routinely checked in young stroke patients, and active treatment should start as soon as possible.
REFERENCES
- Iino T, Akatsuka M, Yamamoto S. Case report: occurrence of thyroid storm in a young patient with recurrent diabetic ketoacidosis. Front Endocrinol. 2022;13:834505.
- Akamizu T, Satoh T, Isozaki O, et al. Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys. Thyroid. 2012;22:661–79.
- Chiha M, Samarasinghe S, Kabaker AS. Thyroid storm: an updated review. J Intensive Care Med. 2015;30:131–40.
- Sheu JJ, Kang JH, Lin HC, et al. Hyperthyroidism and risk of ischemic stroke in young adults: a 5-year follow-up study. Stroke. 2010;41:961–6.
- Devinsky O, Laff R. Callosal lesions and behavior: history and modern concepts. Epilepsy Behav. 2003;4:607–17.
- Radhi MA, Natesh B, Stimpson P, et al. Thyroid storm in head and neck emergency patients. J Clin Med. 2020;9:3548.
- Banerjee A, Bala R, Aggarwal R. Atypical presentation of thyroid storm: a diagnostic dilemma. BMJ Case Rep. 2019;12:e231090.
- Gonzalez-Bossolo A, Gonzalez-Rivera A, Coste-Sibilia S. Cerebrovascular accident due to thyroid storm: should we anticoagulate? Case Rep Endocrinol. 2016;2016:5218985.
- Hampton J. Thyroid gland disorder emergencies: thyroid storm and myxedema coma. AACN Adv Crit Care. 2013;24:325–32.
- Sarah Gul Rehman & Deepak Singh. Thalassemia Consequences and Survival Rates in South Asian Kids and Adults. Dinkum Journal of Medical Innovations, 2(05):194-200.
- Rubab Rasheed & Manisha Nagpal. Psychosocial issues in Parents and Patients with Thalassemia. Dinkum Journal of Medical Innovations, 2(05):188-193.
- Dua Zahra & Parshu Ram Chaudhary. Women’s Nutritional Variability and Domestic Food Safety in Rural and Semi-Urban Communities. Dinkum Journal of Medical Innovations, 2(05):182-187.
- Pradip Rijal. Advances of NGS in Understanding of Epilepsy Genetics and Recent Discoveries of Gene in Monogenic Epilepsies. Dinkum Journal of Medical Innovations, 2(05):170-181.
- Pradip Rijal, Aatiqa Tariq & Syeda Hajra Batool. The Study of Differential Expression of Genes Controlling Reproductive Function in Immune Cells of PCOS Women. Dinkum Journal of Medical Innovations, 2(05):157-169.
- Tanabe N, Hiraoka E, Hoshino M, et al. Progressive ischemic stroke due to thyroid storm-associated cerebral venous thrombosis. Am J Case Rep. 2017;18:194–7.
- Snyder S, Joseph M. The perfect storm: a case of Ischemic stroke in the setting of thyroid storm. Cureus. 2020;12:e7992.
- Gill JH, Nam TK, Jung HK, et al. Acute cerebral infarction combined with a thyroid storm in a patient with both Moyamoya syndrome and Graves’ disease. J Cerebrovasc Endovasc Neurosurg. 2022;24:160–5.
- Czarkowski M, Hilgertner L, Powałowski T, et al. The stiffness of the common carotid artery in patients with Graves’ disease. Int Angiol. 2002;21:152–7.
- Moodley K, Botha J, Raidoo DM, et al. Immuno-localisation of anti-thyroid antibodies in adult human cerebral cortex. J Neurol Sci. 2011;302:114–7.
- Tendler BE, Shoukri K, Malchoff C, et al. Concurrence of Graves’ disease and dysplastic cerebral blood vessels of the Moyamoya variety. Thyroid. ;7:625–9.
- Zhang X, Chen Z, Shi Z, et al. Correlation between thyroid autoantibodies and intracranial arterial stenosis in stroke patients with hyperthyroidism. J Neurol Sci. 2012;318:82–4.
- Goldstein SA, Green J, Huber K, et al. Characteristics and outcomes of atrial fibrillation in patients with thyroid disease (from the ARISTOTLE trial). Am J Cardiol. 2019;124:1406–12.
- Howard-Thompson A, Luckey A, George C, et al. Graves’ disease and treatment effects on Warfarin anticoagulation. Case Rep Med. 2014;2014:292468.
- Papi G, Corsello SM, Pontecorvi A. Clinical concepts on thyroid emergencies. Front Endocrinol. 2014;5:102.
- Chaker L, Heeringa J, Dehghan A, et al. Normal thyroid function and the risk of atrial fibrillation: the Rotterdam study. J Clin Endocrinol Metab. 2015;100:3718–24.
- Kahilogullari G, Comert A, Arslan M, et al. Callosal branches of the anterior cerebral artery: an anatomical report. Clin Anat. 2008;21:383–8.
- Li S, Sun X, Bai YM, et al. Infarction of the corpus callosum: a retrospective clinical investigation. PLoS One. 2015;10:e0120409.
- Senda A, Endo A, Tachimori H, et al. Early administration of glucocorticoid for thyroid storm: analysis of a national administrative database. Crit Care. 2020;24:470.
- Carroll R, Matfin G. Endocrine and metabolic emergencies: thyroid storm. Ther Adv Endocrinol Metabol. 2010;1:139–45.
- Nakamura K, Yanaka K, Ihara S, Nose T. Multiple intracranial arterial stenoses around the circle of Willis in association with Graves’ disease: report of two cases. Neurosurgery. 2003;53:1210–14; discussion 1214-1215.
- Rathish D, Karalliyadda S. Concurrent presentation of thyroid storm and diabetic ketoacidosis: a systematic review of previously reported cases. BMC. 2019;19:49.
- Liu Z, Le Y, Chen H, et al. Role of PKM2-mediated immunometabolic reprogramming on development of cytokine storm. Front Immunol. 2021;12:748573.
- Takeda H, Yamaguchi T, Yano H, et al. Microglial metabolic disturbances and neuroinflammation in cerebral infarction. J Pharmacol Sci. 2021;145:130–9.
- Aktas G, Sit M, Dikbas O, et al. Elevated neutrophil-to-lymphocyte ratio in the diagnosis of Hashimoto’s thyroiditis. Rev Da Assoc Med Brasil. 2017;63:1065–8.
- Aktas G, Sit M, Dikbas O, et al. Could red cell distribution width be a marker in Hashimoto’s thyroiditis? Exp Clin Endocrinol Diab. 2014;122:572–4.
- Sit M, Aktas G, Ozer B, et al. Mean platelet volume: an overlooked herald of malignant thyroid nodules. Acta clinica Croatica 2019;58:417–20.
Publication History
Submitted: May 03, 2023
Accepted: May 20, 2023
Published: June 01, 2023
Identification
D-0122
Citation
John H. Marshal, Robert Downey & Olivia James (2023). Adult Participant with Corpus Callosum Infarction and Thyroid Storm Exacerbate. Dinkum Journal of Medical Innovations, 2(06):229-235.
Copyright
© 2023 DJMI. All rights reserved