

")
Publication History
Submitted: September 06, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0145
Citation
Prabin Acharya & Prachi Bhattarai (2023). Perinatal Mortality Rate in South-Asian Countries: A Systematic Review. Dinkum Journal of Medical Innovations, 2(10):418-425.
Copyright
© 2023 DJMI. All rights reserved
418-425
Perinatal Mortality Rate in South-Asian Countries: A Systematic ReviewReview Article
Prabin Acharya 1*, Prachi Bhattarai2
- Nepal Medical College Teaching Hospital, Nepal; prabinacharya098@gmail.com
- Nepal Medical College Teaching Hospital, Nepal; bhattarai_prachi546@gmail.com
* Correspondence: prabinacharya098@gmail.com
Abstract: The average number of premature and late neonatal deaths per 1000 live births is known as the neonatal mortality rate. A fetus that dies at or after 28 weeks of gestation or weighs 1000 grams or more is said to have experienced late fetal death . Pakistan continues to have a 37/1000 stillbirth rate and an early neonatal mortality rate (ENMR) of 43/1000, which suggests that there is a deficiency in identifying the obstacles to providing the best prenatal care as well as insufficient quality treatment during or shortly after delivery. In order to assist policy makers in identifying areas that require improvement and in providing suggestions for effectively reducing the perinatal mortality rate, the purpose of this systematic review is to ascertain the prevalence of perinatal mortality rate in Pakistan and other South Asian nations. To adopt novel health care initiatives and monitor success at the national and sub-national levels, timely and dependable statistics on maternal and neonatal mortality are necessary.
Keywords: perinatal, mortality, South Asian Countries
- INTRODUCTION
The average number of premature and late neonatal deaths per 1000 live births is known as the neonatal mortality rate. A fetus that dies at or after 28 weeks of gestation or weighs 1000 grams or more is said to have experienced late fetal death [1, 2]. Although the globe has achieved major strides in the field of health, which has increased newborn and child survival, there is still a great deal of work to be done to address the extremely high rates of neonatal and perinatal mortality in some parts of the world. “To ensure healthy lives and promote well-being for all at all ages” is the mission statement of Sustainable Development Goal no. 3, or SDG-3, as it is officially known. By 2030, it seeks to put an end to the avoidable deaths of infants and young children worldwide. An estimated 1.8 million newborns perished in 2019 and a further 2 million stillbirths were reported [3]. 40% of newborn deaths worldwide are caused by maternal mortality, but 70% of infant deaths are caused by perinatal mortality [4]. A nation’s socioeconomic standing and the quality of its healthcare system are both reflected in the PNMR and NMR [5]. The high rates of stillbirths and early infant deaths in many nations pose a significant obstacle to accomplishing the Sustainable Development Goals 3 (SDG 3) set forth by the World Health Organization [6]. The global perinatal mortality rate (PMNR) was reported to be 43/1000 live births (7.5 perinatal deaths annually) in 2015 [7], a significant decrease from the 1990 perinatal mortality rate of 91/1000 live births. South Asia and sub-Saharan Africa are home to low- and middle-income nations, accounting for 98% of all recorded perinatal fatalities globally. This explains why, despite considerable improvements in the newborn mortality rate (NMR) and under-5 mortality rate (U5MR), there has been little to no improvement in the global PNMR [6]. Perinatal mortality rate (PNMR) estimates for Asia range from 50/1000 to 65/1000 in south-central Asia [8]. Regional differences can exist, though; Bangladesh and Nepal, for instance, have far lower rates of foetal death. Nonetheless, there has been no progress in reducing neonatal mortality, according to the Pakistan Demographic and Health Survey (PDHS), despite a gradual improvement in children health indicators like Under Five Mortality and Infant Mortality. Instead, Pakistan’s rate of neonatal deaths has gone up since 1990 [9–10]. Pakistan continues to have a 37/1000 stillbirth rate and an early neonatal mortality rate (ENMR) of 43/1000, which suggests that there is a deficiency in identifying the obstacles to providing the best prenatal care as well as insufficient quality treatment during or shortly after delivery. In order to assist policy makers in identifying areas that require improvement and in providing suggestions for effectively reducing the perinatal mortality rate, the purpose of this systematic review is to ascertain the prevalence of perinatal mortality rate in Pakistan and other South Asian nations. To adopt novel health care initiatives and monitor success at the national and sub-national levels, timely and dependable statistics on maternal and neonatal mortality are necessary.
- MATERIALS AND METHODS
The systematic review is reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
2.1 Eligibility criteria
Inclusion criteria:
- If the study is a survey, cross-sectional, or cohort study, it is included.
- It provides any unique information on the rates of stillbirth, early neonatal mortality, and neonatal mortality, among other perinatal outcomes.
- It is released between 2018 and 2023; • It is carried out in South Asian nations.
Exclusion criteria:
- If the study is a review based on secondary data, RCTs, or systematic reviews, it is not included.
- The entire text is not available.
- There isn’t an English version available.
- It provides information on non-Asian nations.
- Its foundation is a particular minor population.
2.2 Search strategy and study selection
Three internet databases—Google Scholar, Pub Med, and Cochrane—were searched for every study released between January 2018 and March 2023. Duplicate entries were eliminated using EndNote Reference Software X7. The last duplicates were then manually eliminated. The articles were then manually filtered using Microsoft Excel based on the title and abstract. Two reviewers separately completed the full text screening, and any disagreements were discussed with a third reviewer to resolve them. The aforementioned exclusion criteria were used to eliminate the research, and full-text screening was used to pick the papers that met the inclusion criteria.
2.3 Data Extraction
Data were extracted using excel spread sheet. The following data were extracted; authors and year of publication, region, study design, study setting, sample size and magnitude and trend of perinatal mortality (including stillbirth and early neonatal mortality).
2.4 Data Analysis
Authors and the year of publication, location, study design, study setting, sample size, stillbirth rate, early neonatal death result, and perinatal mortality outcome were all recorded on a data extraction sheet. The study looked at several definitions of mortality. A total of fifteen studies [11-16, 18-21,23-27], five studies [11,15,18,19,23], and nine studies [11,15,17-19,22-25] reported on the rate of stillbirths, 7-day neonatal mortality (ENMR), and perinatal mortality, respectively. Using Microsoft Excel, the descriptive analysis was carried out. The studies were divided into groups based on the perinatal outcomes (SBR, ENMR, and PMR) that were examined in this systematic review as well as the countries (India, Pakistan, Bangladesh, and Nepal).
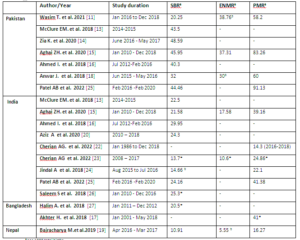
Table 1: Mortality Rates in some south Asian countries
- ANALYSIS AND RESULTS
Through the literature research, 850 articles were identified.48 duplicates were removed before screening. After removing duplicates articles were screened on the basis of titles and abstracts. Of these, 760 were excluded during the abstract screening stage. Thus, a total of 19 articles were included after meeting the inclusion criterion for this review [Figure1].
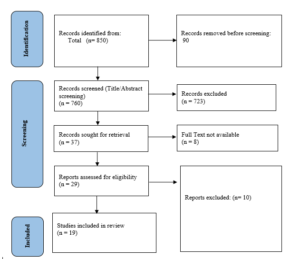
Figure 1: PRISMA Flow Chart
According to the study by Saleem S et al. 2018[26], conducted between 2010 and 2016 the SBR was estimated to be 56.9/1000 births in Pakistan. Another study by Patel AB et al. 2022, [25] conducted between 2016 and 2020 SBR was 44.6 per 1000 births in Pakistan which shows a slight decline as compared to the previous data but it is still quite high. A hospital based study conducted in Islamabad Aziz A et al. 2020 between 2012 and 2016 shows SBR of 11.9 per 1000 births which is significantly lower which may be due to small sample size of 109 pregnant women[20]. In Bangladesh, a study [27] conducted between 2011 and 2012 the SBR was recorded as 19.6 in 2011 and 21.4 in 2012 per 1000 births which shows a slight rise in subsequent year but the rates are low as compared to India and Pakistan. One study by Aghai ZH.et al.[15], which was conducted in Pakistan between 2010 and 2018, estimated the ENMR in Pakistan to be 37.31 per 1000 live births which is comparable to the rates found in another study by Wasim T. et al. [11] conducted in a public hospital of Lahore, Pakistan which calculated ENMR to be 38.76 per 1000 live births. Another study conducted by Cherian AG et al. [23] reported the ENMR in India to be 10.6 per 1000 live births. In contrast, the study conducted in Nepal by Bajracharya M. et al. [19] between 2016 and 2017, the ENMR in Nepal was estimated to be 5.55 per 1000 live births which is lower than both Pakistan and India. These studies show that Pakistan has a relatively higher ENMR compared to India and Nepal, while Nepal has the lowest ENMR among the studied South Asian countries. Two studies Aghai ZH.et al.[15] and Patel AB et al.[25] that were undertaken in Pakistan between 2010 and 2020,stated that the PMR was 83.26 and 91.13 per 1000 total births respectively. A study conducted in a public hospital in Lahore estimated PMR to be 58.2/1000 total births with early neonatal deaths constituting a larger share than stillbirths[11] While the data collected in Indian site revealed PMR to be 39.16 per 1000 total births[15].] According to a study conducted by Akhter H. et al.[17] carried out in Bangladesh between 2001 and 2018, the PMR was 41/1000, which is lower than that of Pakistan and India. In contrast, the study carried out in Nepal (2016–2017) Bajracharya M. et al revealed that the PMR was 16.27/1000 total births, the lowest among the studies South Asian countries[19].This was a study with a small sample size of 1275 which pointed out the avoidable factors responsible for perinatal deaths. The studies which reported at least two of the three perinatal outcomes were included in the data for column chart. The studies were grouped according to the country so that the different perinatal outcomes can be compared among these four countries. (Figure 2).
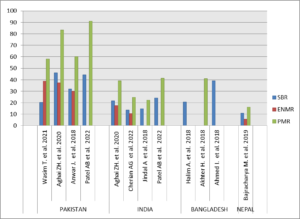
Figure 2: Perinatal outcomes for some South Asian countries
The incidence of perinatal deaths in several south Asian nations was the main focus of this systematic review. Perinatal deaths include stillbirths and early neonatal deaths. Among the studies that presented data on Pakistan. The PMR for Pakistan was reported in total 4 studies.[11][15][18][25] The PMR was found to be relatively lower in two studies by Wasim et al. [11] and Anwar J. et al. [18] that reported it to be 58.2 and 60 respectively. While a study by Aghai et al. [15] which is a population based study with a sample size of 91355 reported PMR to be 83.26/1000 total births. The perinatal mortality rates in Pakistan were previously reported as 107.8/1000 and 97.2/1000[28, 29] which shows the improvement in mortality rates in later years but the country still has long way to go before achieving global target. A study which collected data from both the Pakistani and Indian sites showed that for India and Pakistan the cumulative stillbirth rate was 25.3 and 56.9 per 1000 births respectively. Another study that involved both Pakistan and India showed that the PMR was 83.26 which are a lot higher than the rates found in India that is 39.16.This comparison was also true for SBR and ENMR. The SBR were found to be 45.95 and 21.58 while ENMR were 37.31 and 17.58 for Pakistan and India respectively [15]. A study in Bangladesh showed that in urban areas, the perinatal death rate has decreased from 55.6 in 2000 to 35 in 2014 i.e. by almost half. Rural areas had a higher perinatal death rate than urban areas, which decreased from 57.7 per 1,000 live births in 2000 to 47 in 2014 which showed that rural areas are improving at an almost nonexistent rate [17]. As all the countries discussed in this systematic review i.e. Bangladesh, India, Pakistan and Nepal are LMICs so when compared with the other LMICs such as countries in Sub Saharan Africa, their trends and improvements can be better understood. A systematic review that estimated perinatal death rates across many different countries shows that the pooled estimated PMR across 4 sub-regions of Sub-Saharan Africa (SSA) are 34.5, 35.7, 30.3 and 30.7 per 1000 births which gives the cumulative PMR of 34.7 across Sub-Saharan Africa. The highest reported PMR across Sub-Saharan Africa is for Lesotho-which is also a LMIC- that is 49.62/1000.
- CONCLUSION
Perinatal mortality rate is the highest in Pakistan among other South Asian countries including India, Bangladesh and Nepal. The PMR in Pakistan is almost double than the global average of 43/1000 live births [7]. It signifies that perinatal mortality rate has not improved significantly in the last few years in South-Asian countries especially Pakistan who is making very little progress. This systematic review emphasizes the importance of better surveillance of perinatal and neonatal mortalities and need of policies to reduce these mortality rates.
REFRENCES
- Aziz A, Saleem S, Nolen TL, Pradhan NA, McClure EM, Jessani S, Garces AL, Hibberd PL, Moore JL, Goudar SS, Dhaded SM. Why are the Pakistani maternal, fetal and newborn outcomes so poor compared to other low and middle-income countries?. Reproductive Health. 2020 Dec;17:1-2.
- Aziz S, Naseer M, Akhter S, Shahid R. Frequency of Stillbirths at MCH Centre FGPC Islamabad. Journal of the Society of Obstetricians and Gynecologists of Pakistan. 2018 Apr 17;8(1):9-14.
- Cherian AG, Paul JS, Abraham VJ, Mohan VR, Prasad JH, George K. Changes in birth weights and perinatal mortality rate in a rural block in South India over 30 years. Current Medical Issues. 2022 Oct 1;20(4):225.
- Cherian AG, Tryphena C, George K, Abraham VJ, Mohan VR, Prasad JH. Perinatal mortality and its causes in a rural block in Tamil Nadu, Southern India: A community-based non-concurrent cohort study. Indian Journal of Community Medicine: Official Publication of Indian Association of Preventive & Social Medicine. 2022 Jan;47(1):12.
- Jindal A, Thakur R, Minhas S. Causes of stillbirth according to different gestational ages. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2018 Mar 1;7(3):1029-35.
- Patel AB, Bann CM, Kolhe CS, Lokangaka A, Tshefu A, Bauserman M, Figueroa L, Krebs NF, Esamai F, Bucher S, Saleem S. The Global Network Socioeconomic Status Index as a predictor of stillbirths, perinatal mortality, and neonatal mortality in rural communities in low and lower middle income country sites of the Global Network for Women’s and Children’s Health Research. Plos one. 2022 Aug 16;17(8):e0272712.
- Saleem S, McClure EM, Goudar SS, Patel A, Esamai F, Garces A, et al. A prospective study of maternal, fetal and neonatal deaths in low- and middle-income countries. Bulletin of the World Health Organization. 2014;92(8):605–12.
- De Bernis L, Kinney MV, Stones W, ten Hoope-Bender P, Vivio D, Leisher SH, Bhutta ZA, Gülmezoglu M, Mathai M, Belizán JM, Franco L. Stillbirths: ending preventable deaths by 2030. The lancet. 2016 Feb 13;387(10019):703-16.
- Arach AA, Tumwine JK, Nakasujja N, Ndeezi G, Kiguli J, Mukunya D, et al. Perinatal death in Northern Uganda: Incidence and risk factors in a community-based prospective cohort study. Global Health Action. 2021;14(1).
- Hossain MB, Kanti Mistry S, Mohsin M, Rahaman Khan MH. Trends and determinants of perinatal mortality in Bangladesh. PLOS ONE. 2019;14(8).
- Yu VYH. Global, regional and national perinatal and neonatal mortality. Journal of Perinatal Medicine. 2003;31(5).
- Ahmed J, Alam A, Raynes-Greenow C. Maternal empowerment and healthcare access determines stillbirths and early neonatal mortality in Pakistan: Analysis of Demographic and Health Survey 2012-13. Journal of Global Health Reports. 2018;2.
- Rahemi MH, Masih M. A descriptive study of under-five mortality. Journal of Pharmaceutical Research International. 2021;:86–97.
- Ghimire PR, Agho KE, Renzaho AM, Nisha MK, Dibley M, Raynes-Greenow C. Factors associated with perinatal mortality in Nepal: Evidence from Nepal Demographic and health survey 2001–2016. BMC Pregnancy and Childbirth. 2019;19(1).
- Ahmed M, Won Y. Cross-national systematic review of neonatal mortality and postnatal newborn care: Special focus on Pakistan. International Journal of Environmental Research and Public Health. 2017;14(12):1442.
- Cross-national research to help countries prepare for an aging population. Revista Panamericana de Salud Pública. 2001;10(4).
- Wasim T, Bushra N, Iqbal HI, Mumtaz A, Khan KS. Maternal condition as an underlying cause of perinatal mortality: Prospective cohort study. Journal of Obstetrics and Gynecology Research. 2021 Feb;47(2):544-50.
- Altijani N, Carson C, Choudhury SS, Rani A, Sarma UC, Knight M, Nair M. Stillbirth among women in nine states in India: rate and risk factors in study of 886,505 women from the annual health survey. BMJ open. 2018 Nov 1;8(11):e022583.
- McClure EM, Garces A, Saleem S, Moore JL, Bose CL, Esamai F, Goudar SS, Chomba E, Mwenechanya M, Pasha O, Tshefu A. Global Network for Women’s and Children’s Health Research: probable causes of stillbirth in low‐and middle‐income countries using a prospectively defined classification system. BJOG: An International Journal of Obstetrics & Gynecology. 2018 Jan;125(2):131-8.
- Zia K, Zahid N, Saad M, Shahzad R, Manzoor U, Shahzad U. An Analytical Study of Intrauterine Fetal Demise with Risk Factors and Prevention Strategies in a tertiary care hospital of Lahore. Pakistan Journal of Medical and Health Sciences. 2020;14(2):282-5.
- Aghai ZH, Goudar SS, Patel A, Saleem S, Dhaded SM, Kavi A, Lalakia P, Naqvi F, Hibberd PL, McClure EM, Nolen TL. Gender variations in neonatal and early infant mortality in India and Pakistan: a secondary analysis from the Global Network Maternal Newborn Health Registry. Reproductive health. 2020 Dec;17:1-1.
- Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, Begum N, Bhandari N, Bhatia K, Bhutta ZA, Biemba G. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. The Lancet Global Health. 2018 Dec 1;6(12):e1297-308.
- Akhter H, Jahan KM, Numan MH. Understanding the neonatal health situation of Bangladesh in relation to other South Asian countries. Asian Research Journal of Arts & Social Sciences. 2018;7(4):1–15.
- Anwar J, Torvaldsen S, Sheikh M, Taylor R. Under-estimation of maternal and perinatal mortality revealed by an enhanced surveillance system: enumerating all births and deaths in Pakistan. BMC Public Health. 2018 Dec;18:1-4.
- Bajracharya M, Sherpa AT, Dhakal A, Bhandari S, Tuladhar H, Maharjan M. Perinatal Mortality review in a tertiary care hospital: Way Forward to Address SDG Health Goal 3. Medical Journal of Shree Birendra Hospital. 2019 Feb 26;18(1):69-74.
Publication History
Submitted: September 06, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0145
Citation
Prabin Acharya & Prachi Bhattarai (2023). Perinatal Mortality Rate in South-Asian Countries: A Systematic Review. Dinkum Journal of Medical Innovations, 2(10):418-425.
Copyright
© 2023 DJMI. All rights reserved