

")
Publication History
Submitted: October 17, 2023
Accepted: October 10, 2023
Published: January 31, 2024
Identification
D-0240
DOI
https://doi.org/10.71017/djmi.3.1.d-0240
Citation
Dr. Md. Salah Uddin (2024). Correlation between Duration of Preoperative Motor Deficit and Early Postoperative Motor Functional Recovery in Patients with Intradural Extramedullary Spinal Tumor. Dinkum Journal of Medical Innovations, 3(01):52-63.
Copyright
© 2024 The Author(s).
52-63
Correlation between Duration of Preoperative Motor Deficit and Early Postoperative Motor Functional Recovery in Patients with Intradural Extramedullary Spinal TumorOriginal Article
Dr. Md. Salah Uddin 1 *
- Department of Neurosurgery, Dhaka Medical College and Hospital, BSMMU, Dhaka, Bangladesh.
* Correspondence: dr.babu87@gmail.com
Abstract: Intradural extramedullary (IDEM) spinal tumors are generally benign neoplasms that occur within the dura mater but outside the spinal cord substance and usually treated with surgical excision. Symptoms of these tumors may varies with duration. This study denoted correlation between duration of preoperative motor deficit and early postoperative motor functional recovery that will help eventually to do more accurate assessment, counselling of the patients about surgical outcome and prognosis of IDEM spinal tumors. This prospective interventional study was carried out in the department of Neurosurgery, Dhaka Medical College and Hospital. A total N=49 patients of IDEM spinal tumor were included after taking informed written consent. A detailed history and thorough neurological examination were carried out. Pre and postoperative neurological function and motor deficit were evaluated by Modified Medical Research Council system (MRC) muscle grading. Follow-up was done at 30th postoperative day (POD). Data were collected and analyzed by SPSS – 24. Correlation between duration of preoperative motor symptoms and postoperative MRC grading was determined using Spearman’s rank correlation coefficient. Mean age of the patiesants was 41 ± 14.08 years with male predominance (55.1%). Schwannoma was the commonest tumor (42.8%). The commonest location was dorsal spine (46.9%). Pain was present in all (100%) patients, motor weakness in (97.9%), tingling/numbness in (69.4%), sphincter disturbance in 21 patients (42.9%). The mean duration of preoperative disease symptoms was 9.79 ± 7.46 months. According to MRC motor power grade, majority (83.7%) had improved at 30th postoperative day. Median (IQR) value of MRC motor power grade at 30th postoperative day was increased to 4(3-5) from preoperative grade 3(1-3). Spearman correlation model showed that duration of preoperative motor deficit had significant negative correlation with motor functional recovery at 30th POD (rs= -0.733, p <0.001). Preoperative duration of motor deficit and early postoperative motor functional recovery is significantly interrelated in patients with IDEM spinal tumors.
Keywords: preoperative motor deficit, spinal tumor, Bangladesh
- INTRODUCTION
Spinal tumors are classified as either extradural or intradural in relation to the spinal dura mater. Intradural tumors can be further sub-categorized into extramedullary (IDEM) or intramedullary spinal cord tumors (IMSCT) [1]. Intradural extramedullary (IDEM) tumors are generally benign neoplasms that occur within the dura mater but outside the spinal cord, accounting for about two thirds of primary spinal tumors. These tumors consist of almost 70% of all intradural lesions and the most frequent types are nerve sheath tumors, meningiomas and myxopapillary ependymomas. Other less common tumors include hemangiopericytomas, lipomas, paragangliomas and inclusion cysts such as dermoid and epidermoid cysts [2]. Surgery is considered the only valuable treatment for this condition and aims to get a successful resection while minimizing the risk of spinal cord damage and the postoperative morbidity [3]. IDEM spinal tumors that are anteriorly located in the upper thoracic spine were found to have the highest rate of surgery related complications and postoperative neurological deficits. This finding may be associated with a higher cord-to-canal ratio and a tenuous vascular supply in this region [4]. The choice of treatment in patients with intradural extramedullary spinal tumor is open microsurgical approach to establish a histopathlogical diagnosis and to decompress the neural structures [5]. Recovery potential from sensory and motor deficit appears to be the most prominent matter after surgery. Total laminectomy may cause spinal instability and kyphosis due to the damage to the musculo-ligamentous structures and posterior bony elements. These complications may produce neurologic symptoms by compressing the spinal cord or nerve roots. Most IDEM spinal tumors are benign and they exhibit no specific symptoms except local pain or radicular pain. Radicular pain and worsening sensory and motor loss are common manifestations [6]. Many patients can experience residual focal deficits, which may not be completely disabling. Postoperative worsened neurologic function may show paraplegia with loss of bladder and bowel control [7]. Duration of preoperative motor deficit has significance in the treatment outcome. Diagnostic tools like MRI scan, the advancement of surgical instrumentation and microsurgical techniques have improved the surgical outcome in IDEM spinal tumors. Nevertheless, IDEM spinal tumor are difficult to detect in early stage. These tumors lack obvious clinical symptoms until compression or neurological deficit occurs [8]. However, a delay in surgical removal can lead to permanent neurological deficits and long term outcomes. In consequence, gross total resection can be achieved thus, resulting is a good overall functional recovery of the patient. Therefore, this study was designed to find out any relationship between duration of preoperative motor deficit and early postoperative motor functional recovery in patients with IDEM spinal tumor [9]. IDEM spinal tumors are the most common primary spinal tumors, usually benign and slow growing. The vast majority of these lesions are one of three types: schwannoma, meningioma or neurofibroma. Symptoms may varies with duration according to their location of origin and nature of the tumors. Early detection of these tumor with availability of advanced technique such as CT/MRI scan greatly increases the chances for successful recovery by prompt intervention [10]. The different studies of developed countries observed that, increase the preoperative duration of disease symptoms had delay the functional recovery of the patients postoperatively [11]. The study found out the correlation between duration of preoperative motor deficit and early postoperative motor functional recovery that will help eventually to do more accurate assessment, prompt surgical intervention, counselling of the patients about surgical outcome and prognosis of IDEM spinal tumors. It also helped to understand the current situation in hospital facility to determine a guideline for management of such cases to reduce morbidity. A small portion of intradural tumours are both intra and extramedullary and usually occur at the conus medullaris transition site to filum terminale or nerve root entry zone. Neurofibromas and Schwannomas. In both sexes, nerve sheath tumours are most common in the fourth and fifth decades. Neurofibromatosis type 2 can have schwannomas, the more common subtype. More common dorsal or ventral nerve rootlets can cause spinal NSTs. These tumours may be intradural or extradural, especially in the cervical region. Dumbbell-shaped patterns can contain intra- and extradural components. Schwannomas can be compact with palisading verocay bodies (Antoni A) or less cellular (Antoni B) [12]. Neurofibromas are most common in neurofibromatosis type 2 but can occur occasionally. These tumours can involve many nerve fascicles and enlarge the nerve, making it difficult to remove without surrendering the nerve of origin, unlike schwannomas. Gross pathology with axons can identify these lesions from schwannomas [13]. Most intradural tumours, meningiomas, afflict the thoracic area. The most common histologic subtype is psammomatous, which mimics intracranial variants with many psammoma bodies. Meningiomas attack elderly adults between 50 and 70, 3–4:1 female to male [14]. Myxopapillary ependymoma: Well-capsulated tumours reaching 36 years old with a little male predominance. Histologic smears indicate myxopapillary vascularized myxoid cores surrounding by well-differentiated cuboidal or columnar cells orientated radially [15]. IDEM spinal tumours, which make up 60% of spinal canal tumours, two-thirds of primary spinal tumours, and 15% of central nervous system tumours, are benign neoplasms that arise in the dura mater but not the spinal cord. These patients are 90% over 20. The majority of spinal tumours are extradural (50-55%), whereas 40-45% are intradural extramedullary and 5% are intramedullary [16]. IDEM spinal tumours grow slowly, therefore symptoms may not appear for a long time. Only axial back discomfort may occur, radicular discomfort is another sign of nerve sheath tumours. Compression of the spinal cord can induce myelopathy, Cauda equina spinal tumours do not show symptoms early, and the usual diagnosis time is 12 months [17]. The symptoms are the same for intramedullary and extramedullary lesions. They cause pain syndromes, neurological symptoms, motor and sensory impairment, sphincter disruption, or a combination. Pain is the most common initial symptom and can be local, nocturnal, or extend to an arm, chest, or leg [18]. IDEM tumours cause radicular discomfort, motor weakness, and sphincter disruption in 72%, 60%, and 33% of patients. Due to preoperative neurologic abnormalities, IDEM results correlate with surgical resection, and surveillance can cause lasting neurologic damage [19]. Surgical resection aims to diagnose tissue, remove tumours, and improve neurologic function. Intraoperative somatosensory and motor evoked potentials evaluate neuronal function and functional outcome. Fewer preoperative impairments improve long-term outcomes. The thoracic spine (58.06%) had the most IDEM tumours, followed by the lumbar (25.80%), cervical (3.22%), and mixed junctional (12.90%). Histopathology revealed schwannomas-51.61%, meningiomas-35.48%, lipomas-6.45%, hemangiomas-3.22%, and ependymomas-3.22% [20]. The mean symptom duration was 11.56 months, and 61.29% had motor weakness. In all 19 neurologically affected cases, performance scale and muscle strength improved after surgery. The mean performance score was 56.45 ± 8.77 pre-operatively and 59.68 ± 10.48 post-discharge. A study examined 35 IDEM tumour removal patients’ results. Patients had 6 neurofibromas, 12 schwannomas, 9 meningomas, 3 ependymomas, and 1 paraganglioma, common symptoms were limb weakness, sphincter dysfunction, and paraplegia. Mean symptom duration was 6.4 months. In this series, 77.14% had good Frankel score functional outcomes [21]. Nurick’s score mean values decreased significantly throughout 1 week and 1 month. IDEM surgical results are good with occasional outliers. Greater canal occupancy and longer symptom duration usually lead to poor functional outcomes [22]. Examined IDEM spinal cord tumour surgery outcomes, histopathology showed 58.33% schwannomas, 23.33% meningiomas, 6.67% neurofibromas, 5% arachnoid cysts, and 5% myxopapillary ependymomas [23]. Surgery can cause neurological abnormalities and problems, the study covered 221 patients. Fifty-three neurofibromas, 163 schwannomas, and 5 malignant peripheral nerve sheath tumours. A 32% rate of 70 problems occurred in 221 patients. Twelve were new or increasing motor impairments. Symptoms lasted 0-120 months. Given the proximity of nerve sheath tumours to functional neural parts, surgical result is likely a problem. It is crucial to study the relationship between preoperative motor deficit duration and early postoperative motor functional recovery in IDEM spinal tumour patients [24].
- MATERIALS AND METHODS
The study follow the prospective interventional study design, population of the study was patients with intradural extramedullary spinal tumor who were admitted in the department of Neurosurgery, Dhaka Medical College Hospital for surgical treatment.
The sample size of this study was determined by following equation
Formula of sample size calculation:
![]()
Here,
n = sample size
z = 1.96
p = Prevalence: 16%=0.16 (Alam et al. 2020).
q = 1- p =1-0.16 = 0.84
d = allowable error: 10% (0.1)
Total study subjects (n)
![]()
= 1.962×0.16×0.84/ (0.1)2
= 51.63
However, finally 52 patients were included for this study.
A total number of N=52 patients were finally included, purposive sampling technique has been used to collected primary data. A structured questionnaire was completed by all participating patients with the help of their relatives to obtain information on demographic characteristics like age, gender, marital status, education, family details, socioeconomic level etc. and duration of having the symptoms and co-morbidities. The duration of preoperative disease includes also the waiting period in hospital after admission to surgery. After admission, the location and extent of the tumor was determined by magnetic resonance imaging (MRI) scan of concerning regions of spine. Different sequences of MRI shows signal characteristics and denotes the relationship of the mass to the cord, dura and nerve roots. Dural involvement with dural tail sign and homogenous contrast enhancement are the typical feature of meningioma. Dumbbell shaped, marked hyperintensity in T2 weighted image, heterogeneous contrast uptake and displace the nerve roots are found in schwannoma but similar feature with encasement of nerve roots are present in neurofibroma. In case of intradural lipoma, fat signal intensity found on MRI. Cerebrospinal fluid signal intensity without restricted diffusion in case of spinal arachnoid cyst. All Patients’ muscle bulk, muscle tone, muscle power and jerks were evaluated. Muscle bulk was expressed as normal/diminished/increased. Muscle tone was elicited and expressed as normal/increased/reduced. Muscle strength was scored according to the modified Medical Research Council system (MRC) muscle grading from 0 to 5 where grade 0 means complete paralysis and grade 5 means normal muscle power. Also different jerks were assessed to find out the extension of the impact of the tumor. All the assessment were done and analyzed accordingly. Pre and postoperative neurological function, motor deficit was evaluated by modified Medical Research Council system (MRC) muscle grading. Standard procedures were maintained during and after operation. Patients were evaluated on the 30th POD to follow-up for early postoperative motor functional recovery. The procedure was performed by experienced Neurosurgeon. Posterior decompression of the neural elements by laminectomy or hemilaminectomy under X-ray guidance, gross total removal of spinal tumor was performed by microsurgical technique and followed by posterior stabilization if needed. Then the excised tumor tissue was sent for histopathology. Patients were discharged about one week after the operation. Postoperative motor functional recovery of the patient was evaluated using MRC muscle grading scale. All collected information were stored in separate data record form. After data checking, these were inputted into Microsoft excel sheet (version 2013) and then transcribed into statistical software. Finally, after data editing and compilation, data were analyzed by SPSS version 24. After collection of all the required data, data were checked, verified for consistency and tabulated using the SPSS 24 software. Exploratory data analysis was carried out to describe the study population. Statistical significance was set as 95% confidence level. Frequency and percentage were used to express categorical variables. Mean and standard deviation were used to express continuous variables. For skewed data, non-parametric test (Friedman’s two-way test) was used for analyzing related continuous variables. Correlation between duration of motor symptoms and postoperative MRC grading was determined using Spearman’s rank correlation coefficient. For all statistical tests, p -value less than 0.05 was considered as statistically significant.
- RESULTS AND DISCUSSION
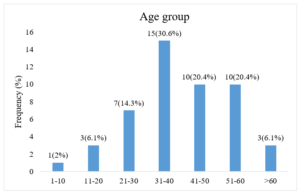
Figure 01: Distribution of the study patients by age (n=49)
Mean age of all patients was 41 ± 14.08 years. Maximum age was 80 years and minimum age was 6 years. About one third (30.6%) of the patients were between 31 to 40 years of age. It was observed that more than half of patients were male (55.1%) and rest were female (44.9%).
Table 01: Distribution of the study patients by clinical presentations (n=49)
| Clinical presentation | Frequency (f) | Percentage (%) |
| Back pain | 41 | 83.7 |
| Neck pain | 8 | 16.3 |
| Paraparesis/Paraplegia | 42 | 85.7 |
| Quadriparesis/Quadriplegia
Tingling/Numbness |
7
35 |
14.2
71.4 |
| Sphincter disturbance | 21 | 42.9 |
Most of the patients had multiple clinical presentations. Among them 42(85.7%) patients had paraparesis or paraplegia, 41(83.7%) back pain, 35(71.4%) patients had tingling or numbness, 21(42.9%) patients had sphincter disturbance.
Table 02: Distribution of the study patients by location of the tumor (n=49)
| Location of the tumor | Frequency (f) | Percentage (%) |
| Cervical | 7 | 14.3 |
| Cervico-dorsal | 2 | 4.1 |
| Dorsal | 23 | 46.9 |
| Dorso-lumbar | 4 | 8.2 |
| Lumbar | 13 | 26.5 |
According to the location, about half of the tumors were dorsal (46.9%), followed by lumbar vertebra (26.5%), cervical (14.3%), dorso-lumbar (8.2%) and cervico-dorsal (4.1%).
Table 03: Distribution of the study patients by duration of preoperative motor deficit (n=49)
| Duration | Frequency (f) | Percentage (%) |
| ≤ 6 months | 25 | 51.1 |
| > 6 months | 24 | 48.9 |
According to duration of disease, about half of the patients had less than or equal of 6 months preoperative disease symptoms (51.1%), while more than 6 months disease duration was present in 48.9% of patients. The mean duration of pre-operative disease symptoms was 9.79 ± 7.46 months.
Table 04: Distribution of the study patients regarding histopathological type of tumor (n=49)
| Histopathological type of tumor | Frequency (f) | Percentage (%) |
| Schwannoma | 21 | 42.8 |
| Meningioma | 16 | 32.7 |
| Myxopapillary ependymoma | 5 | 10.2 |
| Neurofibroma | 4 | 8.2 |
| Arachnoid cyst | 2 | 4.1 |
| Lipoma | 1 | 2 |
Schwannoma formed the largest histopathological group with 21 (42.8%) patients, followed by sixteen (32.7%) patients of meningiomas, and the third most common group of five (10.2%) patients with myxopapillary ependymomas. According to other cell type, 4(8.2%) patient had neurofibroma, 2(4.1%) patients had arachnoid cyst and 1(2%) patient had lipoma.
Table 05: Distribution of study patients according to preoperative and early postoperative MRC motor function grade (n=49)
| MRC grade | Preoperative
f (%) |
30th postoperative day
f (%) |
| 0 | 10 (20.4) | 1 (2) |
| 1 | 3 (6.1) | 1 (2) |
| 2 | 11 (22.4) | 7 (14.3) |
| 3 | 15 (30.6) | 5 (10.2) |
| 4 | 10 (20.4) | 15 (30.6) |
| 5 | 0 | 20 (40.8) |
Preoperatively, 15(30.6%) patients were in grade 3, 11(22.4%) in grade 2, 10(20.4%) patients in both grade 0 and 4, 3(6.1%) patients in grade 1, but no patients were in grade 5. Follow-up at 30th postoperative day, most of the patients 20(40.8%) were in grade 5, 15(30.6%) patients in grade 4, 7(14.3%) in grade 2, 15(30.6%) patients in grade 4, 5(10.2%) in grade 3, 1(2%) patients in each grade 1 and grade 0.
Table 06: Distribution of the study patients regarding improvement of disease condition on the 30th postoperative day (n=49)
| Frequency (f) | Percentage (%) | |
| Stable | 7 | 14.2 |
| Improvement | 41 | 83.7 |
| Deteriorated | 1 | 2.1 |
According to MRC motor power grade, at 30th postoperative day, majority of the patients were improved (83.7%) from pre-operative condition, though, 14.2% were similar as preoperative and only 2.1% were deteriorated.
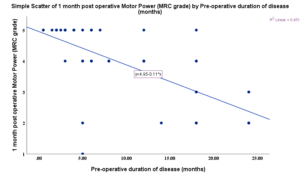
Figure 02: Relationship between duration of preoperative motor deficit and early postoperative motor functional recovery at 30th postoperative day (n=49)
Spearman correlation model showed that increased duration of motor deficit had decreased early post-operative motor power (rs= -0.733, p value <0.001).
Table 07: Clinical improvement by MRC grade (n=49)
| Grade | Median (IQR) | p value |
| MRC motor power grade | ||
| Preoperative | 3 (1-3) | |
| At 30th postoperative day | 4 (3-5) | <0.001** |
Values are expressed as median (IQR) over column in total
p value was determined by **Friedman’s two-way test compared with preoperative score/grades.
Median value of MRC motor power grade of preoperative and 30th postoperative day were statistically significant.
Table 08: Distribution of the study patients regarding postoperative complications (n=49)
| Complications | Frequency (f) | Percentage (%) |
| Surgical site infection | 4 | 8.1 |
| CSF leak | 3 | 6.1 |
| Urinary tract infection | 2 | 4.1 |
| Pressure sore | 2 | 4.1 |
| No complications | 38 | 77.6 |
Table shows distribution of study patients regarding postoperative complications. It was observed that majority of the patients (77.6%) did not presented with postoperative complications. However, surgical site infection was most common complications (8.1%) followed by postoperative CSF leakage (6.1%), urinary tract infection (4.1%) and pressure sore (4.1%).
3.1 Discussion
Spinal tumors that are intradural and extramedullary are typically benign tumors. Meningioma, neurofibroma, and schwannoma are the most common kinds. Hemangiopericytomas, lipomas, paragangliomas, and inclusion cysts such dermoid and epidermoid cysts are among the other less frequent cancers [25]. Depending on the origin location and type of tumor, symptoms can vary in length. By using modern techniques like CT/MRI scans and accurate neurological assessment, early tumor discovery dramatically increases the chances of a full recovery through timely intervention [26]. This study comprised a total of 49 patients with IDEM spinal tumors of any age or gender who had surgery at the Dhaka Medical College and Hospital’s Neurosurgery department between January 2021 and June 2022. Using Spearman’s correlation model, we found that patients with longer duration of preoperative motor symptoms to surgical intervention had lower motor power at 30 days postoperatively (rs = -0.733, p value < 0.001) [21]. Similar findings about the recovery of motor function revealed that three of five paraplegic patients who underwent surgery after 29 days lost the capacity to walk at their first postoperative visit, while six out of seven paraplegic patients who underwent surgery within 29 days were able to walk at that time. When it came to clinical manifestations, the majority of patients had several. The majority of them showed up with sphincter dysfunctions, tingling or numbness, weakness in the limbs, and local pain [27]. Paraplegia (8.57%), sphincter dysfunction (42.9%), limb weakness (80%), and paresthesia (88.6%) were the most common symptoms. It found that spinal pain (89.6%) and motor deficiency (93.5%) were the most common presenting complaints, with sphincter abnormalities (29%), following. The mean length of preoperative disease symptoms was 9.79 ± 7.46 months, and approximately half of the patients (51.1%) had symptoms for less than or equal to six months [28]. The results of the MRI scan showed that the tumor was located in the dorsal spinal region (46.9%), followed by the lumbar (26.5%) and cervical (14.3%) regions, only 5.3% of tumors were cervical, 26.3% were lumbar, and 52.6% of tumors were dorsal. These findings were consistent with our research. Mehta et al. (2013), however, noted that the dorsal region was the most prevalent, occurring in 62.5% (n = 60) of the patients, and the cervical spine in 37.5% (n = 36) of the patients [29]. According to the histological type of tumor cell in this investigation, meningioma (32.7%) and schwannoma (42.8%) were the most common tumor pathologies. The most common tumors, which is in line with our findings, on the other hand, neurofibroma (21.05%), schwannoma (15.78%), and meningioma (63.15%) was the most prevalent type of tumor [30]. The average age of all patients in this study was 41 ± 14.08 years, with a range of 6-80 years. Approximately one-third (30.6%) of the patients were in the 31–40 year age range. Furthermore noted was the fact that 55.1% of the patients were men, infection at the surgical site accounted for 8.1% of all complications among the patients, with CSF leak coming in second at 6.1% [31]. Nonetheless, 77.6% of the participants that did not present with postoperative problems. In line with our findings, Kobayashi et al. (2021) found that postoperative CSF leakage was the most frequent complication, occurring in 2.6% (n=3) of patients. Patients with IDEM spinal tumors experience a significant surgical recovery of motor function depending on the length of their preoperative motor deficit.
- CONCLUSIONS
This study evaluated the duration of preoperative motor deficit had significant negative correlation with postoperative motor functional recovery at 30th postoperative day. Hence it can be concluded that preoperative duration of symptom and postoperative clinical outcome is interrelated in IDEM spinal tumors. Intradural extramedullary spinal tumor are usually benign tumor. Early diagnosis with the help of advanced technique (CT scan, MRI scan) following early intervention leads to better clinical outcome Patients with intradural extra-medullary spinal tumors should be operated without any delay for better early post-operative outcome. Further multicenter study with larger sample size and longer follows up is recommended.
REFERENCES
- Dauleac, C., Boulogne, S., Barrey, C. Y., Guyotat, J., Jouanneau, E., Mertens, P., … & André-Obadia, N. (2022). Predictors of functional outcome after spinal cord surgery: relevance of intraoperative neurophysiological monitoring combined with preoperative neurophysiological and MRI assessments. Neurophysiologie Clinique, 52(3), 242-251.
- Panchariya, P., Jain, V. K., Goel, A., & Gupta, S. (2022). ROLE OF PRE-OPERATIVE SSEP AS POST OPERATIVE OUTCOME INDICATOR IN INTRADURAL EXTRAMEDULLARY SPINE TUMOUR PATIENTS. Int J Acad Med Pharm, 4(5), 859-862.
- Warda Anam, Khadija Anum & Muhammad Anas (2023). Literature Review on Effectiveness of Mirror Therapy and Conventional Therapy in Patients with Stroke. Dinkum Journal of Medical Innovations, 2(07):240-248.
- Gazzeri, R., Telera, S., Galarza, M., Callovini, G. M., Isabella, S., & Alfieri, A. (2021). Surgical treatment of intramedullary spinal cord metastases: functional outcome and complications—a multicenter study. Neurosurgical Review, 1-9.
- Abhiraj, Steven, Darian, Jack, Tania, & Ankit. (2018). Surgical complications in intradural extramedullary spinal cord tumors-an ACS-NSQIP analysis of spinal cord level and malignancy. https://www.sciencedirect.com/science/article/pii/S1878875018312282
- Sarah Rehman, Saira Rana & Mehru-Nisa (2023). Knowledge, Influence of Factors, and Management Strategies among Family Members with Behavioral Conditions. Dinkum Journal of Medical Innovations, 2(03):79-84.
- Ankit, Owoicho, Isaac, Paul, Terence, Ulysses, Allan, Joseph, Carlos, & Robert. (2013). Anatomical location dictating major surgical complications for intradural extramedullary spinal tumors: a 10-year single-institutional experience. https://thejns.org/spine/view/journals/j-neurosurg-spine/19/6/article-p701.xml
- Anmol, Anurag, Shiteez, Jitendra, Bhawani, & Tshering. (2024). Functional outcomes in intradural extramedullary spinal tumors. https://surgicalneurologyint.com/wp-content/uploads/2024/04/12849/SNI-15-114.pdf
- (2009). Extramedullary intradural spinal tumors: a review of modern diagnostic and treatment options and a report of a series. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5655171/
- , A., N., A., J., A., & J. (1998). Intradural extramedullary spinal canal secondary neoplasms: MR findings in 30 patients. https://link.springer.com/article/10.1007/s003300050532
- David, Mark, & David. (2007). Part I: Spinal-cord neoplasms—intradural neoplasms. https://www.thelancet.com/journals/lanonc/article/PIIS1470-2045(06)71009-9/fulltext
- Rubab Rasheed & Manisha Nagpal (2023). Psychosocial issues in Parents and Patients with Thalassemia. Dinkum Journal of Medical Innovations, 2(05):188-193.
- Davide, Corrado, Antonio, Luisa, Rossella, Franco, & Franco. (2018). . . . neurophysiological monitoring for intradural extramedullary spinal tumors: predictive value and relevance of D-wave amplitude on surgical outcome during a 10-year . . .. https://thejns.org/spine/view/journals/j-neurosurg-spine/30/2/article-p259.xml
- Davide, Corrado, David, Rossella, Luisa, Francesco, & Franco. (2015). Intraoperative neurophysiological monitoring for intradural extramedullary tumors: why not? https://www.sciencedirect.com/science/article/pii/S0303846715000086
- Dhanish, Vivek, & Samir. (2021). Clinical outcome of intradural extramedullary spinal cord tumors: A single-center retrospective analytical study. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8088529/
- John Petter (2023). Anti-Depressant Consumption, Patterns, Prevalence, and Risk Considerations among Women in the Fertile Age Range. Dinkum Journal of Medical Innovations, 2(03):85-90.
- Frank, & Marc. (2011). Adult intradural primary spinal cord tumors. https://jnccn.org/view/journals/jnccn/9/4/article-p434.xml?rskey=rtmP8Y&result=2780&utm_source=TrendMD&utm_medium=cpc&utm_campaign=JNCCN_TrendMD_0
- Gaofeng, Li, Ye, Taihang, & Jingmin. (2014). Treatment results in the different surgery of intradural extramedullary tumor of 122 cases. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0111495
- Gerhard, & Rüdiger. (2001). Intradural and extradural spinal metastases. https://link.springer.com/article/10.1007/PL00011959
- , S., M., I., H., J., & S. (2017). Monitoring rate and predictability of intraoperative monitoring in patients with intradural extramedullary and epidural metastatic spinal tumors. https://www.nature.com/articles/sc201743
- Hoon-Seok, Dae-Jung, Kwan-Soo, Tae-Woo, & Soon-Youl. (2009). The surgical treatment for spinal intradural extramedullary tumors. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2766751/
- Jerome, Michael, & Harold. (1961). Differential diagnosis of intradural (extramedullary) and extradural spinal canal tumors. https://pubs.rsna.org/doi/abs/10.1148/76.5.718
- Sarah Gul Rehman & Deepak Singh (2023). Thalassemia Consequences and Survival Rates in South Asian Kids and Adults. Dinkum Journal of Medical Innovations, 2(05):194-200.
- Kelly, & Robert. (2019). Intradural extramedullary spinal neoplasms: radiologic-pathologic correlation. https://pubs.rsna.org/doi/abs/10.1148/rg.2019180200
- Kern, Lewis, Greg, & Kamran. (2011). Spinal intradural, extramedullary anaplastic ependymoma with an extradural component: case report and review of the literature. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3172008/
- Kunal, Khoi, Dean, & Praveen. (2015). Comparison of minimally invasive transspinous and open approaches for thoracolumbar intradural-extramedullary spinal tumors. https://thejns.org/focus/view/journals/neurosurg-focus/39/2/article-pE12.xml
- Marc, & Trent. (2011). Adult primary intradural spinal cord tumors: a review. https://link.springer.com/article/10.1007/S11910-011-0190-2
- Matthew, George, Sara, & James. (2016). Improved patient quality of life following intradural extramedullary spinal tumor resection. https://thejns.org/spine/view/journals/j-neurosurg-spine/25/5/article-p640.xml
- Mazda, Wilson, & Vedantam. (2015). Hemilaminectomy approach for intradural extramedullary spinal tumors: an analysis of 164 patients. https://thejns.org/focus/view/journals/neurosurg-focus/39/2/article-pE9.xml
- (2002). Spinal intradural extramedullary tumors: personal experience. https://search.proquest.com/openview/9f9b2777629e1085334adf26746d474f/1?pq-origsite=gscholar&cbl=49236
- Richard, Adrian, Johnny, & Martin. (2011). Safety and efficacy of intradural extramedullary spinal tumor removal using a minimally invasive approach. https://journals.lww.com/onsonline/fulltext/2011/03001/safety_and_efficacy_of_intradural_extramedullary.28.aspx
Publication History
Submitted: October 17, 2023
Accepted: October 10, 2023
Published: January 31, 2024
Identification
D-0240
DOI
https://doi.org/10.71017/djmi.3.1.d-0240
Citation
Dr. Md. Salah Uddin (2024). Correlation between Duration of Preoperative Motor Deficit and Early Postoperative Motor Functional Recovery in Patients with Intradural Extramedullary Spinal Tumor. Dinkum Journal of Medical Innovations, 3(01):52-63.
Copyright
© 2024 The Author(s).