

")
Publication History
Submitted: September 02, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0148
Citation
Jamal Ahammed, Ferdous Alam, Al Rezowan Shoron, Md. Amir Hamja Niloy, Sumitro Das, Biswajit Kumar Utpal & Sumon Chandraw Roy (2023). A Review on Flavonoids in Neuropathic Pain. Dinkum Journal of Medical Innovations, 2(10):452-465.
Copyright
© 2023 DJMI. All rights reserved
452-465
A Review on Flavonoids in Neuropathic PainReview Article
Jamal Ahammed 1*, Ferdous Alam 2, Al Rezowan Shoron 3, Md. Amir Hamja Niloy 4, Sumitro Das 5, Biswajit Kumar Utpal 6, Sumon Chandraw Roy 7
- Daffodil International University, Bangladesh; jamal29-155@diu.edu.bd
- Daffodil International University, Bangladesh; ferdus.ph@gmail.com
- Daffodil International University, Bangladesh; Shoronmirdha5@gmail.com
- Daffodil International University, Bangladesh; mdamirhamjaniloy184@gmail.com
- University of Asia Pacific, Bangladesh; sumitro990@gmail.com
- Daffodil International University, Bangladesh; utpalpharmacy17@gmail.com
- Medical Information officer Jenphar Bangladesh; sumonr843@gmail.com
* Correspondence: jamal29-155@diu.edu.bd
Abstract: Chronic pain continues to be a major strain on the US healthcare system. Neuropathic pain, a frequent kind of chronic pain, is extremely difficult to cure even after extensive research efforts. There are numerous potentially dangerous side effects and a limited efficacy with current pharmaceutical regimens. This review provides a comprehensive preclinical study of the literature on the use of flavonoids in the treatment of neuropathic pain. Flavonoids are naturally occurring compounds that are present in many food sources, including plants, and they have the potential to be effective in the treatment of neuropathic pain. Numerous research utilising animal models have demonstrated this benefit, including the reversal of hyperalgesia and allodynia. Flavonoids have also exhibited an anti-inflammatory impact relevant to neuropathic pain, as evidenced by the decrease in many pro-inflammatory mediators such as TNF-, NF-B, IL-1, and IL-6. Although they haven’t been tried on humans yet, flavonoids appear promising in preclinical models for treating neuropathic pain.
Keywords: neuropathic, pharmacological, anti-inflammatory, drug, flavonoids
- INTRODUCTION
An unpleasant emotion is often brought on by powerful or potentially harmful stimuli. According to the International Association for the Study of Pain, pain is “an unpleasant sensory and emotional experience associated with, or resembling that associated with actual or potential tissue damage”[1]. Pain is considered to be a symptom of an underlying condition when performing a medical diagnosis. Pain causes an individual to remove themselves from potentially harmful situations, to protect a damaged body part while it heals, and to steer clear of similar experiences in the future [2]. The majority of pain disappears once the noxious stimulus is removed and the body has healed, but it is possible for the pain to persist despite the removal of the stimulus and apparent healing of the body. [Case in Sometimes a person may experience pain even when there is no obvious cause, injury, or illness present [3]. Pain is the most common reason people seek medical attention in most developed countries [4-5]. It is a major symptom of many medical conditions, and it can interfere with a person’s quality of life and general functioning [6]. Simple pain medications are effective in 20% to 70% of cases [7]. Psychological factors such as social support, cognitive behavioral therapy, excitement, or distraction can affect the intensity or unpleasantness of pain [8-9]. It has been argued that allowing those who are suffering from terminal illnesses to end their lives via euthanasia or physician-assisted suicide is the compassionate thing to do since they are in agony [10].

Figure 1 Graphical explanation of pain
In the English language, the word “penalty” first emerged in 1297. The word “punishment” (also known as “torment, hardship, and suffering” in Late Latin) comes from the Latin word “poena,” which in turn came from the Greek word “v” (point), which generally meant “price paid, penalty, and punishment” [12–13]. The Old French word “ensure” is the source of this word. NeuPSIG recently changed the definition of neuropathic pain from “pain initiated or caused by a primary lesion or dysfunction of the nervous system,” as provided by the International Association for the Study of Pain (IASP), to “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system.” Thus, in the updated description, the primary cause of this pain has been identified as a sickness that affects the “somatosensory system” instead of the “nervous system,” providing additional insight into its genesis. Under normal circumstances, the somatosensory system transmits dangerous information to the central nervous system. Consequently, somatosensory system damage can cause pain at the location of discomfort in addition to blocking nerve cell innervation, whether or not a sensory hypersensitive episode occurs. Positive and negative sensory issues can arise from injury to the somatosensory system. Positive sensory symptoms are caused by nerve cell regeneration and disinhibition as a result of decreased sensory input, whereas negative sensory symptoms are caused by a partial or complete loss of input to the neurological system. Positive symptoms may manifest spontaneously or in response to a stimuli. Paraesthesias (tingling or ant-crawling sensations over the skin), spontaneous continuous or shooting pain (stimulus-independent), and electric shock-like sensations are not stimulus-evoked positive symptoms of neuropathy, although hyperalgesia and allodynic pain are Pallyhypoesthesia (reduced sensations to vibration), thermohypoesthesia (abridged impression to cold/warm), and hypoalgesia (abridged impression to noxious stimuli) are negative signs and symptoms of neuropathic pain. Painful sensory neuropathy may respond well to opioids, tricyclic antidepressants, gabapentin, pregabalin, phenytoin, lamotrigine, dextromethorphan, tramadol, and mexiletine, as per several controlled trials. These treatments, sedation being the most common, only lower pain by 30 to 50 percent and are sometimes only temporary. They do not fully eradicate pain.
- LITERATURE REVIEW
Rheumatoid arthritis, peripheral neuropathy, cancer, and idiopathic pain may endure for years. Chronic pain lasts longer than acute pain. Acute and chronic pain has traditionally been distinguished by an arbitrary period of time between onset and remission, with 3 months and six months being the most popular markers [14, 15]. Some theories and researchers have put the shift from acute to chronic pain at 12 months [16]. Others call “acute” pain less than 30 days, “chronic” pain more than six months, and “subacute” pain one to six months. “Pain that lingers beyond the usual time of recovery” is a common definition of chronic pain [17]. A typically painless stimulation causes allodynia. Stimuli classify it as dynamic mechanical, punctate, or static [18-19]. Phantom pain is perceived in an amputated or non-signaled bodily component. Phantom pain affects 82% of upper-limb amputees and 54% of lower-limb amputees. One research indicated that 72% of patients experienced phantom limb discomfort eight days after amputation and 67% six months afterward [20-22]. Some amputees have daily agony, while others have it less frequently. Shooting, crushing, scorching, or cramping are common descriptions. Long-term pain may cause sensitive areas of the intact body, causing the phantom limb to hurt when touched. Phantom limb pain may precede urination or feces.
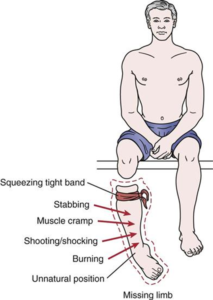
Figure 2: Phantom limb pain
Local anesthetic injections into the nerves or sensitive areas of the stump may relieve pain for days, weeks, or even permanently, despite the drug wearing off in hours. Small injections of hypertonic saline into the soft tissue between vertebrae produce local pain that radiates into the phantom limb for ten minutes and may relieve phantom pain for hours, weeks, or even longer [23]. Some individuals get relief with vigorous stump vibration, electrical stimulation, or spinal cord electrodes. Mirror box treatment may reduce phantom limb discomfort by creating the appearance of movement and touch.[24] Paraplegia, the loss of feeling and voluntary motor control following substantial spinal cord injury, may be accompanied by girdle pain at the spinal cord damage, visceral discomfort from a filled bladder or bowel, or phantom body pain in regions of total sensory loss in five to ten percent of paraplegics. Phantom bodily pain starts as scorching or tingling and progresses to crushing, pinching, fire flowing down the legs, or a knife twisting in the skin. Onset may be instantaneous or years after the crippling injury. Surgery seldom lasts. Breakthrough pain is abrupt, untreated pain. Cancer patients frequently have background pain that is well-controlled by drugs but sometimes has extreme pain that “breaks through” the medication. Breakthrough cancer pain varies by individual and cause. Breakthrough pain may need fentanyl and other medications [25-26]. Pain helps prevent and detect harm. A soldier on the battlefield may not experience pain after a catastrophic amputation or other serious injuries for hours because of episodic analgesia [27-28]. Morphine injection or psychosurgery may elicit extreme pain without unpleasantness in certain people, despite the IASP definition of pain requiring unpleasantness. [29] Patients report feeling pain but not being troubled by it [30]. Rarely do those born indifferent to pain have normal nerves, find pain unpleasant, and repeat the pain stimulation. Nervous system problems may potentially cause pain insensitivity. Undiscovered injuries may cause tissue damage and infection in these people. Due to diminished sensitivity, diabetics’ foot sores heal poorly. Congenital insensitivity to pain is rare and caused by a neural system defect. This disorder repeatedly damages tongues, eyes, joints, skin, and muscles. Some die young; others have shorter lives. Five genetic sensory and autonomic neuropathies cause most congenital insensitivity to pain (which includes familial dysautonomia and congenital insensitivity to pain with anhidrosis). These diseases include autonomic nervous system anomalies and diminished pain sensitivity [31]. Mutations in the SCN9A gene, which encodes a sodium channel (Nav1.7) that conducts pain nerve inputs, have been related to a rare disease of isolated congenital insensitivity to pain. Neuropathy may refer to either a disruption in nerve function or a change in the nerves themselves. Diabetes is responsible for around thirty percent of instances of neuropathy. Sometimes it might be difficult to determine what exactly is causing the neuropathic pain. This particular form of suffering may be attributed to any one of several hundred different illnesses. Pain that is caused by injury or illness that affects the somatosensory system is referred to as neuropathic pain [32-33]. It is possible that it will have both continuous and episodic (paroxysmal) features. The latter feels like being stabbed or getting an electric shock. The feeling of “pins and needles,” itching, burning, numbness, and general itchiness are all often experienced symptoms. As much as 7%-8% of the population in Europe is affected, [34] and the severity of the condition may vary from person to person [35-36]. Pain that is classified as neuropathic may be caused by dysfunctions in either the central nervous system or the peripheral nervous system (brain and spinal cord). Accordingly, neuropathic pain may be classified as either peripheral neuropathic pain, central neuropathic pain, or mixed neuropathic pain (which includes both peripheral and central components). Pain due to neuropathy may occur by itself or in conjunction with other types of pain. The primary goals of medical therapies are to ascertain the root cause of the problem and to alleviate suffering. In certain forms of neuropathy, the sensation of pain might eventually be replaced by numbness. It is possible to trace the origins of pain treatment all the way back to ancient times. Galen also theorized that nerve tissue served as a conduit for the transmission of pain signals from the body to the brain through an unseen psychic pneuma [37]. Medieval medical experts, including Rhazes, Haly Abbas, and Avicenna, put forward the concept that pain originates from the nerve itself and that there should not be any stimulating disease in other organs in order for there to be a pain. They referred to this unique kind of pain as “Vaja al as” (which translates to “pain originating in the nerves”), characterized its numbness, tingling, and needling nature, and spoke about its genesis as well as the distinguishing qualities [38]. John Fothergill is the one who first characterized the condition known as neuralgia (1712-1780). Gordon used the term “neuropathy” for the very first time in 1924 in a medical publication that was titled “Clinical Lecture on Lead Neuropathy,” which was sent to medical professionals at that time [39]. Multiple sclerosis, spinal cord damage, and spinal neuropathic pain are all examples of central neuropathic pain [40]. Diabetes, metabolic diseases, herpes zoster infection, HIV-related neuropathies, nutritional deficiencies, toxins, distant manifestations of malignancies, immunologically mediated illnesses, and physical damage to a nerve trunk are among the major causes of peripheral neuropathies [41-42]. As a direct outcome of cancer on peripheral nerves (such as compression by a tumor) or as a side effect of chemotherapy (chemotherapy-induced peripheral neuropathy), neuropathic pain is frequent in cancer patients [43]. Sharp, stabbing pain and the presence of specific traits are used in the diagnosis of many pain syndromes. Neuropathic pain also has a tendency to impact certain dermatomes, and its distribution may be restricted. Clinicians treating patients with neuropathic pain seek damage to the nervous system or an initiating reason that is consistent with the onset of neuropathic pain. In circumstances when the identification of the underlying lesion leaves the patient in pain for an extended length of time, the patient’s reaction to therapy may be utilized as a proxy to determine the existence of an underlying characteristic or cause. The main manifestation of a tumor or multiple sclerosis is two examples of dangerous underlying illnesses that may be diagnosed with MRI’s aid [44]. Numerous studies have employed quantitative sensory testing (QST), a method of an in-depth examination of the somatosensory system, to detect neuropathic pain and dissect its components. Some experts have hypothesized that QST might one day be used to help diagnose neuropathic pain and, more specifically, help distinguish between the many subtypes of neuropathic pain. It is possible for neuropathic pain to coexist with other forms of pain. Different types of analgesics are needed; therefore, learning how to categorize neuropathic pain is crucial. Skin biopsies are the gold standard for determining whether or not small fiber neuropathy is the underlying cause of neuropathic pain. A screening approach to reduce the number of patients who need a skin biopsy is electrochemical skin conductance evaluation, which is an accurate, objective procedure [45-46].

Figure 3: Quantitative sensory testing (QST)
Weakness, numbness, and pain often manifest in the hands and feet as symptoms of peripheral neuropathy, which results from damage to the nerves outside of the brain and spinal cord. Digestion, urine, and circulation are just a few of the numerous bodily processes that may be impacted [47].
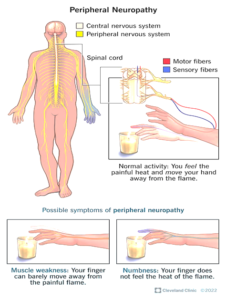
Figure 4: Peripheral neuropathy
Since autonomic neuropathy (AN or AAN) affects the non-voluntary, non-sensory nerve system (i.e., the autonomic nervous system), it mostly affects the internal organs, such as the bladder muscles, cardiovascular system, digestive system, and genital organs. These nerves function automatically, without the person’s knowledge or understanding. The thorax, abdomen, and pelvis are among the regions outside of the spinal cord where large clusters of autonomic nerve fibres gather. But they are connected to the brain through the spinal cord. Autonomic neuropathy can develop in people with type 1 and type 2 diabetes mellitus who have had the condition for a very long time. It is common to observe autonomic neuropathy in conjunction with other neuropathy kinds, like sensory neuropathy. This isn’t always the case, though. Autonomic neuropathy is merely one cause of autonomic nerve system malfunction (dysautonomia), which can be brought on by a variety of other illnesses as well as autonomic neuropathy itself. Autonomic dysfunction can also result from disorders of the brain or spinal cord, such as multiple system atrophy [48]. Fothergill illness, tic douloureux, and trifacial neuralgia are some other names for this disorder. The trigeminal nerve is another name for the nerve that controls facial sensation as well as motor functions like biting and chewing. This type of pain is referred to as neuropathic pain. There are two main classifications for trigeminal neuralgia: atypical and normal. Attacks of sharp, sudden, electric-like pain on one side of the face, lasting anywhere from a few seconds to several minutes at a time, are the hallmark of the usual variety. These episodes can happen in clusters over the course of several hours. The atypical variation produces a constant, mildly excruciating discomfort, unlike the regular variety. Even the smallest touch to the face can trigger an incident. The same person may exhibit both manifestations. Depression is a common side effect, and it is regarded as one of the most painful disorders that may be treated with medication. It is believed to be caused by a degradation of the myelin sheath around the trigeminal nerve, while the exact cause is unknown [49]. This could be caused by trauma, multiple sclerosis, strokes, or any other illness where a blood artery compresses a neuron as it leaves the brain stem. Two less common causes of this disease are tumours and arteriovenous malformations. This type of nerve pain has the potential to be quite severe [50]. After ruling out other likely causes, including postherpetic neuralgia, the symptoms are frequently utilised to establish a diagnosis. Both medication and surgery are options for treating a patient. Approximately 90% of individuals respond well to the anticonvulsant drugs carbamazepine or oxcarbazepine when administered as the first line of therapy. Up to 23% of patients say that they have adverse effects frequently enough to force them to discontinue their prescription [51]. Other options include amitriptyline, lamotrigine, baclofen, gabapentin, and pimozide. Opioids prepared traditionally frequently don’t have the intended therapeutic effect. Patients who do not improve or who become resistant to standard therapies may be tried with a range of surgical techniques. It is estimated that one in every 8,000 people may get trigeminal neuralgia at some point throughout their lives. People over 50 are typically the ones who first experience it. That could, however, affect people of any age. Women are more likely than men to be affected by the illness. The first person to give a thorough description of the illness was John Fothergill in 1773 [52]. Chronic pain is a major cause of disability and disease burden [68], making its management a major challenge for all healthcare systems. Over 100 million people in the US suffer from chronic pain, one of the most prevalent and crippling medical conditions. Furthermore, it should be noted that the annual cost of chronic pain ranges from $560 to $635 billion [53–55], surpassing the combined costs of healthcare and lost productivity associated with diabetes, heart disease, and cancer. Even though chronic pain has many negative repercussions, its prevalence is rising in the US. As a type of chronic pain, neuropathy is very common.Neuropathic pain has been defined as “pain induced by a lesion or illness of the somatosensory nervous system” [56]. Neuropathic pain is caused by a variety of circumstances, and its underlying pathophysiology is still not well understood. It has been shown that the use of an interdisciplinary team in the treatment of neuropathic pain can alleviate pain, improve functioning, and elevate mood [57]. NSAIDs and opioids, two common analgesics, work better in nociceptive pain than in neuropathic pain. The preferred pharmacological therapy for neuropathic pain includes gabapentinoids, topical medicines, tricyclic antidepressants, and serotonin-norepinephrine reuptake inhibitors. These medications have a number of dangers that need to be carefully considered despite their potential effectiveness, especially for people with renal impairment, liver illness, cardiac abnormalities, and mood problems [58]. Although the majority of prior research has focused on the peripheral effects of flavonoids, studies using rat and cow brain membrane binding tests have shown their preferential affinity for GABAA receptors. Apart from studies on binding, a range of behavioural research has also been carried out, all of which indicate that the anxiolytic benefits of flavonoids in rat anxiety models do not include the excess side effects of benzodiazepines, or BDZs. A variety of synthetic flavonoids with a high affinity for the BDZ binding site have been developed as a result of what was previously believed to be their action on BDZ receptors. They were later found to be resistant to flumazenil, an antagonist of the BDZ receptor, suggesting that this family of drugs targets a distinct receptor. A selective functional group was added to flavones at the 6 or 3′ locations to increase their affinity for BDZ receptors. Moreover, the GABA ratios were established by using the effect of ligand binding on GABA binding. These ratios demonstrated the potent biological activity of flavones at BDZ receptors. At these receptors, 6-bromoflavone, 6-Bromo-3′-nitroflavone, and 6-chloro-3′-nitroflavone have been shown to exhibit full agonist, partial agonist, and antagonist properties, with corresponding GABA ratios of 1.6-2.0, 1.38, and 2.0 [59-61]. Strong inhibitory effects are produced by positive ionotropic modulators of GABAA receptors, which increase the influx of chloride ions. As a result, there is significant potential for these modulators to treat a variety of central nervous system illnesses, including neuropathic pain, anxiety disorders, seizures, muscular spasms, and sleep issues. Moreover, opportunities to look for novel therapeutic drugs with less side effects have been presented by the discovery that flavonoids may function upon distinct binding sites other than the traditional benzodiazepine binding site. The 122L and 222L GABAA receptor subunits are positively allosterically modulated by 6-methylflavonone, according the literature. Alterations in the activity of recombinant GABAA receptors are linked to the substitution of flavone 6-position. The 6-hydroxy flavone dramatically altered the BDZ site that is flumazenil-sensitive. It has been demonstrated that six-methoxyflavanone and six-methoxy flavone possess strong anti-allodynic properties in neuropathic pain models induced by streptozotocin and cisplatin, respectively. The protective effects of these drugs against neuropathic pain have been associated with their positive allosteric modulatory actions on GABAA and opioid receptors. In addition, myricetin and baicalin produced notable anti-allodynic effects in models of sciatic nerve ligation. It has been reported that rutin and quercetin can inhibit persistent painful peripheral neuropathy generated by oxaliplatin. Additionally, naringin has been reported to exhibit anti-allodynic potential in the painful diabetic neuropathy caused by streptozotocin [62–65].In addition to their established effects on GABAA receptors, flavonoids also have anti-inflammatory and antioxidant qualities. The underlying cause of nearly all metabolic diseases is oxidative stress. Apart from being susceptible to external harm, cells and tissues are also in a permanent state of danger due to the production of free radicals and reactive oxygen species, which are byproducts of the body’s regular oxygen metabolism. The anti-oxidant properties of flavonoids are well recognised, and numerous studies have demonstrated their positive effects on a range of illnesses [66]. Even if the exact sequence of events underlying the damage caused by free radicals to cellular functions is not fully understood, the contribution of lipid peroxidation leading to cellular membrane destruction and activation of inflammatory mediators by the free radicals culminating in ultimate tissue damage can provide a lot of help in conceiving a pharmacological target. Enzymes like superoxide dismutase and glutathione peroxidase, catalase, and nonenzymatic compounds like ascorbic acid and beta-tocopherol are among the body’s natural defences against reactive oxygen species (ROS). Nevertheless, these endogenous scavenging molecules may be depleted due to rising oxidative stress caused by many clinical conditions, especially disorders like diabetes mellitus that cause neuropathic pain [67]. The enzyme xanthine dehydrogenase normally converts xanthine to uric acid, but during an ischemia-reperfusion event, it changes into xanthine oxidase, which is a precursor to free radicals. The antioxidant properties of quercetin, luteolin, and silybin—which block xanthine oxidase—have been extensively studied. Similar to ischemia, reperfusion mobilises leucocytes, which release cytotoxic oxidants and inflammatory mediators, activating the complement system. Leucocyte immobilisation is thought to be facilitated by a variety of flavonoids, which also lower inflammation and the serum complement system. Numerous studies have shown that there are shared pathophysiological routes between peripheral neuropathic pain and inflammation. Clinically, both conditions manifest as either hyperallergic (abnormally decreased pain sensitivity) or allodynia (abnormally heightened pain perception) [68]. Damage to peripheral nerves results in the invasion of inflammatory cells and their waste products, such as cytokines and arachidonic acid, which are released for nerve regeneration and cause chronic pain. Rats were given injections of cytokines such as tumour necrosis factor- (TNF-), interleukin-1 (IL-1), and interleukin-6 (IL-6) to cause both mechanical and thermal hyperalgesia. In mice with painful neuropathy, hyperalgesia was lessened when TNF- was inhibited. Cytokines, once released, in a COX-2-dependent way, cause the production of more cytokines as well as the release of prostanoids. It has been well shown that PGs cause two effects: inflammation and heightened sensitivity to pain. It has been demonstrated that flavonoids reduce inflammation in both lab dishes and animal trials. In vivo anti-inflammatory effects are attributed to inhibition of eicosanoid-generating enzymes, including phospholipase A2, lipoxygenase (LOX), and cyclooxygenase (COX) [69]. Numerous enzyme systems are known to be impacted by flavonoids; for instance, arachidonic acid is not able to suppress the inflammatory response. This gives the group additional anti-thrombotic and anti-inflammatory qualities. They also stop neutrophils from generating ROS and releasing peroxidase. This results in the inhibition of alpha-1 antitrypsin’s activity. Certain flavonoids remove a potentially chaotic component in the production of free radicals by blocking iron chelation, which causes lipid peroxidation [70].
- CONCLUSION
Flavonoids have been demonstrated to be a potential novel treatment for neuropathic pain in preclinical animals. Clinical evidence from humans is still being investigated, though. GABAA receptor allosteric modulators alter the agonistic potency or specificity of GABA, hence regulating its action. Since our understanding of GABAA receptor subtypes has increased over the past ten years, these modulators have received a great deal of attention. Because flavonoids are potent allosteric modulators, they may be helpful in the treatment of neuropathic pain and other painful conditions. However, further investigation is required to determine the specific location of these bioactive chemicals over the GABAA receptors. The effects of flavonoids, such as genistein, on male C57BL/6J mice are covered in this article. By reducing the generation of pro-inflammatory cytokines and reactive oxygen species and increasing the amount of NGF in the diabetic sciatic nerve, it helps treat diabetic peripheral neuropathy. It led to dilating and reduced blood levels of inflammatory biomarkers. For ninety days, 420 mg of silymarin was used daily to lessen joint discomfort, edoema, and soreness.
REFERENCES
- Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. (September 2020). “The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises.” Pain. 161 (9): 1976–1982. doi:10.1097/j.pain.0000000000001939. PMC 7680716. PMID 32694387.
- Cervero F (2012). Understanding Pain : Exploring the Perception of Pain. Cambridge, Mass.: MIT Press. pp. Chapter 1. ISBN 9780262305433. OCLC 809043366.
- Raj PP (2007). “Taxonomy and classification of pain”. In: The Handbook of Chronic Pain. Nova Biomedical Books. ISBN 9781600210440. Archived from the original on 30 March 2021. Retrieved 3 February 2016.
- Debono DJ, Hoeksema LJ, Hobbs RD (August 2013). “Caring for patients with chronic pain: pearls and pitfalls”. The Journal of the American Osteopathic Association. 113 (8): 620–7. doi:10.7556/jaoa.2013.023. PMID 23918913.
- Turk DC, Dworkin RH (2004). “What should be the core outcomes in chronic pain clinical trials?”. Arthritis Research & Therapy. 6 (4): 151–4. doi:10.1186/ar1196. PMC 464897. PMID 15225358.
- Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK, Kvarstein G, Stubhaug A (July 2008). “Assessment of pain”. British Journal of Anaesthesia. 101 (1): 17–24. doi:10.1093/bja/aen103. PMID 18487245.
- Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L (November 2015). “Non-prescription (OTC) oral analgesics for acute pain – an overview of Cochrane reviews”. The Cochrane Database of Systematic Reviews. 11 (11): CD010794. doi:10.1002/14651858.CD010794.pub2. PMC 6485506. PMID 26544675.
- Eisenberger NI, Lieberman M (2005). “Why it hurts to be left out: The neurocognitive overlap between physical and social pain” (PDF). In Williams KD (ed.). The Social Outcast: Ostracism, Social Exclusion, Rejection, & Bullying (Sydney Symposium of Social Psychology). East Sussex: Psychology Press. p. 210. ISBN 9781841694245.
- Garland EL, Brintz CE, Hanley AW, Roseen EJ, Atchley RM, Gaylord SA, et al. (January 2020). “Mind-Body Therapies for Opioid-Treated Pain: A Systematic Review and Meta-analysis”. JAMA Internal Medicine. 180 (1): 91–105. doi:10.1001/jamainternmed.2019.4917. PMC 6830441. PMID 31682676.
- Weyers H (September 2006). “Explaining the emergence of euthanasia law in the Netherlands: how the sociology of law can help the sociology of bioethics”. Sociology of Health & Illness. 28 (6): 802–16. doi:10.1111/j.1467-9566.2006.00543.x. PMID 17184419.
- Lewis CT, Short C. “Poena”. A Latin Dictionary. Archived from the original on 13 May 2011 – via Perseus Digital Library.
- Liddell HG, Scott R. “ποινή”. A Greek-English Lexicon. Archived from the original on 13 May 2011 – via Perseus Digital Library.
- “Pain”. Archived from the original on 28 July 2011 – via Online Etymology Dictionary.
- Merskey H, Bogduk N (1994). Classification of Chronic Pain (2 nd ed.). Seattle: International Association for the Study of Pain. pp. 3 & 4. ISBN 978-0931092053.
- Turk DC, Okifuji A (2001). “Pain terms and taxonomies of pain”. In Bonica JJ, Loeser JD, Chapman CR, Turk DC (eds.). Bonica’s management of pain. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 9780781768276.
- Coda BA, Bonica JJ (2000). “General considerations of acute pain”. In Panswick CC, Main CJ (eds.). Pain management: an interdisciplinary approach. Edinburgh: Churchill Livingstone. ISBN 9780443056833.
- Thienhaus O, Cole BE (2002). “Classification of pain”. In Weiner R (ed.). Pain management: a practical guide for clinicians. Boca Raton: CRC Press. pp. 28. ISBN 9780849322624.
- Jensen TS, Finnerup NB (September 2014). “Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms”. The Lancet. Neurology. 13 (9): 924–35. doi:10.1016/s1474-4422(14)70102-4. PMID 25142459. S2CID 25011309.
- Lolignier S, Eijkelkamp N, Wood JN (January 2015). “Mechanical allodynia”. Pflügers Archiv. 467 (1): 133–9. doi:10.1007/s00424-014-1532-0. PMC 4281368. PMID 24846747.
- Kooijman CM, Dijkstra PU, Geertzen JH, Elzinga A, van der Schans CP (July 2000). “Phantom pain and phantom sensations in upper limb amputees: an epidemiological study”. Pain. 87 (1): 33–41. doi:10.1016/S0304-3959(00)00264-5. PMID 10863043. S2CID 7565030.
- Jensen TS, Krebs B, Nielsen J, Rasmussen P (November 1983). “Phantom limb, phantom pain and stump pain in amputees during the first 6 months following limb amputation”. Pain. 17 (3): 243–56. doi:10.1016/0304-3959(83)90097-0. PMID 6657285. S2CID 10304696.
- Jensen TS, Krebs B, Nielsen J, Rasmussen P (March 1985). “Immediate and long-term phantom limb pain in amputees: incidence, clinical characteristics and relationship to pre-amputation limb pain”. Pain. 21 (3): 267–78. doi:10.1016/0304-3959(85)90090-9. PMID 3991231. S2CID 24358789.
- Wall PD, Melzack R (1996). The challenge of pain (2nd ed.). New York: Penguin Books. ISBN 9780140256703.
- Ramachandran VS, Rogers-Ramachandran D (April 1996). “Synaesthesia in phantom limbs induced with mirrors”. Proceedings. Biological Sciences. 263 (1369): 377–86. Bibcode:1996RSPSB. 263..377R. doi:10.1098/rspb.1996.0058. PMID 8637922. S2CID 4819370.
- Mishra S, Bhatnagar S, Chaudhary P, Rana SP (January 2009). “Breakthrough cancer pain: review of prevalence, characteristics and management”. Indian Journal of Palliative Care. 15 (1): 14–8. doi:10.4103/0973-1075.53506. PMC 2886208. PMID 20606850.
- Caraceni A, Hanks G, Kaasa S, Bennett MI, Brunelli C, Cherny N, Dale O, De Conno F, Fallon M, Hanna M, Haugen DF, Juhl G, King S, Klepstad P, Laugsand EA, Maltoni M, Mercadante S, Nabal M, Pigni A, Radbruch L, Reid C, Sjogren P, Stone PC, Tassinari D, Zeppetella G (February 2012). “Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC” (PDF). The Lancet. Oncology. 13 (2): e58-68. doi:10.1016/S1470-2045(12)70040-2. PMID 22300860. Archived from the original (PDF) on 19 October 2014.
- Beecher HK (1959). Measurement of subjective responses. New York: Oxford University Press. cited in Melzack R, Wall PD (1996). The challenge of pain (2nd ed.). London: Penguin. p. 7. ISBN 978-0-14-025670-3.
- “International Association for the Study of Pain: Pain Definitions”. Archived from the original on 13 January 2015. Retrieved 12 January 2015. Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage Alt URL[permanent dead link] Derived from Bonica JJ (June 1979). “The need of a taxonomy”. Pain. 6 (3): 247–8. doi:10.1016/0304-3959(79)90046-0. PMID 460931. S2CID 53161389.
- “International Association for the Study of Pain | Pain Definitions”.. Retrieved 12 October 2010.
- Grahek N (2007). Feeling pain and being in pain (2nd ed.). Cambridge, Mass.: MIT Press. ISBN 978-0-262-51732-4. Archived from the original on 27 September 2008.
- Nagasako EM, Oaklander AL, Dworkin RH (February 2003). “Congenital insensitivity to pain: an update”. Pain. 101 (3): 213–9. doi:10.1016/S0304-3959(02)00482-7. PMID 12583863. S2CID 206055264.
- “Taxonomy”. International Association for the study of pain. Archived from the original on 13 January 2015. Retrieved 3 May 2015.
- Kaur, Jaskirat; Ghosh, Shampa; Sahani, Asish Kumar; Sinha, Jitendra Kumar (June 2019). “Mental imagery training for treatment of central neuropathic pain: a narrative review”. Acta Neurologica Belgica. 119 (2): 175–186. doi:10.1007/s13760-019-01139-x. PMID 30989503. S2CID 115153320.
- De Courcy, Jonathan; Liedgens, Hiltrud; Obradovic, Marko; Holbrook, Tim; Jakubanis, Rafal (April 2016). “A burden of illness study for neuropathic pain in Europe”. ClinicoEconomics and Outcomes Research. 8: 113–126. doi:10.2147/CEOR.S81396. PMC 4853004. PMID 27217785.
- Torrance N, Smith BH, Bennett MI, Lee AJ (April 2006). “The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey”. J Pain. 7 (4): 281–9. doi:10.1016/j.jpain.2005.11.008. PMID 16618472.
- Bouhassira, Didier; Lantéri-Minet, Michel; Attal, Nadine; Laurent, Bernard; Touboul, Chantal (June 2008). “Prevalence of chronic pain with neuropathic characteristics in the general population” (PDF). Pain. 136 (3): 380–387. doi:10.1016/j.pain.2007.08.013. PMID 17888574. S2CID 599627.
- Freemon, Frank R. (1994). “Galen’s ideas on neurological function”. J Hist Neurosci. 3 (4): 263–71. doi:10.1080/09647049409525619. PMID 11618827.
- Heydari, Mojtaba; Shams, Mesbah; Hashempur, Mohammad Hashem; Zargaran, Arman; Dalfardi, Behnam; Borhani-Haghighi, Afshin (2015). “The origin of the concept of neuropathic pain in Early Medieval Persia (9th–12th century CE)”. Acta Medico-historica Adriatica. 13 Suppl 2: 9–22. PMID 26966748. S2CID 30398883.
- Scadding, JW (March 2004). “Treatment of neuropathic pain: historical aspects”. Pain Medicine. 5 Suppl 1: S3-8. doi:10.1111/j.1526-4637.2004.04018.x. PMID 14996226.
- Baron, Ralf; Binder, Andreas; Wasner, Gunnar (August 2010). “Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment”. The Lancet Neurology. 9 (8): 807–819. doi:10.1016/S1474-4422(10)70143-5. PMID 20650402. S2CID 14267074.
- Portenoy RK (1989). “Painful polyneuropathy”. Neurol Clin. 7 (2): 265–88. doi:10.1016/S0733-8619(18)30813-2. PMID 2566901.
- Chemotherapy-induced Peripheral Neuropathy Fact Sheet, Retrieved on 29 December 2008
- Archived 2009-07-08 at the Wayback Machine Cancerbackup, Macmillan Cancer Support, Peripheral neuropathy, Retrieved on 29 December 2008
- Freynhagen, R; Bennett, M I (12 August 2009). “Diagnosis and management of neuropathic pain”. BMJ. 339 (aug12 1): b3002. doi:10.1136/bmj.b3002. PMC 6130809. PMID 19675082.
- Fabry, Vincent; Gerdelat, Angélique; Acket, Blandine; Cintas, Pascal; Rousseau, Vanessa; Uro-Coste, Emmanuelle; Evrard, Solène M.; Pavy-Le Traon, Anne (5 May 2020). “Which Method for Diagnosing Small Fiber Neuropathy?”. Frontiers in Neurology. 11: 342. doi:10.3389/fneur.2020.00342. PMC 7214721. PMID 32431663.
- Porubcin, Michal G.; Novak, Peter (17 April 2020). “Diagnostic Accuracy of Electrochemical Skin Conductance in the Detection of Sudomotor Fiber Loss”. Frontiers in Neurology. 11: 273. doi:10.3389/fneur.2020.00273. PMC 7212463. PMID 32425871.
- Kaur, Jaskirat; Ghosh, Shampa; Sahani, Asish Kumar; Sinha, Jitendra Kumar (November 2020). “Mental Imagery as a Rehabilitative Therapy for Neuropathic Pain in People With Spinal Cord Injury: A Randomized Controlled Trial”. Neurorehabilitation and Neural Repair. 34 (11): 1038–1049. doi:10.1177/1545968320962498. PMID 33040678. S2CID 222300017.
- “Neurogenic Bladder: Overview, Neuroanatomy, Physiology and Pathophysiology”. 2019-12-05.
- “What Is Microvascular Cranial Nerve Palsy?”. aao.org. 1 September 2017. Archived from the original on 22 December 2017.
- “Trigeminal Neuralgia Fact Sheet”. NINDS. National Institutes of Health. 17 March 2020. Retrieved 5 April 2021.
- Obermann, Mark (2010-03-01). “Treatment options in trigeminal neuralgia”. Therapeutic Advances in Neurological Disorders. 3 (2): 107–115. doi:10.1177/1756285609359317. ISSN 1756-2856. PMC 3002644. PMID 21179603.
- “Trigeminal Neuralgia”.
- Cruccu, Giorgio; Di Stefano, Giulia; Truini, Andrea (2020-08-20). Ropper, Allan H. (ed.). “Trigeminal Neuralgia”. New England Journal of Medicine. 383 (8): 754–762. doi:10.1056/NEJMra1914484. ISSN 0028-4793. PMID 32813951. S2CID 221201036.
- Gritsch, Simon; Bali, Kiran Kumar; Kuner, Rohini; Vardeh, Daniel (January 2016). “Functional characterization of a mouse model for central post-stroke pain”. Molecular Pain. 12: 174480691662904. doi:10.1177/1744806916629049. PMC 4956143. PMID 27030713.
- Costigan, Michael; Scholz, Joachim; Woolf, Clifford J. (1 June 2009). “Neuropathic Pain: A Maladaptive Response of the Nervous System to Damage”. Annual Review of Neuroscience. 32 (1): 1–32. doi:10.1146/annurev.neuro.051508.135531. PMC 2768555. PMID 19400724.
- Manion, John; Waller, Matthew A.; Clark, Teleri; Massingham, Joshua N.; Neely, G. Gregory (20 December 2019). “Developing Modern Pain Therapies”. Frontiers in Neuroscience. 13: 1370. doi:10.3389/fnins.2019.01370. PMC 6933609. PMID 31920521.
- Henderson, L. A.; Peck, C. C.; Petersen, E. T.; Rae, C. D.; Youssef, A. M.; Reeves, J. M.; Wilcox, S. L.; Akhter, R.; Murray, G. M.; Gustin, S. M. (24 April 2013). “Chronic Pain: Lost Inhibition?”. Journal of Neuroscience. 33 (17): 7574–7582. doi:10.1523/JNEUROSCI.0174-13.2013. PMC 6619566. PMID 23616562.
- Ji, Ru-Rong; Donnelly, Christopher R.; Nedergaard, Maiken (November 2019). “Astrocytes in chronic pain and itch”. Nature Reviews Neuroscience. 20 (11): 667–685. doi:10.1038/s41583-019-0218-1. PMC 6874831. PMID 31537912.
- Ji, Ru-Rong; Chamessian, Alexander; Zhang, Yu-Qiu (4 November 2016). “Pain regulation by non-neuronal cells and inflammation”. Science. 354 (6312): 572–577. Bibcode:2016Sci… 354..572J. doi:10.1126/science. aaf8924. PMC 5488328. PMID 27811267.
- Siniscalco, Dario; Giordano, Catia; Rossi, Francesco; Maione, Sabatino; de Novellis, Vito (1 December 2011). “Role of Neurotrophins in Neuropathic Pain”. Current Neuropharmacology. 9 (4): 523–529. doi:10.2174/157015911798376208. PMC 3263449. PMID 22654713.
- Latremoliere, Alban; Woolf, Clifford J. (September 2009). “Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity”. The Journal of Pain. 10 (9): 895–926. doi:10.1016/j.jpain.2009.06.012. PMC 2750819. PMID 19712899.
- Ji, Ru-Rong; Kohno, Tatsuro; Moore, Kimberly A; Woolf, Clifford J (December 2003). “Central sensitization and LTP: do pain and memory share similar mechanisms?”. Trends in Neurosciences. 26 (12): 696–705. doi:10.1016/j.tins.2003.09.017. PMID 14624855. S2CID 14214986.
- Truini A, Cruccu G (May 2006). “Pathophysiological mechanisms of neuropathic pain”. Neurol. Sci. 27 Suppl 2: S179–82. doi:10.1007/s10072-006-0597-8. PMID 16688626. S2CID 28736907.
- Tadokoro, Takahiro; Bravo-Hernandez, Mariana; Agashkov, Kirill; Kobayashi, Yoshiomi; et al. (May 2022). “Precision spinal gene delivery-induced functional switch in nociceptive neurons reverses neuropathic pain”. Molecular Therapy. 30 (8): 2722–2745. doi:10.1016/j.ymthe.2022.04.023. PMC 9372322. PMID 35524407. S2CID 248553626.
- Nolano M, Simone DA, Wendelschafer-Crabb G, Johnson T, Hazen E, Kennedy WR (1999). “Topical capsaicin in humans: parallel loss of epidermal nerve fibers and pain sensation”. Pain. 81 (1–2): 135–45. doi:10.1016/S0304-3959(99)00007-X. PMID 10353501. S2CID 8952555.
- Delage B (November 2015). “Flavonoids”. Linus Pauling Institute, Oregon State University, Corvallis, Oregon. Retrieved 2021-01-26.
- de Souza Farias SA, da Costa KS, Martins JB (April 2021). “Analysis of Conformational, Structural, Magnetic, and Electronic Properties Related to Antioxidant Activity: Revisiting Flavan, Anthocyanidin, Flavanone, Flavonol, Isoflavone, Flavone, and Flavan-3-ol”. ACS Omega. 6 (13): 8908–8918. doi:10.1021/acsomega.0c06156. PMC 8028018. PMID 33842761.
- Department of Anesthesiology, New York-Presbyterian, Weill Cornell Medical College, 525 East 68th Street, Box 124, New York, NY 10065, USA
- Southcoast Health, Southcoast Health Physicians Group, New Bedford, MA, USA
- Department of Anesthesiology, Louisiana State University Health Shreveport, Shreveport, LA, USA
Publication History
Submitted: September 02, 2023
Accepted: September 20, 2023
Published: October 01, 2023
Identification
D-0148
Citation
Jamal Ahammed, Ferdous Alam, Al Rezowan Shoron, Md. Amir Hamja Niloy, Sumitro Das, Biswajit Kumar Utpal & Sumon Chandraw Roy (2023). A Review on Flavonoids in Neuropathic Pain. Dinkum Journal of Medical Innovations, 2(10):452-465.
Copyright
© 2023 DJMI. All rights reserved