

")
Publication History
Submitted: September 01, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0142
Citation
Kamal Anwar (2023). Comparison of Objective Refraction in Darkness with Cycloplegic Refraction. Dinkum Journal of Medical Innovations, 2(10):394-401.
Copyright
© 2023 DJMI. All rights reserved
394-401
Comparison of Objective Refraction in Darkness with Cycloplegic RefractionOriginal Article
Kamal Anwar1*
- College of Ophthalmology & Allied Vision Sciences (COAVS), KEMU, Lahore, Pakistan; Shahzadanwar42@gmail.com
*Corresponding author: Shahzadanwar42@gmail.com
Abstract: The goal of this research was to evaluate non-cycloplegic objective refraction using an auto-refractor in the dark and compare it to children’s subjective refraction and distant cycloplegic retinoscopy in a poorly lit room. A cross-sectional comparative research of the Punjabi population was carried out in the eye department of Mayo Hospital Lahore. 34 patients in total, ranging in age from 5 to 20, were chosen. The only eye pathology present in the patients was refractive problems. After five minutes in a dark room, auto-refraction was performed, and 20 minutes later, distant cycloplegic retinoscopy was performed using one drop of 1% cyclopentolate. Subjective refraction is the gold standard; hence a questionnaire about participants’ objective refraction in a dark room and comparison with cycloplegic refraction was conducted. SPSS 20 was used to enter and analyse the data. Mean and standard deviation for frequencies were computed. The average age in this study was 9.24, and the standard deviation was 2.00. Out of 34 patients, 16 (47.1%) were male and 18, (52.9%), were female. The outcome demonstrates that there was no discernible difference in the spherical, cylindrical, and axial values across the three techniques: subjective refraction in children, distance cycloplegic retinoscopy, and non-cycloplegic auto-refraction in the dark. All of the components’ p-values are higher than 0.05, making them all insignificant. The values of spherical, cylindrical, and axial among the three techniques of determining a patient’s refractive status are statistically negligible. Statistics demonstrate that the auto-refraction in the dark result exhibits the same values as retinoscopy and objective refraction.
Keywords: auto-refraction, retinoscopy, cycloplegic, subjective, objective, dark room
- INTRODUCTION
Refractive errors are determined by two methods, one is subjective and other is objective. For non-cooperative children and adults objective technique is used. To find out the correct refractive status subjective technique is used. Accurate correction of refractive errors is too much necessary in too young children with high hyperopia, strabismus and amblyopia [1]. Refractive power of the eye is the effect of lens and cornea to focus the Light rays. Accommodation force is the change of pitch of the curvature of lens for the change of light. Cycloplegia delays the accommodative power by inhibition the action of ciliary muscle to determine the objective refractive power in the eye.it is important to calculate full term visibility in accommodative esotropia and to prevent overcorrection in myopia. It is also useful in correcting errors in amblyopia and subjective refraction that face chaotic accommodation [2]. Retinoscopy is objective technique which is important to access the refractive errors, especially for infants and non-verbal. For an objective refraction to detect a possible failure of amblyopia this is an average value. The patient may develop amblyopia if the degree of anisometropia was important and not corrected [3]. Manual Retinoscopy is difficult and takes time even by an expert optometrist. On the other hand these things can be avoided with an auto-refractor that does not require a qualified person. Excessive accommodation effort is induced by those who use too much minus spectacles, because of this reason we do not overcorrect myopia that become troublesome [4]. Subjective refraction and cycloplegic refraction has become important measures to determine the visual status of younger patients. The cycloplegic refraction required more time to achieve complete cycloplegia. Cycloplegic Drops may cause discomfort like itching, redness, irritation. So, because of all these reasons nowadays, optometrist used auto refractor in place of cycloplegia. Auto refractor is used to access the objective refraction of children, clinical practice, visual assessment or Research purposes. Auto-refractor does not require a well train person [5]. To prevent accommodation, auto refractor has fogging technique. Some of the results made with respect to refractive errors and their ability to reconcile with one another. Children with overcorrection myopia have higher accommodation efforts that lead to progression in myopia [6]. When we compare the results of automatic refraction and cycloplegic Retinoscopy the values become spherical equivalent of the original values which are used for research purposes and individually, these spherical and cylindrical statements and their axis are modified into dioptric units that connect the sphere, cylinder and its axis [7]. Complete cycloplegia was used to access an accurate refractive error in adolescent less than 12 years of age, which is latent far sightedness, esotropia, poor fixation and children’s who are non-cooperative. For children of age 13 years refractive errors are determined by cycloplegia and self-refraction. And for this purpose, several techniques have been performed between cycloplegic Retinoscopy and non-cycloplegic refraction [8]. Refractive error is pathology worldwide that affects large number of people and it is related to many eye diseases. In adults and infants cycloplegic refraction is important tool to measure refractive errors [9]. Cycloplegic drugs have many side effects like blurred vision, irritation in eyes and redness. Therefor some people are not satisfied after cycloplegic refraction because of problems due to cycloplegic drugs. But there is evidence that myopia may be over corrected and that long term vision could be corrected if refraction was achieved without cycloplegic drugs [10]. Accommodation improves slightly or completely depending upon the age of person. With dominant hyperopia and examination related accommodation results of automatic refractometer changes. That indicates greater myopic changes. Since the housing range is age dependent, its impact on refractor results increase with age and is significant for children. It includes training for childrens [11]. Significant errors are thought to be caused by refraction without cycloplegia in children. Myopia presents a change in refractive error due to frequent accommodation response that result in insufficient correction of hyperopia and overcorrection of myopia [12]. So, estimation of refractive error with cycloplegia is the method of choice to determine refractive error with in adolescent [13]. Accommodation, mainly in children, disturbs the equivalent of sphere performing an important part in calculation of refractive error. There young children and persons with more spherical power essential to confirm by retinoscopy. To identify the refractive error, refraction with cycloplegia is important. In children the power refractor is an applied and genuine hand-held auto refractor for the verification of refractive error [14, 15]. The objectives of this study were to check the effectiveness of objective refraction using auto refractor five minutes after in dark room with distance cycloplegic retinoscopy twenty minutes after of one drop of cyclopentolate (1%) in dimly illuminated room and to find out that autorefraction is more time saving and reliable method of refraction in children than cycloplegic retinoscopy.
- MATERIALS AND METHODS
Comparative cross sectional study was conducted on patient with refractive errors from five to twenty (5-20) years of age. Patients with emmetropes, <5 & >20 years old patients, other ocular pathology, mentally retarded, and non-verbal children were excluded from study. Dependent variable was visual acuity. Independent variables were gender and age. Collage of Ophthalmology and Allied Vision Sciences were the place of study and study was conducted in 2019. Patients were visiting Eye Ward, Mayo Hospital, Lahore were included in study. Non- Probability Purposive sampling was used. Proportion of Cycloplegic refraction taken from previous study was 0.1322 and sample size was 34 patients. All the patients’ data was collected in mayo hospital eye ward. First after taking consent of all patient history was record. Then visual acuity recorded on LOGMAR chart. After sitting 5 mints in dark room auto-refraction was performed. Then cycloplegic retinosopy was performed after 20 minutes of one drop of cyclopentolate 1%. Then readings of both methods were compared with subjective refraction.
- RESULTS AND DISCUSSION
Table 1 shows us the results from two famous tests of normality (Kolmogorov-Smirnov Test and the Shapiro-Wilk test). The Shapiro-Wilk Test is more correct for low sample size like less than 50, but it can also give results of large sample size up to 2000. So there for we are using the Shapiro-Wilk test for our numerical means of determination of normality. In the above table if the P-Value of the Shapiro-Wilk Test is greater than 0.05, the data is normal. Figure 1 shows that the total number of participants is 34. In which 4 with age of 6 years, 3 with age of 7 years,7 with age of 8 years,4 with age of 9 years,5 with age of 10 years,5 with age of 11 years and 6 with age of 12 years. Table 2 shows that the total number of participant is 34 in which 16 are male and 18 are females. Table 3 shows that out of 34 participants 20 have history of glasses and 14 have no history of glasses. Table 4 shows that right eye sphere with auto-refractor SD is 3.039, right eye sphere with retinoscopy SD is 2.948 and right eye sphere with subjective SD is 2.817.
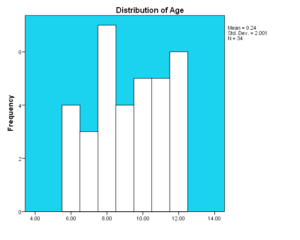
Figure 1: Age distribution of age in patients (N = 34)
Table 1: Normality test results of study variables (N= 34)
| Variables | Kolmogorov-Smirnova | Shapiro-Wilk | ||||
| Statistic | Df. | P-Value | Statistic | Df. | P-Value | |
| Right eye sphere in dark | .231 | 15 | .030 | .855 | 15 | .020 |
| Left eye sphere in dark | .243 | 15 | .018 | .881 | 15 | .049 |
| Right eye cylinder in dark | .139 | 15 | .200* | .941 | 15 | .401 |
| Left eye cylinder in dark | .130 | 15 | .200* | .949 | 15 | .515 |
| Right eye axis in dark | .264 | 15 | .006 | .826 | 15 | .008 |
| Left eye axis in dark | .199 | 15 | .114 | .825 | 15 | .008 |
| Right eye sphere with Retino | .278 | 15 | .003 | .783 | 15 | .002 |
| Left eye sphere with Retino | .290 | 15 | .001 | .794 | 15 | .003 |
| Right eye cylinder with Retino | .116 | 15 | .200* | .939 | 15 | .369 |
| Left eye cylinder with Retino | .113 | 15 | .200* | .948 | 15 | .495 |
| Right eye axis with Retino | .254 | 15 | .010 | .832 | 15 | .010 |
| Left eye axis with Retino | .246 | 15 | .015 | .779 | 15 | .002 |
| Right eye sphere with sub ref | .280 | 15 | .002 | .825 | 15 | .008 |
| Left eye sphere with sub ref | .280 | 15 | .002 | .789 | 15 | .003 |
| Right eye cylinder with sub ref. | .114 | 15 | .200* | .959 | 15 | .667 |
| Left eye cylinder with sub ref. | .107 | 15 | .200* | .948 | 15 | .493 |
| Right eye axis with sub ref. | .291 | 15 | .001 | .810 | 15 | .005 |
| Left eye axis with sub ref. | .257 | 15 | .009 | .840 | 15 | .013 |
| *. This is a lower bound of the true significance. | ||||||
| a. Lilliefors Significance Correction | ||||||
Table 2: Gender distributions of patients
| Variables | Frequency | Percent |
| Male | 16 | 47.1 |
| Female | 18 | 52.9 |
| Total | 34 | 100.0 |
Table 3: Analysis of history of glasses usage
| History of glasses usage | Frequency | Percent |
| Yes | 20 | 58.8 |
| No | 14 | 41.2 |
| Total | 34 | 100.0 |
Table 4: Descriptive statistics of variables (Right eye sphere)
| Category | N | Minimum | Maximum | Mean | S. Deviation | |
| Auto in Dark | Right sphere | 30 | -7 | 6 | .07 | 3.039 |
| Retinoscopy | Right sphere | 31 | -7 | 6 | .10 | 2.948 |
| Subjective | Right sphere | 29 | -6 | 5 | .17 | 2.817 |
Table 5 shows that left eye sphere with auto-refractor SD is 2.840, left eye sphere with retinoscopy SD is 3.254 and left eye sphere with subjective SD is 2.869.
Table 5: Descriptive statistics of variables (Left eye sphere)
| Category | N | Minimum | Maximum | Mean | S. Deviation | |
| Auto in Dark | Left sphere | 33 | -4 | 8 | .58 | 3.039 |
| Retinoscopy | Left sphere | 32 | -9 | 6 | .16 | 2.948 |
| Subjective | Left sphere | 30 | -8 | 5 | .10 | 2.817 |
Table 6 shows that right eye cylinder with auto-refractor SD is 2.093, right eye cylinder with retinoscopy SD is 2.225 and right eye cylinder with subjective SD is 2.225. Table 7 shows that left eye cylinder with auto-refractor SD is 1.960, left eye cylinder with retinoscopy SD is 2.068 and left eye cylinder with subjective SD is 1.956.
Table 6: Descriptive statistics of variables (Right cylinder)
| Variables
|
N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | |
| Lower Bound | Upper Bound | |||||||
| Auto in Dark | 33 | -1.15 | 2.093 | .364 | -1.89 | -.41 | -6 | 3 |
| Retinoscopy | 27 | -.89 | 2.225 | .428 | -1.77 | -.01 | -5 | 3 |
| Subjective | 23 | -.96 | 2.225 | .464 | -1.92 | .01 | -5 | 3 |
| Total | 83 | -1.01 | 2.150 | .236 | -1.48 | -.54 | -6 | 3 |
Table 7: Descriptive statistics of variables (Left cylinder)
| Variables
|
N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | |
| Lower Bound | Upper Bound | |||||||
| Auto in Dark | 33 | -.97 | 1.960 | .341 | -1.66 | -.27 | -5 | 3 |
| Retinoscopy | 28 | -.86 | 2.068 | .391 | -1.66 | -.06 | -4 | 3 |
| Subjective | 25 | -.92 | 1.956 | .391 | -1.73 | -.11 | -4 | 2 |
| Total | 86 | -.92 | 1.972 | .213 | -1.34 | -.50 | -5 | 3 |
A study was performed on automatic refraction dark and cycloplegic retinoscopy after a drop of cyclopentolate. In 34 participants 34.53% of the population was female and 47% of male. This sample size was concluded with a specially designed formula [16]. When the auto-refraction and retinoscopy measurements were compared, the values were changed to SE for study and, individually, these spherical and cylindrical declarations and their axis are modified at a single point to obtain the eccentricity for each dimension in dioptric units which simultaneously connect the spherical, cylindrical and its axis of dimensions. Studies have shown that clinically significant impairment was greater in children under the age of 6. Although retraction is done due to the low level of collaboration and the high level of accommodation in children, these alterations do occur. In adult children, this can be improved, used to detect and correct refractive errors. In young people with mixed astigmatism, this should be checked with an automatic hand refractor and retinoscopy in the study, the spherical values showed variations between the three procedures [17]. Some previous studies show that retinoscopy after cycloplegia and autorefraction after cycloplegia could be useful screening tools for refractive error in offspring, but could not find any study indicating the consistency of autorefraction under cyclopentolate. In this study, autorefraction with cycloplegia provides good agreement with cycloplegic retinoscopy to find the type of refractive error. In our study, automatic refraction in the dark and cycloplegic refraction showed no significant difference in the three spherical, cylindrical and axial values. First, an automatic refraction is performed, then a retinoscopy then a subjective refraction. All three methods work on the same day [18]. Smith’s study shows us that the standard deviation of uncertainty in the calculation of refractive error is close to 0.3. Most of the uncertainty difference, which gives 95% autonomy, would be 0.6 diopters in the refractive error calculations. Refractive errors calculated with a difference of 0.25 diopters, appropriated a variation of more than 0.50 of the diopters of the spherical and cylindrical values as a clinically important change. Certain studies show that the automatic refractor produces a myopic refraction compared to subjective refraction. In contradiction, there is no significant association with cycloplegia. In previous studies, we obtained that the amounts of spherical equivalent and spherical power without cycloplegia by plusoptix A04 were compared with cycloplegic refraction. However, the application of the cycloplegic drug indicates an extended spherical equivalent, a cylindrical power and a spherical power calculated by plusoptix A09. In addition, the cylindrical power calculated by plusoptix A09 with and without cyclopentolate is greater [19]. A recent study that included screening children with refractive error with and without cycloplegia using retinomax K-plus 2 and plusopti X S08 and comparing it with cycloplegic retinoscopy, revealed that sensitivity advanced with cycloplegia because the accommodative element was excluded among the most young boys. Our study was conducted in children and compared objective refraction in the dark with cycloplegic and subjective refraction. The results do not show significant differences between the three procedures in terms of spherical, cylinder and axis values [20].
- CONCLUSION AND RECOMMENDATIONS
In all the three methods of finding refractive status of patients the values of spherical, cylindrical and axis are statistically insignificant. The result of auto-refraction in darkness statistically shows same values to Retinoscopy and objective refraction. It is more satisfactory for parents as they have fears about side effects of cycloplegic drops.
REFERENCES
- Hashemi H, Khabazkhoob M, Asharlous A, Soroush S, Yekta A, Dadbin N, et al. Cycloplegic autorefraction versus subjective refraction: the Tehran Eye Study. Br J Ophthalmol. 2016;100(8):1122-7.
- Arici C, TÜRK A, Keskin S, Ceylan OM, Mutlu FM, Altinsoy HIJTJoMS. Effect of cycloplegia on refractive errors measured with three different refractometers in school-age children. Turk J Med Sci. 2012;42(4):657-65.
- Ozdemir O, Tunay ZÖ, Petriçli IS, Acar DE, Erol MKJIjoo. Comparison of non-cycloplegic photorefraction, cycloplegic photorefraction and cycloplegic retinoscopy in children. Int J Ophthalmol. 2015;8(1):128.
- Morgan IG, Iribarren R, Fotouhi A, Grzybowski AJAo. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 2015;93(6):581-5.
- Hu YY, Wu JF, Lu TL, Wu H, Sun W, Wang XR, et al. Effect of cycloplegia on the refractive status of children: the Shandong children eye study. PLoS One. 2015;10(2):e0117482.
- French AN, Morgan IG, Burlutsky G, Mitchell P, Rose KAJO. Prevalence and 5-to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology. 2013;120(7):1482-91.
- Vasudevan B, Ciuffreda KJ, Meehan K, Grk D, Cox MJC, Optometry E. Comparison of objective refraction in darkness to cycloplegic refraction: a pilot study. Clin Exp Optom. 2016;99(2):168-72.
- Choong Y-F, Chen A-H, Goh P-PJAjoo. A comparison of autorefraction and subjective refraction with and without cycloplegia in primary school children. Am J Ophthalmol. 2006;142(1):68-74. e1.
- Kinge B, Midelfart A, Jacobsen GJBjoo. Clinical evaluation of the Allergan Humphrey 500 autorefractor and the Nidek AR-1000 autorefractor. Br J Ophthalmol. 1996;80(1):35-9.
- Guha S, Shah S, Shah K, Hurakadli P, Majee D, Gandhi SJC, et al. A comparison of cycloplegic autorefraction and retinoscopy in Indian children. Clin Exp Optom. 2017;100(1):73-8.
- Ayse YK, Onder U, Suheyla KJCJoO. Accuracy of Plusoptix SO4 in children and teens. Can J Ophthalmol. 2011;46(2):153-7.
- Singman E, Matta N, Tian J, Brubaker A, Silbert DJS. A comparison of the PlusoptiX S04 and A09 photoscreeners. Strabismus. 2013;21(2):85-7.
- Payerols A, Eliaou C, Trezeguet V, Villain M, Daien VJBo. Accuracy of PlusOptix A09 distance refraction in pediatric myopia and hyperopia. BMC Ophthalmol. 2016;16(1):72.
- Smith GJC, Optometry E. Refraction and visual acuity measurements: what are their measurement uncertainties? Clin Exp Optom. 2006;89(2):66-72.
- Manny RE, Chandler DL, Scheiman MM, Gwiazda JE, Cotter SA, Everett DF, et al. Accommodative lag by autorefraction and two dynamic retinoscopy methods. Optom Vis Sci. 2009;86(3):233-43.
- Bailey MD, Twa MD, Mitchell GL, Dhaliwal DK, Jones LA, McMahon TTJJoC, et al. Repeatability of autorefraction and axial length measurements after laser in situ keratomileusis. J Cataract Refract Surg. 2005;31(5):1025-34.
- Kulp MT, Ying G-s, Huang J, Maguire M, Quinn G, Ciner EB, et al. Accuracy of noncycloplegic retinoscopy, retinomax autorefractor, and SureSight vision screener for detecting significant refractive errors. Invest Ophthalmol Vis Sci. 2014;55(3):1378-85.
- Iuorno JD, Grant WD, Noël L-PJJoAAfPO, Strabismus. Clinical comparison of the Welch Allyn SureSight handheld autorefractor versus cycloplegic autorefraction and retinoscopic refraction. J AAPOS. 2004;8(2):123-7.
- Silbert J, Matta N, Tian J, Singman E, Silbert DIJJoAAfPO, Strabismus. Pupil size and anisocoria in children measured by the plusoptiX photoscreener. J AAPOS. 2013;17(6):609-11.
- Paff T, Oudesluys-Murphy AM, Wolterbeek R, Swart-van den Berg M, de Nie JM, Tijssen E, et al. Screening for refractive errors in children: the plusoptiX S08 and the Retinomax K-plus2 performed by a lay screener compared to cycloplegic retinoscopy. J AAPOS. 2010;14(6):478-83.
Publication History
Submitted: September 01, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0142
Citation
Kamal Anwar (2023). Comparison of Objective Refraction in Darkness with Cycloplegic Refraction. Dinkum Journal of Medical Innovations, 2(10):394-401.
Copyright
© 2023 DJMI. All rights reserved