

")
Publication History
Submitted: October 05, 2023
Accepted: October 20, 2023
Published: November 01, 2023
Identification
D-0196
Citation
Jamil Raza & Sidra Anwar (2023). Cardiovascular Findings in Women Delivered At Advanced Maternal Age. Dinkum Journal of Medical Innovations, 2(11):466-472.
Copyright
© 2023 DJMI. All rights reserved
466-472
Cardiovascular Findings in Women Delivered At Advanced Maternal AgeReview Article
Jamil Raza 1*, Sidra Anwar 2
- Punjab Institute of Cardiology, Lahore, Pakistan; razajamil34@gmail.com
- Punjab Institute of Cardiology, Lahore, Pakistan; sidraanwar56@yahoo.com
* Correspondence: razajamil34@gmail.com
Abstract: Over the past few decades, there has been an increase in adverse cardiovascular outcomes during pregnancy due to a rise in the number of women giving birth later in age. Higher incidence of female obesity, diabetes, hypertension, cardiovascular illnesses, and the use of assisted reproductive technologies, which has increased fertility are additional causes. Extensive prenatal maternal screening, ongoing pregnancy supervision, monitoring during labor, delivery, and the puerperium, and thorough anesthetic evaluation during delivery are all necessary for those who are at risk. The current review summarizes the pertinent data on cardiovascular outcomes in older mothers giving birth as well as the associated medicolegal concerns. Ovid conducted a search using the following terms: “cardiomyopathy,” “ischaemic heart disease,” “arrhythmias,” “hypertension,” “peripartum period,” “diabetes,” “advanced maternal age,” “anesthesia,” “maternal morbidity and mortality,” and “litigation.” The search was conducted on the Pubmed, Cochrane, Semantic Scholar, Medline, and Embase databases. Underestimating peripartum cardiomyopathy (PPCM) risk factors can have a negative effect on both mother and fetal outcomes. Misdiagnosis or mismanagement can have significant legal ramifications, including large compensatory damages. Increases in insurance premiums are caused by substantial indemnity payments. For optimal pregnancy monitoring and delivery results, obstetricians, cardiologists, anesthesiologists, and perinatologists must use multidisciplinary techniques.
Keywords: cardiovascular, maternity, advanced maternal age
- INTRODUCTION
A lady who is 35 years of age or older on the anticipated date of delivery is considered to be of advanced maternal age (AMA) [1-3]. A new dimension of what medical professionals once referred to as pregnancy in the “older gravida” is motherhood at or beyond the border of reproductive age [4]. The incidence of AMA has recently increased, particularly in high-income nations, as a result of the combined effects of societal changes and medical advancement, and some women are even delaying motherhood into their forties [5-7]. Studies conducted worldwide have shown that certain cardiovascular risk factors, such as hypertensive disorders (including chronic hypertension, gestational hypertension, preeclampsia, and eclampsia) or glycometabolic disorders, and their corresponding cardiovascular consequences (including peripartum cardiomyopathy; PPCM), ischemic cardiac events, arrhythmias, and sudden cardiac death), may manifest more frequently in older mothers due to pre-existing medical conditions [8–12]. It has also been proposed that women who are 45 years of age or older, or who have reached very advanced maternal age (vAMA), are much more vulnerable to unfavorable pregnancy outcomes than women who have reached AMA [13]. Concerning this, assisted reproductive technology has provided this group of women an enhanced chance of becoming pregnant even though fertility decreases with age [11–13]. In this study, pertinent data on cardiovascular outcomes in women who give birth before their due date and the unfavorable legal developments around these outcomes for both the mother and the fetus are presented from throughout the world.
- MATERIALS AND METHODS
Ovid visited the multidisciplinary research databases Pubmed, Cochrane, Semantic Scholar, Medline, and Embase, where a literature search was conducted to find all relevant papers up to 2023. Cardiomyopathy, ischemic heart disease, arrhythmias, hypertension, peripartum duration, obesity, advanced maternal age, preeclampsia, eclampsia, anesthetic, maternal morbidity and mortality, and litigation were among the terms that were included in the search. The search was restricted to human studies and English-language publications. To find pertinent papers, two impartial reviewers looked through abstracts, full article studies, and titles. All-cause mortality and cardiovascular outcomes with long-term follow-up reported results (≥1 year) were included in the retrospective and prospective studies that were chosen. Excluded were case reports, case series, and sample sizes less than ten. The demographic details from each trial, including age, ethnicity, comorbidities, length of follow-up, and reported mortality, were taken out whenever possible. Cardiovascular events, such as hypertension, preeclampsia, new onset cardiomyopathy, arrhythmias, diabetes mellitus, and all-cause mortality, were the main outcomes of interest. The relevant independent variable was the mother’s age at delivery. Court situations in which peripartum cardiomyopathy had occurred but did not immediately result in unfavorable repercussions were dismissed with regard to medico-legal issues linked to misdiagnosis of PPCM. After a thorough search of legal databases, five cases were chosen for consideration based on how well they presented the idea that peripartum cardiomyopathy was the cause of the patient’s poor clinical outcome. It was thereafter limited to cases where the extent of compensatory damages awarded was disclosed along with the ultimate decision.
- RESULTS AND DISCUSSION
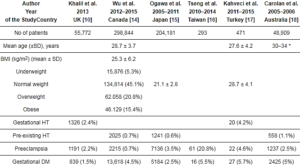
After eliminating duplicates from the original 156 publications, a total of 206 papers were taken into consideration and examined. Sadly, 95 papers were not included since there was no documented classification according to mother age. Ultimately, our evaluation contained eleven publications with quantitative data on the prevalence of cardiovascular events comparing the AMA to the pregnant population under 35 [14–23]. Only the discussion section’s quantitative data was taken into consideration in support of other studies for which there were no available quantitative data to bolster our claims. The demographic features, cardiovascular outcomes, and risk factor incidence of severe maternal morbidity due to cardiovascular disease in delivering mothers who are 35 years of age or older (AMA) in the studies under consideration are summarized in Tables 1 and 2. Regretfully, the statistical assessment of any noteworthy disparity in results between women under 35 and those over 35 who give birth was absent from the published research. Thus, the only clinical characteristic that could be reported was the prevalence of the traits under review. Nonetheless, a tendency in the two groups’ varying prevalence of cardiovascular problems is discernible. Compared to the group under 35 years old, there was a higher incidence of glycometabolic diseases and hypertension in the AMA group. Preeclampsia prevalence in the AMA group was 0.9% to 25.8%, while in the group under 35 years old, it ranged from 0.7% to 20.8%. In AMA women, the prevalence of gestational diabetes varied from 2.5% to 14.8%, whereas in the group under 35 years old, it ranged from 1.5% to 5.7%. The incidence of PPCM varied between 0.008% and 0.4% in the AMA group and between 0.005% and 0.2% in the <35 years group [19–23]. In the AMA group, the prevalence of arrhythmias ranged from 0.005% to 0.19%, whereas in the group of those under 35 years, it ranged from 0.005% to 0.05% [19, 21]. At the time of release, 0.004-0.049% of the AMA group and 0.004-0.016% of the group under 35 had an acute myocardial infarction diagnosis [19, 20]. The AMA group had a two-fold higher prevalence of aortic dissection [19]. Asystole happened a day following an elective cesarean delivery, and there were two instances of abrupt cardiac mortality in the AMA group as a result of ventricular fibrillation in the condition of cardiogenic shock [22].
Table 01: Demographics and Characteristics of Studies
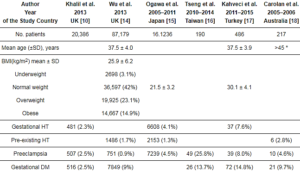
Table 02: Demographic and cardiovascular aspects and incidence of severe maternal morbidity due to cardiovascular disease in <35 years old pregnant women
Over the past few decades, the number of pregnancies at advanced maternal ages (over 35) has increased in many high-income nations [24–26]. Recent reports have indicated rates as high as 9.1% in the US [27] and 28.1% in Japan [28]. This has led to the observation that women who give birth to babies via AMA are more likely than their younger counterparts to experience a negative cardiovascular result [29]. Regarding this matter, hypertension issues represent the most common cardiovascular outcome during pregnancy and are closely associated with the advanced age of the expectant mother. In fact, a decrease in insulin sensitivity and an aberrant lipid profile with elevated levels of cholesterol and triglycerides are linked to age-related glucose intolerance [5]. According to nationwide statistics from the United States, the risk of late-onset pre-eclampsia increases by 4% for every year over the age of thirty-two [31], while the risk of pre-eclampsia does not appear to be affected by age before thirty-five [30]. That is supported by the finding of a sizable population-based study conducted in the Canadian province of Ontario, which indicated that mothers older than 43 were more likely to experience an adverse event cardiovascular composite outcome that included gestational diabetes and preeclampsia [14]. In Texas, USA, more recently (2013–2014), it was observed that the very advanced maternal age (vAMA) at childbirth (>45 years) had a higher frequency (p < 0.05) of pregestational diabetes, chronic hypertension, and pregnancy-related hypertensive disorders than the youngest maternal age group [32].
In a similar vein, a cross-sectional study conducted in Japan revealed that pregnant women 45 years of age and above were 1.5–2 times more likely than younger women (aged 30-34) to experience maternal morbidity. In particular, women over 45 who give birth are at a heightened risk of developing preeclampsia, particularly severe cases of the condition [33]. Moreover, contrary to other reports in the literature, multiparous women experienced a higher influence of maternal age on preeclampsia and severe preeclampsia than primiparous women [34]. Given that preeclampsia is thought to be strongly associated with both primiparity and advanced age, older primiparous women may be more likely to be prescribed medication than older multiparous women [35]. According to the Japanese study mentioned above, older multiparous women as well as primiparous women should take this approach into consideration [15]. Similar findings were also reported in a 2013 UK-based study that determined the predictive value of preeclampsia and gestational diabetes to be significantly influenced by the following factors: weight, chronic hypertension, Type 1 diabetes, previous preeclampsia, family history of preeclampsia, and maternal ages of 35 to 39.9 years or older [10]. Comparable findings were shown in the Australian Registry of Births, where women who were 45 years of age or older and classified as very advanced maternal age (vAMA) had a higher frequency of pregnancy complications like gestational diabetes, antepartum hemorrhage, preeclampsia, and caesarean sections [18]. For healthy women who had been tested to rule out pre-existing disease, a trend of positive outcomes was visible, even at highly advanced maternal age (50–65 years). In the USA, from 2004 to 2011, women between the ages of 40 and 54 had the highest incidence of PPCM (36.7 (95% CI 35.4 to 37.9) per 10,000 live births). Of these patients, 20% to 50% also had a moderate to severe risk of left ventricular function deterioration, which could persist after delivery [35–37]. A prospective population-based cohort study conducted in the Netherlands between 2004 and 2006 also found that pre-existing hypertension and an increasing incidence of older mothers were significant risk factors for the development of PPCM during pregnancy [19]. These findings highlight the fact that AMA is a significant risk factor for the development of PPCM and that pregnant women in this category need to have their pregnancies well monitored.
Comparably, women 41 to 50 years of age had an overall higher frequency of any arrhythmia and a greater increase in any arrhythmia over time (199 per 100,000 and 162% increase) compared to women 18 to 30 years of age (55 per 100,000 and 58% increase) in a large USA study conducted between 2000 and 2012 [21]. The prevalence of arrhythmias, particularly atrial arrhythmias, often rises with age. When arrhythmias occur during pregnancy, medication use is restricted due to possible fetal toxicity, which makes patient care very challenging. Regarding myocardial infarction, there were 859 instances of acute myocardial infarction among the pregnancy-related discharges in the USA between 2000 and 2002 [44]. Of these, 233 (27%) required hospital readmission after giving birth, while 626 (73%) happened during pregnancy. For individuals who had an acute myocardial infarction, the mean age was 33 years; for those who did not, it was 27 years. Women 40 years of age and above had a 30-fold increased risk of acute myocardial infarction compared to women under 20. This indicates that AMA is associated with an increased risk of acute myocardial infarction and, moreover, that older pregnant women should be monitored throughout and after their pregnancies. In order to reduce the risk of high- or total-spinal anesthesia (unintentional intrathecal injection) or local anesthetic systemic toxicity (unintentional intravascular injection), modern neuraxial analgesia favors the initiation and maintenance of analgesia with low-dose local anesthesia and opioid solutions [87]. Additionally, these low-dose approaches reduce placental drug transfer and hemodynamic effects [88]. Local anesthetics diluted lower the chance of severe hypotension. Significant visceral and somatic analgesia can be achieved by combining a local anesthetic with a lipid-soluble opioid. Because opioid and local anesthetic treatments work well together, their dosages can be reduced, which reduces side effects [35].
- CONCLUSION
Over the past few decades, older mothers have become pregnant at an increased rate. Worldwide, the number of women delaying delivery for various reasons is rising. Advanced maternal age increases the likelihood of unfavorable cardiovascular outcomes during pregnancy. With a high case fatality rate, cardiovascular illness is an uncommon cause of severe maternal morbidity, particularly in cases of aortic dissection. The majority of cardiac conditions that arise during pregnancy, birth, or puberty affect women who do not already have a cardiac condition. The information in this study will help raise awareness of the prevalence of severe maternal morbidity from cardiovascular disease, which will enable timely referral of women who are at risk and appropriate risk assessment. However, some studies came to the conclusion that there is no solid medical justification for discouraging very advanced maternal age (50–65 years) women from trying to conceive based only on their age, since healthy women who have been screened to rule out pre-existing disease tend to do well even at this advanced age. Pregnancy-related cardiovascular disease necessitates early disease detection, ideally prior to conception, as well as ongoing, risk-appropriate specialized care and monitoring during the condition. Pregnant women who already have cardiac disease should be referred to a specialized center for preconceptional counsel, to optimize their preconception health, and to remain within their area of care during their pregnancy.
REFERENCES
- Jackson, S.; Hong, C.; Wang, E.T.; Alexander, C.; Gregory, K.D.; Pisarska, M.D. Pregnancy outcomes in very advanced maternal age pregnancies: The impact of assisted reproductive technology. Fertil. Steril. 2015, 103, 76–80.
- Le Ray, C.; Scherier, S.; Anselem, O.; Marszalek, A.; Tsatsaris, V.; Cabrol, D.; Goffinet, F. Association between oocyte donation and maternal and perinatal outcomes in women aged 43 years or older. Hum. Reprod. 2012, 27, 896–901.
- Sauer, M.V. Reproduction at an advanced maternal age and maternal Health. Fertil. Steril. 2015, 103, 1136–1143.
- Manisha Gupta, Ramcharan Singh & Mahrukh Asghar (2023). Frequency of Neck & Arm Pain in Professionals Associated With Posture & Ergonomics. Dinkum Journal of Medical Innovations, 2(10):376-385.
- Javaria Arif, Muhammad Anwar Awan, Muhammad Suhail Sarwar, Asad Aslam Khan & Kabir Hussain (2023). Optometric Criteria of Prescription in Case of Borderline Refractive Errors. Dinkum Journal of Medical Innovations, 2(10):386-393.
- Kamal Anwar (2023). Comparison of Objective Refraction in Darkness with Cycloplegic Refraction. Dinkum Journal of Medical Innovations, 2(10):394-401.
- Sana Jamil, Sidra Anwar, Muhammad Anwar Awan, Sania Alam & Kamal Anwar (2023). Comparison of Measurement Techniques of Amplitude of Accommodation in Young Adults. Dinkum Journal of Medical Innovations, 2(10):370-375.
- Shamiul Bashir Plabon & Joya Mondol (2023). Nutritional Knowledge and Attitude towards Micronutrient Deficiency Disease among Selected Households in Dhaka City, Bangladesh. Dinkum Journal of Medical Innovations, 2(10):402-410.
- Shamiul Bashir Plabon & Shuvo Horel (2023). Prevalence of Micronutrients Deficiency Diseases and its Improvement Practices in Population of Mohammadpur, Dhaka, Bangladesh. Dinkum Journal of Medical Innovations, 2(10):411-417.
- Jamal Ahammed, Ferdous Alam, Al Rezowan Shoron, Md. Amir Hamja Niloy, Sumitro Das, Biswajit Kumar Utpal & Sumon Chandraw Roy (2023). A Review on Flavonoids in Neuropathic Pain. Dinkum Journal of Medical Innovations, 2(10):452-465.
- Mahrukh Asghar, Ashfaq Ahmad, Waqar Afzal, Umber Nawaz, Aqeel Saeed & Iqra Rasheed (2023). Effectiveness of Routine Physical Therapy with and Without Core Stability Exercises in Patients with Rotator Cuff Tendinopathy. Dinkum Journal of Medical Innovations, 2(10):443-451.
- Samrat Upadhya, Prachi Upadhya & Syeda Hajra Batool (2023). Perinatal Mortality Rate in South-Asian Countries: A Systematic Review. Dinkum Journal of Medical Innovations, 2(10):426-442.
- Prabin Acharya & Prachi Bhattarai (2023). Perinatal Mortality Rate in South-Asian Countries: A Systematic Review. Dinkum Journal of Medical Innovations, 2(10):418-425.
- Thomson, E.; Lappegard, T.; Carlson, M.; Evans, A.; Gray, E. Childbearing across partnerships in Australia, the United States, Norway, and Sweden. Demography 2014, 51, 485–508.
- Hage, F.G.; Mansur, S.J.; Xing, D.; Oparil, S. Hypertension in women. Kidney Int. Suppl. 2013, 3, 352–356.
- Yogev, Y.; Melamed, N.; Bardin, R.; Tenenbaum-Gavish, K.; Ben-Shitrit, G.; Ben-Haroush, A. Pregnancy outcome at extremely advanced maternal age. Am. J. Obstet. Gynecol. 2010, 203, 558.
- Khalil, A.; Syngelaki, A.; Maiz, N.; Zinevich, Y.; Nicolaides, K.H. Maternal age and adverse pregnancy outcome: A cohort study. Ultrasound Obstet. Gynecol. 2013, 42, 634–643.
- Alshami, H.A.; Kadasne, A.R.; Khalfan, M.; Iqbal, S.Z.; Mirghani, H.M. Pregnancy outcome in late maternal age in a high-income developing country. Arch. Gynecol. Obstet. 2011, 284, 1113–1116.
- Carolan, M.C.; Davey, M.A.; Biro, M.; Kealy, M. Very advanced maternal age and morbidity in Victoria, Australia: A population based study. BMC Pregnancy Childbirth 2013, 13, 80.
- Balayla, J.; Azoulay, L.; Assayag, J.; Benjamin, A.; Abenhaim, H.A. Effect of maternal age on the risk of stillbirth: A population-based cohort study on 37 million births in the United States. Am. J. Perinatol. 2011, 28, 643–650.
- Wu, Y.; Chen, Y.; Shen, M.; Guo, Y.; Wen, S.W.; Lanes, A.; White, R.R.; Adanlawo, A.; Walker, M.; Hua, X. Adverse maternal and neonatal outcomes among singleton pregnancies in women of very advanced maternal age: A retrospective cohort study. BMC Pregnancy Childbirth 2019, 19, 3.
- Ogawa, K.; Urayama, K.Y.; Tanigaki, S.; Sago, H.; Sato, S.; Saito, S.; Morisaki, N. Association between very advanced maternal age and adverse pregnancy outcomes: A cross sectional Japanese study. BMC Pregnancy Childbirth 2017, 17, 349.
- Tseng, K.T.; Peng, C.C.; Chang, J.H. The impact of advanced maternal age on the outcomes of very low birth weight preterm infants. Medicine 2019, 98, 14336.
- Kahveci, B.; Melekoglu, R.; Evruke, I.C.; Cetin, C. The effect of advanced maternal age on perinatal outcomes in nulliparous singleton pregnancies. BMC Pregnancy Childbirth 2018, 18, 343.
- Carolan, M. Maternal age ≥45 years and maternal and perinatal outcomes: A review of the evidence. Midwifery 2013, 29, 479–489.
- Huisman, C.M.; Zwart, J.J.; Roos-Hesselink, J.W.; Duvekot, J.J.; van Roosmalen, J. Incidence and Predictors of Maternal Cardiovascular Mortality and Severe Morbidity in the Netherlands: A Prospective Cohort Study. PLoS ONE 2013, 8, e56494.
- James, A.H.; Jamison, M.G.; Biswas, M.S.; Brancazio, L.R.; Swamy, G.K.; Myers, E.R. Acute Myocardial Infarction in Pregnancy A United States Population-Based Study. Circulation 2006, 113, 1564–1571.
- Vaidya, V.R.; Arora, S.; Patel, N.; Agnihotri, K.; Billimoria, Z.; Turakhia, M.P.; Friedman, P.A.; Madhavan, M.; Kapa, S.; Noseworthy, P.A.; et al. Burden of arrhythmia in pregnancy. Circulation 2017, 135, 619–621.
- Li, J.M.; Nguyen, C.; Joglar, J.A.; Hamdan, M.H.; Page, R.L. Frequency and Outcome of Arrhythmias Complicating Admission During Pregnancy: Experience From a High-volume and Ethnically-diverse Obstetric Service. Clin. Cardiol. 2008, 31, 538–541.
- Kolte, D.; Khera, S.; Aronow, W.S.; Palaniswamy, C.; Mujib, M.; Ahn, C.; Jain, D.; Gass, A.; Ahmed, A.; Panza, J.A.; et al. Temporal Trends in Incidence and Outcomes of Peripartum Cardiomyopathy in the United States: A Nationwide Population-Based Study. J. Am. Heart Assoc. 2014, 3, e001056.
- Breart, G.; Barros, H.; Wagener, Y.; Prati, S. Characteristics of the childbearing population in Europe. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, S45–S52.
- Martin, J.A.; Hamilton, B.E.; Ventura, S.J.; Osterman, M.J.; Mathews, T.J. Births: Final data for 2011. Natl. Vital. Stat. Rep. 2013, 62, 1–69.
- Mathews, T.J.; Hamilton, B.E. Mean age of mother, 1970–2000. Natl. Vital. Stat. Rep. 2002, 51, 1–14.
- Mathews, T.J.; Hamilton, B.E. Mean age of mothers is on the rise: United States, 2000–2014. NCHS Data Brief 2016, 232, 1–8.
- Report on Fertilization and Embryo Transfer in 2017. Available online: http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai15/dl/h3-4.pdf (accessed on 3 April 2019).
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.K. Births: Provisional data for 2016. Vital Statistics Rapid Release, No. 2; National Center for Health Statistics: Hyattsville, MD, USA, 2017. Available online: https://www.cdc.gov/nchs/data/vsrr/report002.pdf (accessed on 3 April 2019).
- Saftlas, A.F.; Olson, D.R.; Franks, A.L.; Atrash, H.K.; Pokras, R. Epidemiology of preeclampsia and eclampsia in the United States, 1979–1986. Am. J. Obstet. Gynecol. 1990, 163, 460–465.
- Poon, L.C.; Kametas, N.A.; Chelemen, T.; Leal, A.; Nicolaides, K.H. Maternal risk factors for hypertensive disorders in pregnancy: A multivariate approach. J. Hum. Hypertens. 2010, 24, 104–110.
- Arya, S.; Mulla, Z.D.; Plavsic, S.K. Outcomes of women delivering at very advanced maternal Age. J. Womens Health 2018, 27, 1378–1384.
- Duckitt, K.; Harrington, D. Risk factors for pre-eclampsia at antenatal booking: Systematic review of controlled studies. BMJ 2005, 330, 565.
- Bianco, A.; Stone, J.; Lynch, L.; Lapinski, R.; Berkowitz, G.; Berkowitz, R.L. Pregnancy outcome at age 40 and older. Obstet. Gynecol. 1996, 87, 917–922.
- Dulitzki, M.; Soriano, D.; Schiff, E.; Chetrit, A.; Mashiach, S.; Seidman, D.S. Effect of very advanced maternal age on pregnancy outcome and rate of cesarean delivery. Obstet. Gynecol. 1998, 92, 935–939.
- Sheen, J.J.; Wright, J.D.; Goffman, D.; Kern-Goldberger, A.R.; Booker, W.; Siddiq, Z.; D’Alton, M.E.; Friedman, A.M. Maternal age and risk for adverse outcomes. Am. J. Obstet. Gynecol. 2018, 219, 390.
Publication History
Submitted: October 05, 2023
Accepted: October 20, 2023
Published: November 01, 2023
Identification
D-0196
Citation
Jamil Raza & Sidra Anwar (2023). Cardiovascular Findings in Women Delivered At Advanced Maternal Age. Dinkum Journal of Medical Innovations, 2(11):466-472.
Copyright
© 2023 DJMI. All rights reserved