

")
Publication History
Submitted: September 03, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0141
Citation
Javaria Arif, Muhammad Anwar Awan, Muhammad Suhail Sarwar, Asad Aslam Khan & Kabir Hussain (2023). Optometric Criteria of Prescription in Case of Borderline Refractive Errors. Dinkum Journal of Medical Innovations, 2(10):386-393.
Copyright
© 2023 DJMI. All rights reserved
386-393
Optometric Criteria of Prescription in Case of Borderline Refractive ErrorsOriginal Article
Javaria Arif 1*, Muhammad Anwar Awan 2, Muhammad Suhail Sarwar 3, Asad Aslam Khan 4, Kabir Hussain 5
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; javariamalikawan@gmail.com
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; Anwar_optom@gmail.com
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; drsuhail@yahoo.com
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; drasad@lhr.comsats.net.pk
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; Kabirh805@gmail.com
*Corresponding author: javariamalikawan@gmail.com
Abstract: The objective of this study is to find out the criteria for prescription in borderline refractive errors and also estimate the refractive prescription in certain conditions that involve very low degree of refractive error. A cross sectional study with the help of non-probability purposive sampling method was conducted in 66 optometrists working in government hospital, doing private job, working in optical setup, practicing in clinic or studying optometry. The study consisted of both male and female participants of age group ranges 21-48 years. A questionnaire was distributed online among the optometrists through google form. 66 optometrists were included in this study. Results were assessed online via Google form. In majority of cases optometrists prescribe new lenses i.e 97% optometrists prescribe in childhood myopia, 92.4% optometrists in latent hyperopia, 82.5% optometrists in antimetropia and 53% optometrists in residual refractive error after refractive surgery. Prescription is not given by 80.3% optometrists in allergic conjunctivitis and 77.3% optometrists in hyperglycemia. In symptomatic patients, 74.2% optometrists give full prescription in hyperopic patients, 78.8% optometrists in myopic patients and 63.6% optometrist in astigmatic patients of borderline category. It was concluded that optometrists prescribe full refractive correction in borderline cases in the presence of symptoms and slight or no prescription in the absence of symptoms. Symptoms were the most important factor which determines whether to prescribe new lenses or not.
Keywords: borderline refractive errors, refractive errors, symptoms, refractive prescription
- INTRODUCTION
Emmetropia is defined as the state of refraction wherein parallel rays of light coming from infinity are focused at retina and hence resulting in no refractive error. This is normal state of vision. In ametropia parallel rays are not focused on retina but focus either in front or behind it. In myopia rays are focused in front of retina and in hypermetropia they are focused behind it. Refractive error is considered as one of the main causes of visual impairment. It accounts for 80% of total visual impairment [1]. Accurate correction of uncorrected ametropia improves the quality of life of a person [2]. Number of people with visual impairment that includes uncorrected ametropia is 259 million and number of people having visual impairment due to uncorrected ametropia lies between 82 to 117 million [3]. Borderline refractive errors are the very small amount of errors which can or cannot be prescribed depending upon various circumstances. One of the most important decisions that optometrists have to make is to finalize the prescription of a refractive error. It is comparatively easier to prescribe for high uncorrected refractive error than for prescribing borderline cases [4]. The main purpose of optometrists is to enhance vision and eliminate the associated symptoms. In borderline refractive errors there is no significant demarcation line between prescribing or not prescribing spectacles. Presence of symptoms associated with low refractive errors is not clearly specific and defined [5]. Myopia (nearsightedness) is the error of refractive state of eye in which distant objects are not seen clearly, due to projection of light rays anterior to retina with accommodation being at rest. Prevalence of myopia is increasing day by day. Number of myopic people is estimated to be 1406 million (22.9% of world’s population) and there is prediction that by the year 2050 there will be 4758 million (49.8% of world’s population) myopic people [6]. Borderline myopia is prescription of -0.50D in the presence of symptoms and -0.75D in the absence of symptoms. It is more closely related with the normal visual development.4 in case of delayed visual impairment spectacles are the most convenient way of correction as they reduce the effects of sensory maturation [7]. Hypermetropia is the error of refraction in which parallel rays of light focus at a point posterior to retina with accommodation being at rest. Hypermetropia is most commonly presented in children, as they are hypermetropic by birth. Age of the child is inversely related with hyperopia as the child grows his refractive error reduces normally. Prevalence of hyperopia ≤ +1.25DS is 13.4% while of hyperopia ≥ +1.25DS is 34.0%. It is not understood to define a cut off\ borderline point for hypermetropia prescription due to hyperopic defocus [8]. The prescription of refractive correction starts from ≤+0.75DS in the presence of symptoms and ≥+1.00DS in the absence of symptoms [4]. Refractive error that is less than +1.00D is borderline, between +1.00D to +3.00D is mild hypermetropia and greater than +5.00D is high hypermetropia [9]. Small uncorrected hypermetropia leads to high hypermetropia with causes many visual anomalies, especially in children. It can lead to amblyopia, strabismus, anisometropia and astigmatism [10]. There is a strong association between esotropia and exotropia with childhood hyperopia [11]. Astigmatism is the type of refractive error in which parallel rays of light are not brought to a point of focus but form two focal lines that are right angle to each other. Refractive power varies in different meridia. It is one of the most common anomalies of refractive media of eye [12]. Small amount of uncorrected astigmatism can create serious disturbances in visual environment. Even <1.0D astigmatism if not corrected can influence patient’s visual acuity. Uncorrected astigmatism results in decreased distance and near vision [13]. Astigmatism is categorized as mild/low astigmatism: <-1.00D, moderate astigmatism: -1.00D to -3.00D, and high astigmatism: ≥-3.00D [14]. Overall prevalence of myopia is 27.3% with more prevalence in men and becomes stable in young and middle aged persons [15]. Presbyopia is not a refractive error but it is physiological age related decrease in amplitude of accommodation resulting in decrease of near visual acuity. With increased age the lens lose its elasticity and it becomes difficult to accommodate [16]. Uncorrected presbyopia leads to visual impairment as in 2005 people with presbyopia were 1 billion, now 1.8 billion people with presbyopia are estimated globally out of which 826 million suffer from visual impairment because they lack in adequate correction [17].
- MATERIALS AND METHODS
The study was conducted during October to December in 2020. Sixty six participants were filled questionnaire via online technique through Google form and all participants were optometrist. The questionnaire included questions related to different circumstances which acquired whether the optometrist would prescribe new lenses or not in the given scenario. The exact prescription was also determined for borderline refractive errors (myopia, hypermetropia and astigmatism) which the optometrist gives in the presence and absence of symptoms. Data is self-analyzed through Google form and different prescription criteria are assessed. Frequency and percentages are calculated accordingly. The research protocol was approved by the Ethical Review Board of College of Ophthalmology and Allied Vision Sciences. The study methods adhered to the tenets of the Declaration of Helsinki for the use of participants in bio medical research.
- RESULTS AND DISCUSSION
Sixty six optometrists were included in this study. Results were assessed online via Google form. The criteria of prescription for each condition were estimated. In majority of cases optometrists prescribe new lenses i.e., 97% optometrists prescribe in childhood myopia, 92.4% optometrists in latent hyperopia, 82.5% optometrists in anti-metropia and 53% optometrists in residual refractive error after refractive surgery. Prescription is not given by 80.3% optometrists in allergic conjunctivitis and 77.3% optometrists in hyperglycemia. In symptomatic patients, 74.2% optometrists give full prescription in hyperopic patients, 78.8% optometrists in myopic patients and 63.6% optometrist in astigmatic patients of borderline category. Graphical explanation has given below in Figures. Figure 1 showed that a patient having binocular VA 6/6 and monocular VA (right eye) 6/9 having no symptoms. More details have given below in Figure 1.
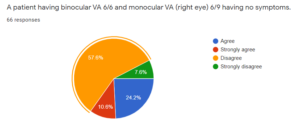
Figure 1: Frequency of having binocular VA and monocular VA in participants
Figure 2 demonstrated the refractive error in patients that demonstrated a hyperopic patient age 7-10 years old, visual acuity 6/9, and spectacles was prescribed. This graph shows that optometrists give full refractive prescription in patients representing symptoms. The Figure 3 shows that optometrists give full prescription in symptomatic patients. Figure 4 show that optometrists give full prescription in symptomatic patients. Further details have been given below.
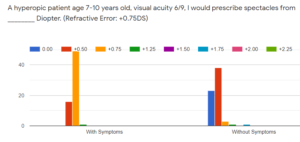
Figure 2: Refractive Error (+0.75DS) with or without symptoms
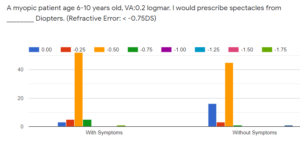
Figure 3: Refractive Error (-0.75DS) with or without symptoms
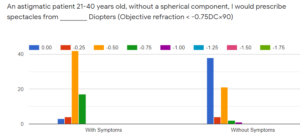
Figure 4: Refractive Error (-0.75DCx90) with or without symptoms
The main purpose of my study was to estimate the criteria of prescription of borderline refractive errors among different age groups. Prescription depends upon different factors the most important being the symptoms. The research was conducted among 66 optometrists via an online questionnaire provided with different circumstances. The optometrists were graduates, M.phil students and post graduates. Among these 66, 47% optometrists were working in government hospital, 28.8% were doing private job, 18.8% were working in clinics and remaining 5.4% were practicing in optical setups or studying optometry. 90.9% did not received any incentives on sale which means that our result is independent of the factor that corrective prescription is independent of the incentives received by optometrists. Forty seven optometrists were female and 19 were male. Majority of the optometrists [18] agreed on prescribing new lenses to patient having 6/6 partial vision with previous prescription who complained of any symptom. As symptom is the most common factor associated with refractive error and most commonly related with astigmatism.18 Visual acuity has major role in correction of refractive error as uncorrected refractive error result in reduced visual acuity and consequently decreased visual performance [19]. Most of the optometrists did not prescribe to patients having 6/6 vision in one eye and 6/9 in other eye with no symptoms. Ocular morbidity includes allergic conjunctivitis, refractive error, corneal opacity and infective conjunctivitis [20]. Fifty three optometrists did not prescribe new lenses in case of patient appreciating cylinder in allergic conjunctivitis. As in most of the cases the cylinder disappears when the allergy resolves. Thirteen optometrists prescribed in this case indicate there must be a significant change in visual acuity with prescription or patient having some degree of refractive error previously. Sometimes refractive surgery of high refractive errors results in residual refractive error. There occurs reduction in corneal thickness after refractive surgery and there are different procedures to overcome residual refractive errors that may include corneal enhancement procedures and relaxing corneal incisions. But it is risky to perform such lasers when thickness is already reduced [21]. But in case of significant residual refractive error post refractive surgery, majority of the optometrists agree on prescribing the refractive correction. People with heterophoria although have good visual functioning but it may be associated with any refractive error. It is estimated that exophoria is associated with astigmatism and esophoria has association with myopia and astigmatism [22]. Therefore most of the optometrists agree to prescribe refractive correction in case of esophoria although in the presence of normal visual functions. In patients of cataract surgery, an intraocular lens is implanted to overcome the anomalies caused by cataract. Therefore accurate biometric readings of corneal curvature and axial length are required. However sometimes there occurs some difference in calculations resulting in slight overcorrection or undercorrection of the refractive state [23]. Overcorrected intraocular lens results in myopic shift post implantation. And if there is significant refractive error it is necessary to correct it as 89.9% optometrists agree to prescribe in this case. Refractive error in case of childhood is necessary to correct. In children it is advisable to fully correct myopia to prevent its progression [24]. Therefore 64 out of 66 optometrists prescribe refractive correction in this case. Sometimes subjective refraction is verified by doing few post refraction tests, +1.00 blurr test is most common of it. If patient report differences with previous using glasses on the test then there must be some change in new prescription. Patient might be overcorrected or undercorrected. 81.8% optometrists give new prescription in this case. In some people mostly adults, cycloplegic refraction is done to estimate the otherwise latent hyperopia as it causes symptoms [25]. 61 optometrists agree to give refractive correction in latent hyperopia as it causes headache, blurring and asthenopia. Patients with antimetropia (having opposite refractive error in both eyes), are of special consideration and agree to give prescription in this case as it is mandatory to neutralize the refractive error of both eyes but it is considered to adjust the refractive power among both eyes so that it can be tolerable. Refractive errors cannot be corrected in the presence of elevated blood sugar level. There occurs instability in the refractive state in case of patients with hyperglycemia and subjective refraction is carried out when blood sugar level is normal as it improves accommodative ability [26]. Majority of the optometrists [27] do not prescribe refractive correction lenses in case of hyperglycemia. The prescription of hyperopic, myopic, astigmatic and presbyopic patients varies with the presence or absence of symptoms. In children optometrists prefer to prescribe the full correction even in the presence or absence of symptoms. In adults optometrists mostly give full prescription of borderline refractive error in the presence of symptoms, however in the absence of symptoms full or partial prescription can be given depending upon visual acuity.
- CONCLUSION AND RECOMMENDATIONS
The study concluded that prescription of refractive correction depends mainly on symptoms. Symptoms is the most important factor which determines whether to prescribe new lenses or not. However while prescribing age of the patient and visual acuity is also considered. In some circumstances falling in borderline category i.e., childhood myopia, antimetropia, residual refractive error post cataract and refractive surgery and latent hyperopia, new lenses are prescribed to a previously spectacle using person. New prescription is not given in some cases as allergic conjunctivitis, hyperglycemia and normal vision and no symptoms with previous prescription. The prescription criteria vary from case to case. In adults full prescription is given in the presence of symptoms and in the absence of symptoms the optometrists decide whether to give slight refractive correction or not depending on certain other factors like visual acuity or previous prescription. It is also considered that hypermetropia is fully corrected and myopia is slightly under corrected. There is not a definite a cutoff point of prescription but it differs according to the required condition.
Following recommendations based on this study are as follows:
- It is not necessary to give a refractive prescription in each case of borderline refractive errors.
- Prescription criteria should be majorly dependent on the symptoms as it is not constant and varies from case to case.
REFERENCES
- Error A. The prevalence of refractive errors among adults in the United States, Western Europe, and Australia. Arch Ophthalmol. 2004;122(4):495-05.
- Coleman AL, Yu F, Keeler E, Mangione CM. Treatment of uncorrected refractive error improves vision‐specific quality of life. Journal of the American Geriatrics Society. 2006;54(6):883-90.
- Dandona L, Dandona R. What is the global burden of visual impairment? BMC Med. 2006;4(1):6.
- Shneor E, Evans BJ, Fine Y, Shapira Y, Gantz L, Gordon-Shaag A. A survey of the criteria for prescribing in cases of borderline refractive errors. J Optom. 2016;9(1):22-31.
- O’leary CI, Evans BJ, Edgar DF. The effect of low refractive corrections on rate of reading. Optom Pract. 2014;15:87-100.
- Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-42.
- Smitha K, Patil V, Kamate MD, Prabhu M, Harakuni U, Rakshitha O. Impact of refractive error correction on mental and visual development in children with global developmental delay. Indian Journal of Health Sciences and Biomedical Research (KLEU). 2019;12(2):117.
- Castagno VD, Fassa AG, Vilela MaP, Meucci RD, Resende DPM. Moderate hyperopia prevalence and associated factors among elementary school students. Ciência & Saúde Coletiva. 2015;20:1449-58.
- Mezer E, Meyer E, Wygnansi-Jaffe T, Haase W, Shauly Y, Biglan AW. The long-term outcome of the refractive error in children with hypermetropia. Graefes Arch Clin Exp Ophthalmol. 2015;253(7):1013-9.
- Kulp MT, Ying G-S, Huang J, Maguire M, Quinn G, Ciner EB, et al. Associations between hyperopia and other vision and refractive error characteristics. Optometry and vision science: official publication of the American Academy of Optometry. 2014;91(4):383.
- Zhu H, Yu J-J, Yu R-B, Ding H, Bai J, Chen J, et al. Association between childhood strabismus and refractive error in Chinese preschool children. PLoS One. 2015;10(3):e0120720.
- Read SA, Vincent SJ, Collins MJ. The visual and functional impacts of astigmatism and its clinical management. Ophthalmic Physiol Opt. 2014;34(3):267-94.
- Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37(3):454-60.
- Davis AL, Harvey EM, Twelker JD, Miller JM, Leonard-Green T, Campus I. Convergence insufficiency, accommodative insufficiency, visual symptoms, and astigmatism in Tohono O’odham students. Journal of ophthalmology. 2016;2016.
- Williams KM, Verhoeven VJ, Cumberland P, Bertelsen G, Wolfram C, Buitendijk GH, et al. Prevalence of refractive error in Europe: the European eye epidemiology (E 3) consortium. Eur J Epidemiol. 2015;30(4):305-15.
- Andualem HB, Assefa NL, Weldemichael DZ, Tefera TK. Prevalence and associated factors of presbyopia among school teachers in Gondar city, Northwest Ethiopia, 2016. Clinical optometry. 2017;9:85.
- Mezer E, Meyer E, Wygnansi-Jaffe T, Haase W, Shauly Y, Biglan AW. The long-term outcome of the refractive error in children with hypermetropia. Graefes Arch Clin Exp Ophthalmol. 2015;253(7):1013-9.
- Kulp MT, Ying G-S, Huang J, Maguire M, Quinn G, Ciner EB, et al. Associations between hyperopia and other vision and refractive error characteristics. Optometry and vision science: official publication of the American Academy of Optometry. 2014;91(4):383.
- Fricke TR, Tahhan N, Resnikoff S, Papas E, Burnett A, Ho SM, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmology. 2018;125(10):1492-9.
- Dhungel D, Shrestha GS. Visual symptoms associated with refractive errors among Thangka artists of Kathmandu valley. BMC Ophthalmol. 2017;17(1):258.
- Hopkins S, Narayanasamy S, Vincent SJ, Sampson GP, Wood JM. Do reduced visual acuity and refractive error affect classroom performance? Clinical and Experimental Optometry. 2020;103(3):278-89.
- Alabi AS, Aribaba OT, Alabi AO, Ilo O, Onakoya AO, Akinsola FB. Visual impairment and ocular morbidities among schoolchildren in Southwest, Nigeria. Niger Postgrad Med J. 2018;25(3):166.
- Zhang J, He F, Liu Y, Fan X. Implantable collamer lens with a central hole for residual refractive error correction after corneal refractive surgery. Exp Ther Med. 2020;20(6):1-.
- Wajuihian SO. Prevalence of heterophoria and its association with near fusional vergence ranges and refractive errors. African Vision and Eye Health. 2018;77(1):1-9.
- Alio JL, Abdelghany AA, Fernández-Buenaga R. Management of residual refractive error after cataract surgery. Curr Opin Ophthalmol. 2014;25(4):291-7.
- Yazdani N, Sadeghi R, Ehsaei A, Taghipour A, Hasanzadeh S, Zarifmahmoudi L, et al. Under-correction or full correction of myopia? A meta-analysis. J Optom. 2021;14(1):11-9.
- Mimouni M, Zoller L, Horowitz J, Wygnanski-Jaffe T, Morad Y, Mezer E. Cycloplegic autorefraction in young adults: is it mandatory? Graefe’s Archive for Clinical and Experimental Ophthalmology. 2016;254(2):395-8.
- Abokyi S, Ayerakwah PA, Abu SL, Abu EK. Controlled blood sugar improves the eye’s accommodative ability in type-1 diabetes. Eye. 2020:1-7.
Publication History
Submitted: September 03, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0141
Citation
Javaria Arif, Muhammad Anwar Awan, Muhammad Suhail Sarwar, Asad Aslam Khan & Kabir Hussain (2023). Optometric Criteria of Prescription in Case of Borderline Refractive Errors. Dinkum Journal of Medical Innovations, 2(10):386-393.
Copyright
© 2023 DJMI. All rights reserved