

")
Publication History
Submitted: December 22, 2023
Accepted: January 14, 2024
Published: February 29, 2024
Identification
D-0248
DOI
https://doi.org/10.71017/djmi.3.2.d-0248
Citation
Dr. Sangam Pokharel, Dr. Rajesh Yadav, Dr. Anima Pradhan & Dr. Ashmita Paudel (2024). Comparative Study of Bupivacaine 0.5% and Ropivacaine 0.75% Epidurally In Lower Limb Orthopedic Surgeries. Dinkum Journal of Medical Innovations, 3(02):165-173.
Copyright
© 2024 DJMI. All rights reserved
165-173
Comparative Study of Bupivacaine 0.5% and Ropivacaine 0.75% Epidurally In Lower Limb Orthopedic SurgeriesOriginal Article
Dr. Sangam Pokharel 1 *, Dr.Rajesh Yadav 2, Dr Anima Pradhan 3, Dr.Ashmita Paudel 4
- Department of anaesthesia, College of Medical science, Kathmandu University, Nepal.
- Professor, department of anaesthesia, College of Medical science, Kathmandu University, Nepal.
- Department of anaesthesia, College of Medical science, Kathmandu University, Nepal.
- Department of anaesthesia, College of Medical science, Kathmandu University, Nepal.
* Correspondence: pokharelsangam1990@gmail.com
Abstract: The epidural blockade is becoming one of the most useful and versatile procedures in modern anesthesiology as it provides effective surgical anesthesia. In equal concentrations, the degree of motor blockade is less pronounced with Ropivacaine, and there is a greater propensity for blocking pain transmitting A-delta and C fibers rather than A-α motor fibers and an effective alternate to epidural Bupivacaine for major lower limb orthopedic surgery. This prospective, randomized, double blind study performed on N=60 patients of department of Anesthesiology, College of Medical Sciences-Teaching Hospital, Chitwan, Nepal. Patients were divided into Group R (Ropivacaine group) and Group B (Bupivacaine group). After premedication, patients were asked to maintain nil per oral status for at least for 8 hours. 30 patients of Group Ropivacaine received 15 mL of 0.75% Ropivacaine epidurally whereas 30 patients of group Bupivacaine received 15 mL of 0.5% Bupivacaine under full aseptic technique, after 16 G epidural needle inserted in L3-L4 interspace (midline approach), and introduction of 18G epidural catheter and test dose of 3ml 2% lignocaine with adrenaline 1:200,000, given in absence of signs of subarachnoid and intravascular injection. Onset and duration of sensory and motor blockade, maximum level of sensory blockade and motor blockade, hemodynamic changes were recorded in various time intervals throughout the surgeries less than or equal to 3 hours. The onset, duration and maximum level of sensory and motor blocks with hemodynamics observed at different time intervals of 0, 1, 3, 5, 10, 20, 30, 60, 90, 120, 150 and 180 minutes found that there was no significant difference between two groups in terms of onset of sensory block(p value- 1.00), duration of sensory block (p=0.85), maximal level (p=0.305) of sensory and onset of motor block (p=0.305), and maximum level of motor level (p=0.48), whereas we found statistically significant difference in duration of motor block (p< 0.005) which concluded Ropivacaine had shorter duration of motor block as compared to Bupivacaine which is taken as beneficial point for early mobilization in lower limb orthopedic surgeries.
Keywords: Ropivacaine, Bupivacaine, Epidural, Mean Blood Pressure, Heart Rate.
- INTRODUCTION
In today’s rapidly changing world, regional anesthesia has gained widespread acceptance among anesthesiologists worldwide. Epidural anesthesia is well-established as a safe and effective technique for both perioperative and postoperative analgesia. As a result, the search is always on for a drug that is safer, more effective, and less toxic, with an early recovery profile that allows for early ambulation [1]. Bupivacaine, introduced in 1965, was followed by reports of central nervous system and cardiovascular system toxicity, prompting restrictions on its use. This resulted in the development of newer pure agents with lower toxicity potential, such as ropivacaine and levobupivacaine [2]. Ropivacaine is a long-acting amide local anesthetic that is optically active and the pure S-enantiomer of propivacaine [3]. Ropivacaine has good hemodynamic stability, is less likely to cause cardiotoxicity and neurotoxicity, and has the highest margin of safety of any long-acting local anesthetic currently available [4]. The onset, quality, and duration of sensory block are nearly identical to bupivacaine. It has a lower lipid solubility, making it less likely to penetrate large, myelinated motor nerve fibers, and thus less prone to motor blockade [5]. Neuraxial anesthesia denotes all forms of central blocks, involving spinal and epidural spaces [6]. The epidural blockade is becoming one of the most useful procedure in modern anesthesiology as it provides effective surgical anesthesia and can meet the extended duration of surgical needs and prolongs postoperative analgesia, and reduces the incidence of hemodynamic changes as a result of the sympathetic blockade [7]. Bupivacaine and Ropivacaine controls pain at the nerve level by blocking the sodium channel by reversibly binding to receptors on the intracellular side of the membrane, while the sodium channel is inactive [8]. Bupivacaine being highly lipid soluble local anaesthetic, associated with cardiotoxicity when used in high concentration or when accidentally administered intravascularly [9]. Ropivacaine being fewer lipid soluble is associated with lower central nervous system and cardiotoxicity thus the recognition of acute life threatening cardiotoxicity of Bupivacaine led to the idea for study of drug comparable with Bupivacaine but with lower cardiotoxicity [10]. MLAC suggested Ropivacaine is 40% less potent than Bupivacaine so ideal to compare 0.5% bupivacaine with 0.75% Ropivacaine as the equipotent concentration for epidural anesthesia. A novel long-acting amide local anesthetic, ropivacaine shares structural similarities with other aminoamides, such as mepivacaine and bupivacaine [11]. Pure (S)-enantiomer is ropivacaine; the other two are racemic mixtures. The pharmacodynamic and pharmacokinetic profiles of ropivacaine are comparable to those of bupivacaine [12]. According to reports, the anesthetic’s overall clinical efficacy and the start and duration of sensory block are similar to those of bupivacaine. When used in equal concentrations, ropivacaine may cause less motor block than bupivacaine, though [13]. Primarily, ropivacaine is a pure S Bupivacaine’s (−) enantiomer renders it less detrimental to the cardiovascular and central nervous systems. For use in epidural anesthesia, ropivacaine is readily available in two strengths: 0.5% and 0.75%. 0.5% ropivacaine and 0.5% bupivacaine produced sensory block for cesarean sections that was equally effective [14]. The median duration of sensory block varied between 1.7–4.2 hours for ropivacaine and 1.8–4.4 hours for bupivacaine. Of the adverse effects, nausea affected 30% of patients receiving ropivacaine and 58% of those receiving bupivacaine [15]. Epidural ropivacaine (0.5%, 0.75%, and 1%) and 0.5% bupivacaine in patients undergoing hip surgeries and showed that 0.5% ropivacaine and 0.5% bupivacaine were indistinguishable with regard to sensory and motor blocking characteristics while 1% ropivacaine produced a longer duration of analgesia and more intense motor block than 0.5% bupivacaine [16]. However, many patients treated with 1% ropivacaine required treatment for hypotension and bradycardia. In comparison 0.5% ropivacaine and 0.5% bupivacaine for epidural anesthesia in 45 patients undergoing lower extremity surgery and showed that bupivacaine produced slightly longer duration of motor blockade than ropivacaine but did not find any statistical significant difference in the onset of analgesia or in highest sensory level achieved [17]. Ropivacaine has a greater propensity for blocking pain transmitting A-delta and C fibers rather than A-α motor fibers and appears to have most of the blocking characteristics of Bupivacaine. So, it is an effective alternate to epidural Bupivacaine for major lower limb orthopedic surgery [18].
- MATERIALS AND METHODS
The study followed the randomized, prospective, comparative interventional study design conducted in the department of Anesthesiology, College of Medical Sciences-Teaching Hospital, Chitwan, Nepal. The sample size was calculated by using the following formula
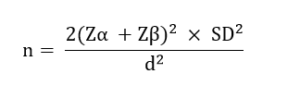
Where
n = Number of sample
Zα = 1.96 (at 95% confidence interval and power of 90%)
Zβ = 1.282 (at 95% confidence interval and power of 90%)
SD = Sum of standard deviation of the two groups which is 11.02 from previous study
d = Difference of mean between two groups which is 9
Following calculation based on previous published data, the sample size in each group came to be 31.2. Based on this result a decision to take 30 patients in each group was made. Randomization was done using closed envelope method, N=60 envelopes were prepared before start of study. Half of the envelopes contained receipt where Group R was written and the other half contained receipt where Group B was written. These envelopes were mixed and arranged randomly. The accompanying anesthesia assistant was trained regarding protocol of the study and was allowed to open the envelope before induction of anesthesia and prepare the drug as per the protocol and code the patient and give the drug to attending anesthesiologist of the OT to administer the drug at the time of anesthesia. Attending anesthesiologist did not know the drug being given. Data collection was done and decoding was done only during analysis of the collected data. The study included patients with ASA physical status class I and II, age between 18 – 71 years of either sex, BMI less than 30 kg/m2, lower limb routine orthopedic surgeries. Those patients with allergy to local anesthetics, local infections, coagulopathies, deformity of spine, patients on antiarrythmic treatment, alcohol or drug abuse, pregnant patients, surgeries more than 3 hr were excluded. The data has been analyzed using Statistical Package For Social Sciences (SPSS) software version 23, where independent sample T test (to measure difference between two groups), Chi Square test has been performed. Moreover, contingency table analysis (for association between rows and columns), analysed by Fischer test And p value thus calculated using these tools were considered statistically significant if less than 0.05.
- RESULTS AND DISCUSSION
Total sample size was taken as 60, group R 30 patients were given 15 mL of 0.75%, ropivacaine epidurally whereas Group B were given 15 mL of 0.5% Bupivacaine. Premedication with tab alprazolam 0.5 mg and ranitidine 150 mg was given orally the night before surgery. Patients were asked to maintain nil per oral status for at least for 8 hrs. In the operation theatre, baseline blood pressure and pulse rate, saturation was recorded. An 18G IV cannula was inserted and all patients were preloaded with 500 mL of Ringer lactate 30 mins prior to the epidural procedure and were premedicated with Inj. Midazolam 1 mg IV before the epidural block. All epidural blocks were performed under strict aseptic conditions in sitting or lateral position. After 16 G epidural needle inserting in L3-L4 interspace (midline approach), 18G epidural catheter was introduced. Then test dose of 3ml 2% lignocaine with adrenaline 1:200,000, was given in absence of signs of subarachnoid and intravascular injection, then 15 ml of study drug was administered at 5 min interval after negative aspiration for blood and cerebrospinal fluid. Sensory blockade were assessed by pinprick method using a 27G hypodermic needle and onset of sensory block (time from epidural injection to loss of pinprick sensation at L1 level). Maximum dermatomal level block were assessed by pinprick method and was taken as the highest level of sensory blockade and duration of analgesia was taken from the time of injection till the patient complains of pain at the site of surgery. The surgery was started when T12 level of sensory block is achieved. Degree of motor block was assessed using Modified Bromage scale. Time for the onset of motor block (time from epidural injection from the time Bromage grade 0 changed to grade 1) duration of motor block was taken from the time of injection till the patient attains complete motor recovery (Bromage 0) and maximum level of motor block achieved according to Bromage scale was noted. Preoperative vitals were taken as baseline .Time of completion of injection of drug was recorded as 0 min. In both the groups, bilateral blockade assessments were performed and hemodynamic parameters as heart rate, mean arterial blood pressure were recorded repeatedly at 1, 3, 5, 10, 20, 30 min then after every 30 min till surgery is over. For those surgeries that were completed prior to 3 hours, block assessment and hemodynamic were recorded until 3 hours. Patients were observed for complications hypotension, hypertension, bradycardia, vomiting, hypoxemia, and was treated as required. Tachycardia was defined as heart rate >100 beats/min, hypertension when systolic blood pressure was>180 mmHg. Hypotension was defined as fall in mean arterial pressure by >20% from baseline, and was treated by IV bolus of crystalloid and incremental doses of IV Inj Mephetermine. Bradycardia was defined as reduction in heart rate <50 beats/min, and was treated with intravenous atropine (0.01 mg/kg). Patients were transferred to the post anesthesia care unit and monitored vitals. The study sample comprised of 60 patients aged between 18 to 71 years. No significant difference was found compared to Age (p-value 0.060), Sex (p value 0.795) and BMI (p value 0.816) between group R and group B.
Table 01: Onset of sensory and motor block between two groups
|
Parameters |
Group |
Mean difference |
p-value |
|||
| Ropivacaine | Bupivacaine | |||||
| Mean | Std.
Deviation |
Mean | Std.
Deviation |
|||
| Onset of
Sensory Block (min.) |
4.40 |
0.932 |
4.40 |
0.932 |
0.000 |
1.000 |
| Onset of Motor Block (min.) | 18.33 | 2.397 | 18 | 2.491 | 0.333 | 0.305
|
Table 02: Duration of sensory and motor block between two groups
|
Parameters |
Group | Mean difference | p-value | |||
| Ropivacaine | Bupivacaine | |||||
| Mean | Std.
Deviation |
Mean | Std.
Deviation |
|||
| Duration of
Sensory block |
153.00 | 21.359 | 154.00 | 20.443 | -1 | 0.854 |
| Duration of
motor block (min.) |
128.00 |
15.625 |
165.00 |
15.256 |
-37 |
0.000
|
Whereas, In group R highest number of patients 17 (56.7%) attained T10 level, while minimum 4 (10%) patient attained T8 level. Similarly, 10 (33.3 %) patients attained T12 level. In group B 15(50 %, maximum) patients attained T10 levels, 11 (36.7%) patients attaining T12 level and 4 (13.3 %, least) attaining T8 level. The p-value 0.305 implied that there was no significant difference in maximum level of sensory block between two groups. In Ropivacaine group, there were 6 patients (20%) who had scale 3 block and 24 patients (80%) who had scale 4. In Bupivacaine group, 4 patients (13.3%) had scale 3 block and 26 patients (86.7%) had scale 4 block. The percentage distribution of patients who had scale 3 and scale 4 block was approximately similar in both the groups. The p-value 0.488 implied that there was no statistically significant difference in the maximum level of motor block between two groups.
Table 3: Comparison of mean arterial blood pressure at different time intervals between two groups
| MAP
(mm/Hg) |
Group |
Mean difference |
p-value |
|||
| Ropivacaine | Bupivacaine | |||||
| Mean | Std. Deviation | Mean | Std. Deviation | |||
| 0 min | 99.93 | 5.311 | 99.97 | 5.301 | -0.033 | 0.981 |
| 1 min | 98.07 | 4.996 | 97.07 | 5.030 | 1.000 | 0.443 |
| 3 min | 95.10 | 4.992 | 93.50 | 4.644 | 1.600 | 0.204 |
| 5 min | 93.07 | 4.653 | 89.83 | 4.480 | 3.233 | 0.280 |
| 10 min | 90.90 | 4.262 | 86.47 | 4.501 | 4.433 | 0.220 |
| 20 min | 88.50 | 3.998 | 83.30 | 4.236 | 5.200 | 0.150 |
| 30 min | 86.50 | 3.928 | 80.37 | 3.917 | 6.133 | 0.110 |
| 60 min | 85.00 | 3.787 | 77.93 | 4.017 | 7.067 | 0.090 |
| 90 min | 83.23 | 3.559 | 75.23 | 3.730 | 8.000 | 0.080 |
| 120 min | 82.10 | 3.325 | 72.50 | 3.617 | 9.600 | 0.070 |
| 150 min | 81.57 | 2.944 | 69.80 | 3.585 | 11.767 | 0.065 |
| 180 min | 81.60 | 2.943 | 66.83 | 3.485 | 14.767 | 0.057 |
Table 04: Comparison of Heart Rate in different time intervals between two groups
| Heart Rate | Group |
Mean difference |
p-value |
|||
| Ropivacaine | Bupivacaine | |||||
| Mean | Std.
Deviation |
Mean | Std.
Deviation |
|||
| Baseline | 78.40 | 3.865 | 77.13 | 4.049 | 1.267 | 0.220 |
| 0 min | 78.73 | 3.532 | 77.13 | 4.049 | 1.66 | 0.108 |
| 1 min | 76.97 | 3.090 | 75.60 | 3.856 | 1.367 | 1.135 |
| 3 min | 75.90 | 2.964 | 73.20 | 3.680 | 2.7 | 0.125 |
| 5 min | 73.90 | 2.482 | 70.40 | 3.092 | 3.50 | 0.118 |
| 10 min | 72.03 | 2.205 | 67.90 | 2.833 | 4.133 | 0.112 |
| 20 min | 70.43 | 1.755 | 65.40 | 2.686 | 5.033 | 0.097 |
| 30 min | 68.90 | 2.354 | 62.63 | 2.189 | 6.267 | 0.086 |
| 60 min | 67.07 | 2.083 | 60.30 | 2.548 | 6.767 | 0.079 |
| 90 min | 65.90 | 2.006 | 59.03 | 2.606 | 6.867 | 0.071 |
| 120 min | 64.37 | 1.903 | 57.23 | 1.851 | 7.133 | 0.068 |
| 150 min | 63.23 | 1.832 | 56.37 | 1.884 | 6.867 | 0.062 |
| 180 min | 61.87 | 1.613 | 56.13 | 2.330 | 5.733 | 0.052 |
3.2 Discussion
Epidural anaesthesia is a regional anaesthesia technique that is most commonly used in lower limb surgeries. A study compared the effects of 20 ml 0.75 percent ropivacaine and 20 ml 0.5% bupivacaine for epidural anaesthesia in patients undergoing lower abdominal and lower extremity surgeries [19]. It discovered that the onset of motor block was statistically significant and that it occurred more quickly in the case of bupivacaine. This could be because bupivacaine is more lipid soluble, which allows it to penetrate large motor fibres more quickly [20]. A study designed a randomised double-blind study in which they compared the clinical effectiveness of 0.5% Ropivacaine and 0.5% Bupivacaine in patients who were undergoing surgery on their lower extremities. They discovered that there was no statistical difference in the onset of sensory or motor block between the two groups [21]. A recent study compared 15 ml of 0.5% Bupivacaine and 15 ml of 0.75 % Ropivacaine when administered epidurally, it discovered that the mean duration of sensory block in the Ropivacaine and Bupivacaine group was 272 minutes and 266 minutes, respectively, with comparable results [22]. However, the mean duration of motor block for Ropivacaine and Bupivacaine was 190 minutes and 194 minutes, respectively, with statistically significant results [23]. The effects of Ropivacaine 20 ml 0.75% (group B) and Bupivacaine 20 ml 0.5% (group A), the study discovered that the total duration of sensory block was 403±16.70 minutes in group A and 413.5±24.67 minutes in group B (p=0.0007), the Ropivacaine group had a longer duration of sensory block, but the duration of motor blockade was significantly shorter in the Ropivacaine group (p<0.05) [24]. One possible explanation for this is that the anaesthetic potency of the drug or the degree of protein binding varies from patient to patient. Considering that the lipid solubility of Bupivacaine is higher than that of Ropivacaine, a higher lipid solubility results in a faster absorption of the drug [25]. In a lower availability of the drug in space, which in turn causes its analgesic action to last for a shorter period of time. Additionally, because of its vasoconstrictive property, ropivacaine has the potential to increase the availability of the drug in the epidural space, which could potentially extend the duration of the block [26]. A study conducted on 126 patients who were undergoing elective hip surgery were given 20 millilitres of either 1.0% Ropivacaine or 0.5% Bupivacaine extradurally [27]. When compared to 0.5% Bupivacaine, 1% Ropivacaine was able to provide relief from pain and motor block for a longer period of time [28]. The result of the use of a higher concentration dose of Ropivacaine, which led to a longer duration of analgesia. Additionally, the number of patients who required injections of atropine and ephedrine to treat bradycardia and hypotension was higher in the group that received 1% Ropivacaine [29]. Because of this, the utilisation of a higher concentration dose of ropivacaine might be the potential cause of increased hemodynamic disruptions. In addition, the research consisted entirely of hip surgeries, which may account for a greater amount of blood loss, which may lead to an increase in the hemodynamic changes [30]. Another study compared that 20ml 0.5% Bupivacaine and 20ml 0.75 percent Ropivacaine epidurally, it discovered that the maximum level of sensory block was T4 in both groups, and the results were comparable [31]. However, when it came to the level of motor blockade, they discovered that the maximum number of patients in both groups attained bromage scale 4.16 [32]. The maximum sensory level that was achieved was high, which may be due to the higher volume of drug that was used, which facilitated the higher spread to the dermatomal level of sensory analgesia [33]. In contrast, the similar results when it came to motor blockade from this study, a randomised double blind study compared epidural anaesthesia using 20 ml of 1% Ropivacaine and 0.75 % Bupivacaine through an epidural catheter [34]. The researchers came to the conclusion that cardiovascular changes and the overall incidence of side effects were comparable in both groups, which is similar to the findings that we obtained [35]. This study compared the values at the beginning of the study to the values achieved during the anaesthetic effects between two different study groups. It is possible that the actual effectiveness of the drugs under study was not determined because there was no control group to compare them to. There were specific time intervals during which we observed the hemodynamic parameters; continuous monitoring of the parameters, particularly blood pressure, through the utilisation of invasive hemodynamic monitoring devices might have resulted in more accurate findings. As a result of the fact that this study was conducted on patients with ASA PS I and II as well as those who did not have significant cardiovascular diseases, the findings of this study may or may not be correlated with those of patients with higher grades of ASA PS. Single doses of drugs were the subject of our research. When it comes to determining the appropriate dose of the drugs under study, a dose response study might prove to be helpful.
- CONCLUSIONS
The epidural blockade is becoming one of the most useful and versatile procedures in modern anesthesiology as it provides effective surgical anesthesia. In equal concentrations, the degree of motor blockade is less pronounced with Ropivacaine, and there is a greater propensity for blocking pain transmitting A-delta and C fibers rather than A-α motor fibers and an effective alternate to epidural Bupivacaine for major lower limb orthopedic surgery. This study compared the values at the beginning of the study to the values achieved during the anaesthetic effects between two different study groups. It is possible that the actual effectiveness of the drugs under study was not determined because there was no control group to compare them. There were specific time intervals during which we observed the hemodynamic parameters; continuous monitoring of the parameters, particularly blood pressure, through the utilisation of invasive hemodynamic monitoring devices might have resulted in more accurate findings Epidural anesthesia in lower limb orthopedic surgeries can be safely achieved using drug 15 ml of 0.75 % of Ropivacaine which provides adequate sensory and motor block for desired lower limb surgery and with shorter duration of motor block provides additional advantage of early ambulation or mobilization in patients with orthopedic surgeries. A significant limitation of this prospective study is the limited number of participants in the sample. The only way to arrive at a conclusive conclusion is to conduct additional research with a significant number of patients. It is possible to conduct additional prospective research with a larger sample size in order to provide support for our findings.
REFERENCES
- Biradar, V. K., Patel, M., Patel, K., & Panditrao, M. (2024). Comparative Study Of Dexmedetomidine Versus Fentanyl As An Adjuvant To Ropivacaine (0.75%) In Epidural Anaesthesia In Lower Limb Orthopaedic Surgery. Archives Of Anesthesiology And Critical Care.
- Bukhari, Saima & Attar, Meshari & Khalid, Amna & Riaz, Mariam & Khalid, Henna & Saad, Ammar & Zulfiqar, Rabia. (2024). EVALUATION OF HEPATIC, RENAL AND HEMATOLOGIC PARAMETERS IN PATIENTS ON LONG-TERM LOW-DOSE METHOTREXATE THERAPY IN RHEUMATOID ARTHRITIS. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1439-1446.
- Mahajan, H. M., & Patel, S. J. (2023). To Compare The Efficacy Of Intrathecal 0.75% Heavy Ropivacaine And 0.5% Heavy Bupivacaine For Lower Abdominal And Lower Limb Surgery. Asian Journal Of Medical Sciences, 14(9).
- Majumder, R. Comparison Of Epidural Anaesthesia Between Levobupivacaine With Clonidine And Ropivacaine With Clonidine In Lower Limb And Lower Abdominal Surgeries.
- Riaz, Mariam & Javed, Maham & Bukhari, Saima & Shaheen, Faiza & Khan, Tariq & Khalid, Henna & Zulfiqar, Rabia. (2024). BLOODSTREAM INFECTIONS AND TRENDS OF ANTIMICROBIAL SENSITIVITY PATTERN: A LABORATORY BASED STUDY. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1421-1428.
- Nagabhushanam, K., Vahida, S., Bommisetty, T. K., & Sudharani, G. G. N. (2024). A Comparision Of Clinical Effects Of Of 0.5% Ropivacaine Vs Levobupivacaine For Epidural Anesthesia In Patients Undergoing Abdominal And Lowerlimb Surgeries. European Journal Of Cardiovascular Medicine, 14(1).
- Gujral, S., Singh, B., Solanki, R. K., Babita, B., Yadav, S., Pipal, R. K., … & Pipal, V. R. (2022). A Comparative Study Of Analgesic Efficacy Of Epidural Ropivacaine With Dexmedetomidine Versus Ropivacaine With Ketamine In Adult Patients Undergoing Elective Lower Limb Surgery. Cureus, 14(7).
- Zahra, Musarrat & Bukhari, Saima & Khan, Tariq & Zakir, Afsheen & Munshi, Muhammad & Mehnaz, Gul & Zulfiqar, Rabia. (2024). Comparative Analysis Of Incidence Of Non-Opioid Analgesic Self-Medication Practice Among Health Associates. Journal of Population Therapeutics and Clinical Pharmacology. 31. 1649-1656. 10.53555/jptcp.v31i4.5980.
- Munir, Shaouki & Biswas, Anirudha & Shakil, Jamil & Mouri, Sadia & Mostafa, Shekh Mohammad & Estoque, Arevalo & Tantong, Alkauzar & Zulfiqar, Rabia. (2024). COMPARISON OF QUALITY ASSURANCE, EMPATHY, AND BURNOUT IN HEALTHCARE PEOPLE SETTINGS: A DESCRIPTIVE STUDY OF PATIENTS AND HEALTHCARE ASSOCIATES. Chinese Science Bulletin (Chinese Version). 69. 1267-1276.
- Sana Jamil, Sidra Anwar, Muhammad Anwar Awan, Sania Alam & Kamal Anwar (2023). Comparison Of Measurement Techniques Of Amplitude Of Accommodation In Young Adults. Dinkum Journal Of Medical Innovations, 2(10):370-375.
- Mutahira, Ayesha & Bukhari, Saima & Uttra, Awais & Saeed, Arooj & Rashid, Salma & Ashhab, Atiq & Tufail, Tabussam & Zulfiqar, Rabia. (2024). INVESTIGATING THE INTERACTION BETWEEN DOPAMINE RECEPTORS AND ANTIBODIES AGAINST GROUP A STREPTOCOCCUS WITH A RANGE OF DIETARY ANTIGENS. General Medicine. 26. 1311-1817.
- Mutahira, Ayesha & Aishi, Shamima & Ahmad, Fozan & Firas, Noor & Al-Kahachi, Qays & Zulfiqar, Rabia & Qasim, Muhammad Bilal & Aman, Aunima. (2024). AN INVESTIGATION OF COMMON AND DISEASE-SPECIFIC HOST GENE EXPRESSION- MICROBIOME CORRELATIONS AMONG HUMAN DISORDERS: LABORATORY BASED EXPERIMENTAL STUDY. Chinese Science Bulletin. 69. 993-1004.
- Pandey, S., Borkar, S., Monteiro, J. M., Mathew, S., Vernekar, D., Barreto, O., … & Kishan, A. V. (2024). Comparative Study Of 0.5% Bupivacaine, 0.5% Ropivacaine, And 0.75% Ropivacaine With Fentanyl As A Continuous Intraoperative Epidural Infusion On Post-Operative Analgesia. Cureus, 16(5).
- Manisha Gupta, Ramcharan Singh & Mahrukh Asghar (2023). Frequency Of Neck & Arm Pain In Professionals Associated With Posture & Ergonomics. Dinkum Journal Of Medical Innovations, 2(10):376-385.
- Magdi, Fatma & Tinny, Sejuti Sarker & Haque, Arifa & Qamar, Afshan & Malik, Samreen & Haider, Muhammad & Zulfiqar, Rabia. (2024). PRACTICE OF PRESCRIPTION ANTIBIOTIC PROPHYLAXIS IN HEAD AND NECK TUMOR EXCISION: A RETROSPECTIVE STUDY. Journal of Population Therapeutics and Clinical Pharmacology. 31. 101-109. 10.53555/jptcp.v31i2.4219.
- Chauhan, A. P., Pandya, J., & Jain, A. (2020). Comparison Of Block Characteristics And Postoperative Analgesia Of 0.5% Levobupivacaine With 0.5% Ropivacaine In Ultrasound Guided Supraclavicular Block For Orthopedic Forearm Surgery-A Prospective, Comparative, Randomized, Clinical Study. Analgesia, 5, 14.
- KANSE, N. (2020). Comparative Study Of Ropivacaine And Bupivacaine. International Journal Of Pharmaceutical Research (09752366), 12(2).
- Ninu, M., Basumatary, J., & Deka, S. (2022). A Comparative Study Of Ropivacaine And Bupivacaine For Caudal Epidural Anaesthesia In Children Undergoing Lower Abdominal Surgery. European Journal Of Molecular And Clinical Medicine, 9(3), 5330-5340.
- Md. Salah Uddin (2024). Correlation Between Duration Of Preoperative Motor Deficit And Early Postoperative Motor Functional Recovery In Patients With Intradural Extramedullary Spinal Tumor. Dinkum Journal Of Medical Innovations, 3(01):52-63.
- VASANTH, D., NARAYANAN, V., & SENTHIL KUMAR, S. A. (2022). Comparison Between Plain Ropivacaine, Ropivacaine With Buprenorphine And Ropivacaine With Clonidine For Intrathecal Use In Lower Limb Orthopaedic Surgeries: A Randomised Controlled Trial. Journal Of Clinical & Diagnostic Research, 16(9).
- Humza Sohail, Markus Peter Chan & Umaima Nagari (2022). Myocarditis After Receiving The Covid-19 Vaccine In An Enormous Medical Facility. Dinkum Journal Of Medical Innovations, 1(01):07-12.
- Ninu, M., Basumatary, J., & Deka, S. (2022). A Comparative Study Of Ropivacaine And Bupivacaine For Caudal Epidural Anaesthesia In Children Undergoing Lower Abdominal Surgery. European Journal Of Molecular And Clinical Medicine, 9(3), 5330-5340.
- Adhikari, P., Vyas, V., Naseem, S., & Shelke, U. (2020). Comparative Efficacy And Safety Of Intrathecal Ropivacaine Versus Intrathecal Bupivacaine In Patients Undergoing Lower Abdominal Surgical Procedures. Indian Journal Of Pain, 34(1), 43-46.
- Hossain, Zahid & Bhuiyan, Md Saruar & Kabir, Md & Jahan, Sharmila & Rahman, Ehsanur & Zulfiqar, Rabia. (2023). EVALUATION OF BONE MINERAL DENSITY IN PATIENTS WITH MUSCULOSKELETAL PAIN IN A REGIONAL AREA OF BANGLADESH. Zhonghua yi shi za zhi (Beijing, China: 1980). 53. 1453-1459.
- Balasubramanian, A. K. (2023). Comparison Of Clinical Efficacy And Tolerability Of Epidural 0.5% Levobupivacaine With 0.75% Ropivacaine In Patients Undergoing Elective Lower Abdominal Surgery. Rivista Italiana Di Filosofia Analitica Junior, 14(2), 497-515.
- Javaria Arif, Muhammad Anwar Awan, Muhammad Suhail Sarwar, Asad Aslam Khan & Kabir Hussain (2023). Optometric Criteria Of Prescription In Case Of Borderline Refractive Errors. Dinkum Journal Of Medical Innovations, 2(10):386-393.
- Kant, R. A COMPARATIVE STUDY OF FENTANYL AND DEXMEDETOMIDINE FOR EPIDURAL ANALGESIA FOR LOWER LIMB ORTHOPEDIC SURGERY–A PROSPECTIVE DOUBLE-BLIND STUDY.
- Nazeera Banu, C. (2021). A Comparative Evaluation Of Isobaric Levobupivacine Versus Hyperbaric Bupivacaine For Elective Lower Limb Orthopedic Surgeries Under Spinal Anaesthesia (Doctoral Dissertation, Government Mohan Kumaramangalam Medical College, Salem).
- Farmawy, M. S., Mowafy, S. M., & Wahdan, R. A. (2023). Epidural Nalbuphine Versus Dexmedetomidine As Adjuvants To Bupivacaine In Lower Limb Orthopedic Surgeries For Postoperative Analgesia: A Randomized Controlled Trial. BMC Anesthesiology, 23(1), 401.
- Batham, N. S., Hardia, H., Sahoo, T., Jain, A., & Agrawal, A. (2023). To Study And Compare The Effect Of Fentanyl And Dexmedetomidine In Epidural Anaesthesia In Lower Limb Orthopaedic Surgeries When Given As An Adjuvant To 0.5% Bupivacaine. Int J Acad Med Pharm, 5(2), 1340-6.
- Prakash, J., Prabhu, J. P., Kharwar, R. K., Priye, S., Singh, D., & Saran, K. (2020). Comparison Of Epidural Levobupivacaine And Bupivacaine In Lower Abdominal And Lower Limb Surgeries. Bali Journal Of Anesthesiology, 4(3), 95-98.
- Patil, P., Dhulkhed, P. V., & Dhulkhed, V. K. (2023). Isobaric Forms Of Ropivacaine Vs. Bupivacaine In Lower Abdominal Surgeries: A Hospital-Based, Prospective, Comparative Study. Medical Gas Research, 13(3), 123-127.
- Sorathiya, A. R., Prajapati, S., Kansagra, M., Patel, B. R., Patel, J., & Desai, D. (2023). Comparative Study Of Bupivacaine.
- Kore Shilpa, S., Ubhe, S. B., Shikalgar, S., & Lomate, P. (2022). Observational Cohort Study Of Ropivacaine And Bupivacaine In Spinal Anaesthesia. Journal Of Pharmaceutical Negative Results, 9869-9879.
- Latwal, B. S., Singam, A., Shrey, S., Jejani, A., & Nagpure, P. (2020). A Comparative Study Of Intrathecal 0.5% Hyperbaric Bupivacaine & Intrathecal 0.75% Isobaric Ropivacaine In Lower Abdominal Surgeries. J Evol Med Dent Sci, 9(5), 256-61.
Publication History
Submitted: December 22, 2023
Accepted: January 14, 2024
Published: February 29, 2024
Identification
D-0248
DOI
https://doi.org/10.71017/djmi.3.2.d-0248
Citation
Dr. Sangam Pokharel, Dr. Rajesh Yadav, Dr. Anima Pradhan & Dr. Ashmita Paudel (2024). Comparative Study of Bupivacaine 0.5% and Ropivacaine 0.75% Epidurally In Lower Limb Orthopedic Surgeries. Dinkum Journal of Medical Innovations, 3(02):165-173.
Copyright
© 2024 DJMI. All rights reserved