

")
Publication History
Submitted: September 04, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0147
Citation
Mahrukh Asghar, Ashfaq Ahmad, Waqar Afzal, Umber Nawaz, Aqeel Saeed & Iqra Rasheed (2023). Effectiveness of Routine Physical Therapy with and Without Core Stability Exercises in Patients with Rotator Cuff Tendinopathy. Dinkum Journal of Medical Innovations, 2(10):443-451.
Copyright
© 2023 DJMI. All rights reserved
443-451
Effectiveness of Routine Physical Therapy with and Without Core Stability Exercises in Patients with Rotator Cuff TendinopathyOriginal Article
Mahrukh Asghar 1*, Ashfaq Ahmad 2, Waqar Afzal 3, Umber Nawaz 4, Aqeel Saeed 5, Iqra Rasheed 6
1, 2, 3, 4, 5 University Institute of Physical Therapy, University of Lahore, Pakistan; mahrukhasghar@yahoo.com, ashfaq.ahmad@uipt.uol.edu.pk, waqarafzal621@gmail.com, umber.nawaz@uipt.uol.edu.pk , aqeelsaeed5@gmail.com
6 Development and Behavioral Pediatrics, University of Child Health Sciences, Pakistan; iqra111rasheed@gmail.com
* Correspondence: mahrukhasghar@yahoo.com
Abstract: Core has greatest impact on our body stability especially of extremities. The goal of this study is to determine the effectiveness of routine physical therapy with and without core stability exercises in patients with rotator cuff tendinopathy. The randomized control trial, which was conducted at physical therapy department of Wapda Teaching Hospital Complex Lahore included rotator cuff tendinopathy patients of both gender having age from 26 to 50 years and patients with fracture, tumor, any deformity, cervical radiculopathy and surgery of shoulder and spine were excluded. . Data was collected through Comparative Pain scale and Upper Extremity Functional Index. Data was entered and analyzed by using SPSS. 32 (or 50%) of the 64 participants were experimental and controls. Comparison between groups regarding pain indicates significant difference that is P-value < 0.000 and comparison regarding Upper Extremity Functional Index (UEFI) indicates no significant difference at UEFI 1 means that P > 0.159 and at UEFI 2 and UEFI 3 the results were significant means P < 0.05. Hence, this study concluded that core stability exercises have significant effect on functional movement and injury prevention of upper extremity.
Keywords: rotator cuff tendinopathy, core stability exercise, upper extremity
- INTRODUCTION
Shoulder musculoskeletal disorders are relatively frequent because of its three dimensional mobility. That’s why shoulder pain and discomfort is habitual complaining especially in Rotator Cuff (RC) tendinopathy subjects. While rotator cuff tendinopathy is one of most generally complaining condition, its ratio of incident is 2.9-5.5% [1]. The term rotator cuff tendinopathy is extensive in character means various conditions come under its heading. So the term Rotator Cuff Tendinopathy is categorize as: “tendonitis, tendinosis, paratendinosis or partial tears of the Rotator Cuff tendons” while the condition “sub acromial impingement syndrome, sub deltoid bursitis adhesive capsulitis and full thickness tears” were excluded [2-4]. Rotator cuff tendinopathy is characterized as, when any tendon of rotator cuff in shoulder get inflamed and injured due to repetitive use especially in overhead activities or steady wear and tear. It is classified according to its anatomical and clinical presentation. Classification is based upon the depth of tear, ranges from partial to full thickness tear. At first the normal tendon, second partial thickness tear, third solitary tendon full thickness tear (0-2.5cm) and lastly multi tendon full thickness tear ( > 2.5cm) [2]. Most common tendon in rotator cuff muscles that usually pull apart is supraspinatous tendon. Acute or partial tear may results after traumatic incident leads to shoulder pain and inappropriate functioning. While chronic or full thickness tear elicits inconsistent pain and infirmity [3]. The significant feature of rotator cuff tendinopathy is describe as pain and fragility that usually arises with shoulder movements especially in external rotation and elevation, as a consequence of extreme loading on the rotator cuff tissues. Etiology of rotator cuff tendinopathy is multifactorial and can be assigning as extrinsic factors, intrinsic factors, as well as environmental factors [5]. For complex and skilled overhead functions, core provide a foundation upon which muscles of upper extremity depends. The core is describes as trunk or more particularly as lumbopelvic segment of the body that provide a stabilize base for limbs movement. This stabilization system is formed by the summation of three distinct components that are Passive Component including ligament and facet articulation between adjacent vertebras, active component that is composed of global and local muscles and neural component that consists of muscle spindle, spinal ligaments and Golgi tendon organ. The involvement of joints, muscles and nerves facilitates posture adjustment and load management to shows the concept of core stability is dynamic in nature [6]. The most effective position in which core functioning optimum is standing, as spine is upheld in vertical and straight position which allows the extremity to accomplish its function freely by placing stress on core musculature [7]. Inadequate core strength and endurance results in increased risk of injury and anatomical deformation. So, core stability is an essential component of biomechanical proficiency by minimizing loads on peripheral joints and enables an individual to produce maximum force [8]. Optimum force production, transmission and regulation required an integrated system of kinetic chain that helps in sequential muscle activation and coordination results in maximum functional output. Any deficit in anatomical and functional kinetic chain system results in impairment of limb movement [9, 10]. Aforementioned analysis in the field of core rehab and conditioning programs were directed only with the point of view to improve athletes muscle strength, endurance and consume energy properly with in sports. While the aim of this investigation is to explore the core stability effects in rotator cuff tendinopathy patients and upper extremity functional status. Core stability work out is essential in upper and lower extremity rehabilitation as it provides ground for functional movements and activities. Apart from routine physical therapy of rotator cuff tendinopathy treatments, an advance technique of core stabilization is introduced to manage upper extremity issues. By integrating advance strategies along with routine treatment physiotherapist and trainers can attain best output from patients.
- LITERATURE REVIEW
In 2019 a study was conducted by Teresa Paolucci et al., to reveal the association between core stability and shoulder injury in overhead athletes during rehabilitation. The strength and credibility of trunk muscles indicate the core stability of any athlete. The study aimed to highlight the effectiveness of core stability in preventing injuries during overhead sports activity. The outcomes after conducting a literature review showing a positive effect of core stability on the shoulder, but further researches have to perform for clear evidence. In 2018 Ali Cadgas Yorukoglu et al. conducted a study to explain the relationship between core stability and rotator cuff injury. The study included 58 patients after rotator cuff (RC) surgery within 2 to 15 days of surgical repair, while 114 healthy subjects of the same age were added to the control group. In the RC repair group, a standardized rehabilitation program was followed without core stability exercises. Core endurance was accessed in the repair group after one year by using different tests. The results show that core endurance was significantly better in the control group than in the repair group. The study illustrates that; stronger core stabilization had a direct effect on loads of vertebral column. The core muscles facilitate by reducing the load on the spine and amplifies peripheral joint strength and endurance: this permits effective energy transfer to distal compartments. The core is the potent area of the trunk, so in shoulder rehabilitation, the core exercise program facilitates by fulfilling the gap between preliminary and later functional training. So coordination of the neuromuscular system along with core stabilization has beneficial results on rotator cuff rehabilitation [11]. A comparative study in young females was conducted in 2018 to observe the influence of core stabilization exercises in the shoulder reintegration regime. Seventy-five healthy females have enrolled in the study, from which 42 females add to the study group, 33 add to the control group. One of the foremost goals of shoulder rehabilitation is shoulder muscle strength. The point of focus of the study was to explore the outcome of core stabilization exercise and investigation of the core muscle-activated posture on shoulder maximal voluntary isometric contraction (MVIC) strength as a result of instant reaction. Home base core stabilization exercise program assigned to the study group for the six-week interval. The results; have been measured by the dynamometer. The results were statistically significant means core stabilization exercises have a positive impact on shoulder maximal voluntary isometric contraction (MVIC) strength. Kinetic chain exercises of the upper extremity were incorporated in shoulder rehabilitation for the last few years. The subsequent transmission of forces and motion while performing a dynamic task can only be possible through mechanical connections of body segment and this phenomenon is known as the kinetic chain [12-13]. Optimum function level in kinetic chain system is essential for the functional movement of extremity, and this can only be achieved if core functions exceptionally [14-15]. The outcome supported the application of core stabilization exercises during the early phase of rehabilitation when shoulder muscle strengthening exercises were painful and causing discomfort [16].
- MATERIALS AND METHODS
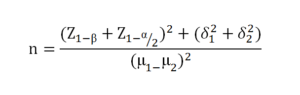
A Randomized Control Trial (RCT) was directed at physical therapy section of Wapda Teaching Hospital Complex Lahore. The study was completed in 9 months after approval. An inclusion and exclusion criterion was mentioned above in abstract [17]. Comparative Pain scale was use to access level of pain and Upper Extremity Functional Index (UEFI) was used to determine functional status [12]. The estimated value of sample size was 64 while expecting 95% confidence level with accuracy 0.05. The sample size calculation was performed by using Open Epi Calculator [13].
Patients who satisfy the above stated criteria were enrolled. Sampling method was non probability convenient sampling hence 32 patients registered in each group. Management regime for group A was patient education, therapeutic ultrasound (at frequency of 1.1 MHz and intensity 1.5 W/cm2) [14] along with shoulder and core exercises. Shoulder exercises include ROM, pendulum exercises, stretching and strengthening exercises of shoulder and cervical [15]. A core stability exercise includes curl-up, supine bridge, bird dog exercise, cat and camel and crunches [16]. The treatment plan was scheduled as; 5-6 minutes were reserved for ultrasound (at frequency of 1.1 MHz and intensity 1.5 W/cm2) [17], 35 minutes for shoulder and neck exercises and former 15 minutes for core stability exercises. The frequency of treatment session was 3 times / week with 3 sets and 10-15 repetitions with 10 seconds hold [14 17]. While group B underwent only routine physical therapy treatment. This consist of patient education, therapeutic ultrasound (at frequency of 1.1 MHz and intensity 1.5 W/cm2) along with shoulder exercises. Shoulder exercises comprised of ROM, pendulum exercises, stretching and strengthening exercises of shoulder and cervical exercises [15]. The Frequency of core stability was 3 times / week with 3 sets and 10-15 repetitions with 10 seconds hold [14 17]. The overall number of sittings were 12 and complete treatment length was extended to 4 weeks. Details from participants were collected after taking written informed consent. After enrolment in group’s baseline information was gathered (represented as Pain1 and Upper Extremity Functional Index 1 or UEFI 1) while patient reinvestigation and data collection was done after 6th session means after 2 weeks (represented as Pain 2 and Upper Extremity Functional Index 2 or UEFI 2) and then at 12th session means after 4 weeks (represented as Pain 3 and Upper Extremity Functional Index 3 or UEFI 3).
Statistical Analysis
Numerical data was documented and examined by using SPSS V23. 0. Descriptive statistics was used for evaluation of standard characteristics such as age, gender, height and weight. After checking normality, the independent sample t test was used to compare the mean variance of score among the two groups. Repeated Measure-ANOVA was used for repeated measure analysis of variance within the group. P-value of less than 0.05 was considered as significant.
- RESULTS
In this study 64 participants were taking part (n = 32 in each group). Out of these 64 patients, in group A (n = 32) the number of female and male patients were 18 (56.3%) and 14 (43.8%) respectively while in group B (n = 32) the number of female and male patients were 17 (53.1%) and 15 (46.9%) respectively. Therefore sum of female respondents were greater as compared to male respondents. The mean and SD age of volunteers in group-A was 37.09 ± 7.38 years and in group-B was 36.96 ± 6.56 years. While mean and SD of BMI in group-A was 22.34 + 3.34 and group-B was 23.42 + 3.51 respectively (Table 1).
Table 1: Descriptive Statistics of Demographic Data
|
|
Gender
|
Age |
BMI |
|
|
Group A |
Mean |
1.56
|
37.09 |
22.34 |
|
SD |
0.50 |
7.38 |
3.34 |
|
|
Group B
|
Mean |
1.53
|
36.96
|
23.42
|
|
SD |
0.50 |
6.56 |
3.51 |
|
Demographic data of Group-A and Group-B
Descriptive statistics shows mean and standard deviation of pain in Group-A at Pain 1, Pain 2 and Pain 3 were 35.78 ± 7.87, 19.68 ± 6.56, 1.09 ± 1.55 and Group-B 40.37 ±5.67, 25.68 ± 4.02, 11.93 ± 1.66 respectively and mean and standard deviation of upper extremity functional index in group-A and group-B after first assessment at UEFI 1 was 24.09 ± 10.71 and 20.81 ± 7.41 respectively. While after completion of six sessions the mean Score for UEFI in Group-A and Group-B at UEFI 2 was 53.34 ± 6.21, 44.84 ± 5.36 respectively. And UEFI 3 which represents the mean and S.D after 12th session in Group-A and in Group-B was 78.37 ± 2.16, 62.93 ± 4.98 respectively. (Table. No 2)
Table 2: Descriptive Table of Mean and S.D in Groups related to UEFI
| Group | Pain 1 | Pain 2 | Pain 3 | UEFI 1 | UEFI 2 | UEFI 3 | |
|
GroupA |
Mean |
6.40 ± |
3.37 ± |
0.53 ± |
24.09 |
53.34 |
78.37 |
|
Std. Deviation |
1.49 |
1.58 |
0.84 |
10.71 |
6.21 |
2.16 |
|
|
GroupB |
Mean |
6.87 ± |
4.71 ± |
3.25 ± |
20.81 |
44.84 |
62.93 |
|
Std. Deviation |
1.21 |
1.27 |
0.98 |
7.41 |
5.36 |
4.98 |
|
Mean pain score in Group-A and in Group-B at Pain 1 score at baseline (Before treatment), Pain 2 Score at 6th session and Pain 3 Score at 12th session.
UEFI 1= UEFI score at baseline (Before treatment), UEFI 2 = Score at 6th session and UEFI 3 = Score at 12th session.
Comparison between groups regarding pain indicates no significant difference at Pain 1 means P-value = 0.174, Pain 2 and at Pain 3 levels P-value is P < 0.000 means there was significant difference between two groups. While comparison between groups regarding UEFI was shown no statistical difference at UEFI 1 level means P-value > 0.159. While at the level of UEFI 2 and UEFI 3 the results showed significant difference at these two levels means P-value < 0.05 (Table 3).
Table 3: Independent T test to compare the results of UEFI within groups
| Pain and UEFI | T | Sig. (2-tailed) | Mean Difference
|
95% Confidence Interval of the Difference | ||
| Lower | Upper | |||||
|
Pain 1 |
-1.375 | 0.174 | -0.468 | -1.150 | 0.212 | |
| Pain 2 | -3.741 | 0.000 | -1.343 | -2.061 | -0.625 | |
| Pain3 | -11.878 | 0.000 | -2.718 | -3.176 | -2.261 | |
| UEFI 1 | 1.42 | 0.159 | 3.281 | -1.323 | 7.885 | |
|
UEFI 2 |
5.85 | 0.000 | 8.500 | 5.598 | 11.401 | |
|
UEFI 3 |
16.07 | 0.000 | 15.437 | 13.517 | 17.357 | |
Pain indicates no significant difference at Pain1 (P value 0.174) while at Pain 2 and Pain 3 shows significant difference (P value 0.000).
Upper Extremity Functional Index (UEFI) indicates no significant difference at UEFI 1 (P value 0.159) while at UEFI 2 and UEFI 3 shows significant difference (P value 0.000).
- DISCUSSION
This research was conducted on two groups of Rotator Cuff patients having random allocation of 32 subjects in each group. The Upper Extremity Functional Index was used to collect data and the outcome of this comparison between groups regarding functional status indicates no significant difference at UEFI 1 means that P > 0.156 and at UEFI 2 and UEFI 3 the results were significant means P < 0.05. A study supervised by Tugba Kocahan and Bihter Akinoglu to find out the core stamina and isokinetic muscle power association in elite athletes, as both of these constituents were responsible for athletes potential, achievement and probability of having any injury. The objective of the study was to discover the relation among elite athletes regarding shoulder isokinetic muscle strength andbiathlon, having age of 18.13 ± 2.9 years were included in this study. ISOMED 2000 apparatus was used to determine the shoulder external-internal rotation muscles isokinetic strength while Mcgill Core Endurance Tests were executed to observe core endurance of volunteers. Results showed the link between all endurance tests, peak torque/body weight and shoulder internal and external rotation except extension strength test means p-value < 0.05. Hence results indicates that all muscles are interlinked and athletes must analyzed and trained as a whole [18]. Current study included 64 participants, having age of 37.17 ± 6.85 years. While upper extremity functional index was used to examine the functional status and outcomes of our study also shows the positive relation among core stability training and upper extremity rehabilitation that is P-value < 0.000. A study was conducted by Teresa Paolucci et al., to reveal the association between core stability and shoulder injury in overhead athletes during rehabilitation. The strength and credibility of trunk muscles indicates the core stability of any athlete. The aim of the study was to highlight the effectiveness of core stability in preventing injuries during overhead sports activity. After considering the inclusion criteria only 13 articles were included in this study. The outcomes after conducting literature review was showing positive effect of core stability on shoulder but further researches were conducting for clear evidence [19 20]. The conclusion of our study also indicates that core stability was an effective treatment method for rotator cuff (RC) tendinopathy patients to relief their discomfort and accomplishment of functional status. Hence there was significant difference among the groups means P-value <0.000. In another study directed by Marisa Pontillo et al., in which they worked on comparison of core stability and balance in athletic population that either suffered from shoulder injury or not. The aim was to develop a comparison among traumatic and non-traumatic shoulder injuries in athletes regarding core stability and balance. Eighty athletes were enrolled in both groups with same age, gender, BMI and sports activity. Athletes accomplished different tests for core stability and balance including double leg lower test, flexor and extensor endurance test, Y-balance test and single leg stance test. Logistic regression was used to access data. The results were surprising as there was no significant difference between the two groups, the value were ϰ2 = 4.4, df = 4, p = 0.36. Although core stability is the major component that assimilated in injured athlete training program, hence no variation were found in static and dynamic balance among the two groups [21]. Present study shows association between core stability and rotator cuff tendinopathy, as it showed level of significance among these variables (p < 0.05). According to a study conducted by Justin Shinkle et al., to detect core strength influence on the power of extremities. The objective of his study was to formulate a functional yield test to examine the role of core musculature and its impression on athletic outdoor activity and also to determine that how effectively force transmitted from lower to upper extremity by core. 25 National Collegiate Athletic Association Division I football players were enrolled. To investigate the dynamic core muscle durability influence on extremities different activities were designed. The results were statistically significant (p < 0.05) means core have an adequate effect on extremity power [22]. Conclusion of our study also shows the significant correlation between core exercises and upper extremity mobility and functional status. It was concluded that implementation of core training in shoulder rehabilitation program had noteworthy effects. As core stability was supposed to have an essential role with athletic performance and injury over a decade [8, 23]. So it was postulated that any deprivation in core stability amplifies the possibility of upper extremity impairment and performance of athletes were adversely influenced.
- CONCLUSIONS
This study concluded that core stability exercises have considerable effect on rotator Cuff tendinopathy patients as it showed significant improvement in pain and functional status as compared to routine physical therapy treatment.
REFERENCES
- Littlewood C, May S, Walters S. Epidemiology of rotator cuff tendinopathy: a systematic review. Shoulder & Elbow. 2013;5(4):256-65.
- Hinsley H, Nicholls A, Daines M, Wallace G, Arden N, Carr A. Classification of rotator cuff tendinopathy using high definition ultrasound. Muscles, ligaments and tendons journal. 2014;4(3):391.
- Carr A, Harvie P. Rotator cuff tendinopathy. Tendon Injuries: Springer; 2005. p. 101-18.
- Abat F, Alfredson H, Cucchiarini M, Madry H, Marmotti A, Mouton C, et al. Current trends in tendinopathy: consensus of the ESSKA basic science committee. Part I: biology, biomechanics, anatomy and an exercise-based approach. Journal of experimental orthopaedics. 2017;4(1):18.
- Lewis J, McCreesh K, Roy J-S, Ginn K. Rotator cuff tendinopathy: navigating the diagnosis-management conundrum. journal of orthopaedic & sports physical therapy. 2015;45(11):923-37.
- Willardson JM. Core stability training: applications to sports conditioning programs. The Journal of Strength & Conditioning Research. 2007;21(3):979-85.
- Hasegawa I. Using the overhead squat for core development. NSCA Perform Train J. 2004;3(6):19-21.
- Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports medicine. 2006;36(3):189-98.
- Pontillo M. Relationship between core stability and shoulder injuries in athletes: Drexel University; 2016.
- Okada T, Huxel KC, Nesser TW. Relationship between core stability, functional movement, and performance. The Journal of Strength & Conditioning Research. 2011;25(1):252-61.
- de Fontenay BP, Mercier C, Bouyer L, Savoie A, Roy J-S. Upper limb active joint repositioning during a multijoint task in participants with and without rotator cuff tendinopathy and effect of a rehabilitation program. Journal of Hand Therapy. 2020;33(1):73-9.
- Gabel CP, Michener LA, Burkett B, Neller A. The Upper Limb Functional Index: development and determination of reliability, validity, and responsiveness. Journal of Hand Therapy. 2006;19(3):328-49.
- Hazar Z, Ulug N, Yuksel I. Is there a relation between shoulder dysfunction and core instability? Orthopaedic journal of sports medicine. 2014;2(11_suppl3):2325967114S00173.
- Analan PD, Leblebici B, Adam M. Effects of therapeutic ultrasound and exercise on pain, function, and isokinetic shoulder rotator strength of patients with rotator cuff disease. Journal of physical therapy science. 2015;27(10):3113-7.
- Kisner C, Colby LA, Borstad J. Therapeutic exercise: Foundations and techniques: Fa Davis; 2017.
- Miyake Y, Kobayashi R, Kelepecz D, Nakajima M. Core exercises elevate trunk stability to facilitate skilled motor behavior of the upper extremities. Journal of bodywork and movement therapies. 2013;17(2):259-65.
- Littlewood C, Ashton J, Chance-Larsen K, May S, Sturrock B. Exercise for rotator cuff tendinopathy: a systematic review. Physiotherapy. 2012;98(2):101-9.
- Kocahan T, Akınoğlu B. Determination of the relationship between core endurance and isokinetic muscle strength of elite athletes. Journal of exercise rehabilitation. 2018;14(3):413.
- Paolucci T, Coraci D, Saggini R, Pezzi L, Priori F. Core Stability and Shoulder Injury in Overhead Athletes: A Mini Review. Diagn Ther Complement Tradit Med. 2019;1:03-5.
- Paolucci T, Coraci D, Priori F, Conte V, Santilli V. Core Stability and Shoulder Injury in Overhead Athletes: A Mini Review. Diagn Ther Complement Tradit Med 2019 (1): 03-05. Correspondence should be addressed to Teresa Paolucci, Italy E-mail: teresapaolucci@ hotmail. com DOI: 10.33513. DTCT/1901-02, 2019.
- Pontillo M, Silfies S, Butowicz CM, Thigpen C, Sennett B, Ebaugh D. Comparison of core stability and balance in athletes with and without shoulder injuries. International Journal of Sports Physical Therapy. 2018;13(6):1015.
- Shinkle J, Nesser TW, Demchak TJ, McMannus DM. Effect of core strength on the measure of power in the extremities. The Journal of Strength & Conditioning Research. 2012;26(2):373-80.
- Ben Kibler W. The role of the scapula in athletic shoulder function. The American journal of sports medicine. 1998;26(2):325-37.
Publication History
Submitted: September 04, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0147
Citation
Mahrukh Asghar, Ashfaq Ahmad, Waqar Afzal, Umber Nawaz, Aqeel Saeed & Iqra Rasheed (2023). Effectiveness of Routine Physical Therapy with and Without Core Stability Exercises in Patients with Rotator Cuff Tendinopathy. Dinkum Journal of Medical Innovations, 2(10):443-451.
Copyright
© 2023 DJMI. All rights reserved