

")
Publication History
Submitted: January 24, 2024
Accepted: February 13, 2024
Published: February 29, 2024
Identification
D-0249
DOI
https://doi.org/10.71017/djmi.3.2.d-0249
Citation
Ms. Saroja Poudel & Dr. Rajesh Niraula (2024). Comprehensive study of Placenta Previa & Its Psychological Consequences. Dinkum Journal of Medical Innovations, 3(02):174-187.
Copyright
© 2024 DJMI. All rights reserved
174-187
Comprehensive study of Placenta Previa & Its Psychological ConsequencesOriginal Article
Ms. Saroja Poudel 1 *, Dr. Rajesh Niraula 2
- Obstetrical & Gynaecological Nursing, Hubei University of Medicine, China.
- Department of Medical Imaging, Hubei University of Medicine, China.
* Correspondence: Saroja.niraula@gmail.com
Abstract: Placenta previa is when the placenta is partially or fully implanted in the lower uterine segment. It causes most antepartum haemorrhage, changing hormone levels during pregnancy and after can cause anxiety, melancholy, and mood swings. The majority of women eventually got over these feelings. However, if not recognized early, some women may develop depression and other mental illnesses. This study evaluated the mother & baby Psychological Consequences of Placenta Previa. Cross sectional study with Purposive sampling conducted at the Obstetrics ward, 3 A General Hospital Shiyan, Hubei province China. Questionnaires, hospital observations, and medical records will capture most of the data. PROMIS (Patient Reported Outcomes measurement information system) measures psychological repercussions from N=100 respondents. The Edinburg postnatal depression scale (EPDS) measures postnatal depression. The study showed Placenta Previa was prevalent among 20-30-year-olds and multipara. Most mothers used caesarean sections in the past. About 30% of mothers had EPDS scores above 10. During delivery, 23% of moms need blood transfusion. Various issues require 20% of women to use MICU. 84% of newborns had APGAR 8-10. 71% of babies weighed 2500-3500g. 16% of babies need NICU. 5% of newborns were congenitally abnormal. To quantify psychological effects, we examined physical, mental, and social health in Placenta Previa mothers and found that 70% were pleased. 46% of mothers reported mild baby care fear. 41% report little sleep disruption. 10% appeared disoriented and puzzled. 38% needed mild help with daily tasks. About 76% of mothers responded to instructions. 83% of mothers responded to external stimuli where 76% of mothers were satisfied with therapy. Although most women had satisfactory results, some had serious psychological issues. It found 30% of mothers likely depressed. Although most women enjoyed good physical, mental, and social health, some saw it as a difficult circumstance and developed despair and other psychological issues that we can’t ignore.
Keywords: placenta Previa, Psychology, Edinburgh Postnatal Depression Scale (EPDS)
- INTRODUCTION
A condition known as placenta previa occurs when the placenta is present in the lower uterine segment, either in part or in its entirety. A significant amount of antepartum bleeding and labor that occurs before the due date are frequently connected with it [1]. One of the most common reasons for antepartum hemorrhage is a condition known as placenta previa. Most of the research did not provide any explanation about the psychological elements of moms. During the third trimester of pregnancy, around one in every two hundred pregnant women will experienceplacenta previa [2]. Within the range of 0.4 to 0.5 percent of all pregnancies [3], it does influence. Many studies on placenta previa have shown that risk factors for placenta previa include advanced maternal age, having more than one partner, having a previous cesarean section, and having had an abortion in the past. Placenta previa continues to be a risk factor for bad outcomes for both the mother and the perinatal period [4]. In order to manage the related maternal and neonatal complications, it is necessary to discover placenta previa at an early stage, do a thorough evaluation, and deliver the baby at the appropriate time. Placenta previa is one of the most significant difficulties that can occur during pregnancy. It is linked to a wide range of additional complications that can affect both the mother and the fetus and the newborn baby [5]. The majority of these are direct results of hemorrhage that occurs during the antepartum and intrapartum periods of the mother. As compared to women who do not have placenta previa, the prevalence of acute pulmonary hypertension (APH) among pregnant women with placenta previa is roughly 10 times higher [6]. The prevalence of placenta previa has been increasing in tandem with the rising rate of cesarean birth. The prevalence of this condition varies from country to country, and it has developed into a significant cause for concern in terms of public health all over the world [7]. In the beginning, when a woman becomes pregnant, she is filled with joy. Immediately after the excitement of becoming pregnant, the worry that comes along with it [8]. If the baby is born healthy or if there are any complications that may emerge, the woman will get anxious. It is possible for the diagnosis of placenta previa to be an extremely frustrating experience [9]. In order to ensure the patient’s mental and physical health during their pregnancy, it is necessary to provide regular attention. It is possible that the pregnant patient’s psychological status will determine her ability to respond to our instructions and how she will care for herself in terms of maintaining personal hygiene, grooming, sleep, diet, bladder and bowel habits, thoughts, emotions, alertness, behaviors, adaptation, interpersonal relationships, cognitive function, habit, social support, and the ability to participate in social activities [10]. The study of mental illness is simply one aspect of psychology; it also encompasses the study of optimal human functioning, sometimes known as mental wellness. The occurrence of an unexpected event can have psychological repercussions [11]. The inability to ventilate one’s feelings causes them to become more intense. The presence of worry causes people to suffer a physiological weakening and an increase in their level of terror. Because of this, a psychological condition could develop. Because of the continual fluctuations in hormone levels that occur throughout pregnancy and during the postpartum period, a woman may experience feelings of worry, melancholy, mood swings, irritability, and confusion for a variety of reasons [12]. Following a specific amount of time, these feelings disappeared in the majority of the women. On the other hand, if it is not recognized at an early stage, it can increase the risk of depression and other mental illnesses in certain women [13]. While it is easier to detect the physiological changes that occur in a pregnant woman’s body, it is also easier to observe the changes that occur in the psyche of a pregnant mother when she is pregnant [14]. These psychological changes that are associated with pregnancy include spikes in hormone levels, which can have an effect on mood, as well as the ability to think and remember. Because she must broaden her sense of self in order to embrace her kid as a component of herself, the process of labor and delivery causes her to undergo a transformation in her sense of self [15]. The 25th Goldbort. On account of the fact that the prevalence of depression during pregnancy is often rather high, depression during pregnancy is a major concern for the public health sector. Teixeira and company [16]. The puerperium and pregnancy are both recognized as risk factors for the development and worsening of mental health disorders. The prevalence of mental disease is comparable in both the puerperium and the gestational period [17]. However, it is believed that the diagnosis during this era is disregarded, and there is a lack of research that is conducted to detect psychological changes that occur throughout pregnancy and the outcomes of obstetric procedures [18]. It is not possible to measure psychological repercussions using diagnostic tests or any other technical means; thus, the Patient Report Outcomes Management Information System (PROMIS) should be in use [19]. The woman’s emotional responses, in addition to the diagnosis of the sickness, are also a contributing factor [20]. Changes in her environment, lifestyle, hospitalization, lengthy bed rest, many examinations, absence from her usual employment, mental unpreparedness to be pregnant and mother, early baby, past loss or stillbirth, and other factors may have contributed to her pregnancy and motherhood. It is stressful for the mother as well as the other members of the family [21]. Additionally, parents who have lost their child are in a state of crisis. In today’s world, in the name of modernization and the advancement of science and technology, there is a change in family structures that brings about a lack of care during pregnancy, after delivery, and for newborns [22].
- MATERIALS AND METHODS
Cross sectional study with Purposive sampling conducted at the Obstetrics ward, 3 A General Hospital Shiyan, Hubei province China. Information will be collected from N=100 patients after applying with inclusion and exclusion criteria women were analyzed with respects to their age parity, gestational age, clinical features, history of warning leeding, duration of hospitalization, need for blood transfusion, delivery route, need for MICU. History of psychiatric is order, socioeconomic status, obstetrical history especially about miscarriages, stillbirth, stress, social support, thoughts, behaviors, emotion, alertness, cognitive function, ability to participate in social role, habit, self efficacy, interpersonal relationship. For the new born APGAR score, birth weight, need for NICU, still birth rate, neonatal mortality rate will be recorded. Primarily information will be collected through Questionnaire and Observation of the patient during their hospital stay and through medical documents. Psychological consequences can’t be measured directly by diagnostic test or by other technical means, so PROMIS (Patient Reported Outcomes measurement information system) is used. IT help researcher to get valid and flexible measures of health status of physical, mental and social well beings from patient perspectives. Edinburg postnatal depression scale (EPDS) is used to measure depression level of postnatal mother. Data analysis will be carried out by using appropriate statistical methods. All the major findings will be interpreted and discussed within the context of prior research. The data was analyzed using the IBM (SPSS).

Figure 01: Roadmap showing research methodology
- RESULTS AND DISCUSSION
3.1 Demographical Analysis
In this study we investigated the status of mother, baby and psychological consequences seen in the mothers. It has found the mother history regarding chronic disease, medical history, surgical history, age, parity of mother, mode of delivery, blood transfusion, need for NICU, abortion, preset mode of delivery. To find the status of baby we investigated birth weight of baby, APGAR, need of NICU, congenital abnormalities. To investigate the psychological status of mother we observed mental, social and physical health of mother. Along with this we also used EPDS scale to measure the presence of depression.
Table 01: Status of mother with Placenta Previa
| Parameters | Frequency | Percentage | |
| AGE | Less than 20 years | 0 | 0 |
| 20 – 30 years | 66 | 66% | |
| 31 – 40 years | 34 | 34% | |
| More than 40 years | 0 | 0 | |
|
Parity |
Primi |
41 |
41% |
| Multi(2-3) | 55 | 55% | |
| Grand multi(>=4) | 4 | 4% | |
|
Past mode of delivery |
Cesarean Section |
72 |
72% |
| Normal delivery | 28 | 28% | |
|
H/O menstrual cycleS |
Regular |
72 |
72% |
| Irregular | 18 | 18% | |
| Dysmenorrhoea | 10 | 10% | |
|
Past medical history |
Chronic disease (yes) |
32 |
32% |
| Heart disease | 13 | 13% | |
| HTN | 6 | 6% | |
| DM | 13 | 13% | |
| Chronic disease (No) | 68 | 68% | |
|
Past history of surgery |
Yes |
36 |
36% |
| No | 64 | 64% | |
|
Past history of still birth |
Yes |
8 |
8% |
| No | 92 | 92% | |
|
History of abortion |
Yes |
54 |
54% |
| Less than 2 | 30 | 30% | |
| 2 – 3 | 18 | 18% | |
| 4 – 5 | 6 | 6% | |
| More than 5 | 0 | 0 | |
| No | 46 | 46% | |
On the basis of mother demographic data history and present condition it was found that Most of the women about 66% with placenta previa were between 20-30 years and remaining 34% were in between 31-40 years of age. Minimum age of 20-30 years to maximum age of 31-40 years had got Placenta Previa. It was commonly seen in age group between 20-30 years. Most of the woman about 55% women with placenta previa was multipara whereas 41% of women were primi and remaining 4% were grandmultipara. Maximum number of mother who was diagnosed with Placenta Previa had given birth in the past by cesarean section. About 72% given birth by cesarean section and remaining 28% by normal delivery. About 72% of mother said that they had regular menstrual cycle.18%of mother have irregular menstrual cycle and remaining 10 % told that they suffered from dysmenorrhoea during menstrual cycle.
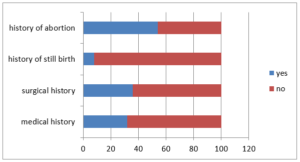
Figure 02: History of mother with Placenta Previa
About 68% of mother told that they were not suffered from chronic diseases which were shown in figure 2. Remaining 32 % of mothers were suffered from different types of chronic diseases such as 13% from cardiovascular diseases, 6% from hypertension (HTN) and remaining 13% from DM. Only 36 % of mother had done surgery in the past and remaining 64% told they never had surgery. About 8% mother had given stillbirth in the past. Remaining 92% of mothers hadn’t given stillbirth. About 46% of mother didn’t have history of abortion and remaining 54% of mothers had history of abortion. Maximum number of mother about 30 % had done abortion for less than 2 times .18% of mother had done abortion for 2-3 times and remaining 6% of mother had abortion for 4-5 times.
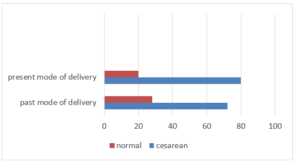
Figure 03: Mode of delivery
Most of the mothers about 80% with placenta previa had given birth by cesarean section and remaining 20% given birth by normal delivery.
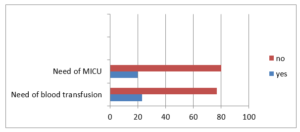
Figure 04: Correlation between MICU and blood transfusion
Only 23% of mother needs blood transfusion during delivery. About 20% of the mother who were diagnosed with Placenta Previa needs MICU.
Table 02: Status of Mother at Delivery
| Parameters | Frequency | Percentage | |
| Present delivery route | Normal delivery | 20 | 20% |
| Cesarean section | 80 | 80% | |
|
Need of blood transfusion |
Yes |
23 |
23% |
| No | 77 | 77% | |
|
Need for MICU |
Yes |
20 |
20% |
| NO | 80 | 80% | |
On the basis of this study the outcomes of the new born baby was 84% of the new born have APGAR score between 8-10 and remaining 16 % of baby have APGAR score in between 5-7. 71% of baby had weight in between 2500-3500gm.18% of baby had weight in between 3500gm-4500gm and remaining 11 % of baby had weight less than 2500gm. 16% of baby need NICU. 5 % of babies had congenital abnormalities which were shown in figure 5.
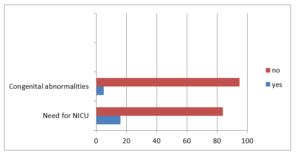
Figure 05: Correlation between congenital abnormalities and NICU
Table 03: Status of New Born Baby
| Parameters | Frequency | Percentage | |
| APGAR score | 0 – 4 | 0 | 0% |
| 5 – 7 | 16 | 16% | |
| 8 – 10 | 84 | 84% | |
|
Birth weight |
Less than 2500gm |
11 |
11%% |
| 2500gm to <3500gm | 71 | 71% | |
| 3500gm-4500gm | 18 | 18% | |
| More than 4500gm | 0 | 0% | |
|
Need for NICU |
Yes |
16 |
16% |
| NO | 84 | 84% | |
|
Congenital Abnormalities |
Yes |
5 |
5% |
| No | 95 | 95% | |
Table 04: Physical Health of Mother
| Parameters | Frequency | Percentage | |
| Fatigability | No | 32 | 32% |
| Mild | 54 | 54% | |
| Moderate | 14 | 14% | |
| Severe | 0 | 0% | |
|
Sleeping Pattern |
Good sleep |
59 |
59% |
| Little disturbance | 41 | 41% | |
| Moderate disturbance | 0 | 0 % | |
| No sleep | 0 | 0% | |
|
Presence of any physical problem |
Constipation |
30 |
30% |
| Diarrhea | 0 | 0% | |
| Nausea and vomiting | 10 | 10% | |
| Other | 60 | 60% | |
|
Feeling of pain |
Yes |
53 |
53% |
| No | 47 | 47% | |
|
Severity of pain |
Mild |
35 |
35% |
| Moderate | 14 | 14 % | |
| Severe | 4 | 4% | |
| Alternating | 0 | 0% | |
3.2 Physical Health
Under physical health it was found that 32% of mother said they were not tired whereas 54%of woman complains of mild fatigue and remaining 14% of mother told they were moderately tired. While asking about sleeping pattern 59% of mother told their sleeping pattern is good and remaining 41% complain they have little disturbance while sleeping. Out of 100 mother 30 % of mother said that they were suffering from constipation whereas 10 % of mother suffered from nausea vomiting. About 35% of mother told that they have got mild pain whereas 14% of mother had got moderate pain and 4% had severe pain and remaining 47% had no pain.
Table 05: Mental Health of Mother
| Parameters | Frequency | Percentage | |
| Past history of mental illness | Yes | 16 | 16% |
| Depression | 6 | 6% | |
| Anxiety | 10 | 10% | |
| Psychosis | 0 | 0% | |
| Other | 0 | 0% | |
| NO | 84 | 84% | |
|
Habit of alcohol/smoking |
No any habit |
80 |
80% |
| Occasionally | 20 | 20% | |
| frequently | 0 | 0% | |
| Daily | 0 | 0% | |
|
Mood |
Happy |
70 |
70% |
| Anger | 12 | 12% | |
| Sad | 10 | 10% | |
| Confused | 8 | 8% | |
| Orientation | Oriented | 90 | 90% |
| Can say little | 10 | 10% | |
| Confused | 0 | 0% | |
| Disoriented | 0 | 0% | |
|
Fear regarding care of new born |
No fear Mild fear Moderate fear Severe fear |
40 46 14 0 |
40% 46% 14% 0% |
| Coping with stressful situations | Easily cope | 88 | 88% |
| Self harm | 0 | 0% | |
| Harm to other | 0 | 0% | |
| Avoidance | 12 | 12% | |
3.3 Mental Health
About 6% of mother told that in the past they have got depression and 10% of mother had got anxiety and remaining 84% told that they have no any history of mental illness. Out of hundred 80% mother told that she have no any habit of alcohol and smoking and remaining 20% mother told that they drink and smoke occasionally. Talking about the mood 70% of mother told they were in happy mood, 12 % of mother told that they were angry, 10% were sad and remaining 8% were confused about their mood. While asking the mother do they have any fear regarding care of the new born baby 40% of mother told that they have no any fear whereas 46% of mother told that they have mild fear regarding care of the new born baby and remaining 14% told that they have got moderate fear. While observing the orientation level of mother it was found that 90% of mothers were oriented towards time place and person, whereas remaining 10 % were partially oriented and looked confused. While asking how they cope with stressful situations 88% woman told that they easily cope with stressful situation whereas 12 % of mothers avoid the situation.
Table 06: Edinburgh Postnatal Depression Scale (EPDS)
| EPDS (EDINBURGH POSTNATAL DEPRESSION SCALE) | |||||
| No. of respondents | Minimum Score | Maximum Score | Mean Score | Standard Deviation | p- value |
| 100 | 1.0 | 17.0 | 8.2609 | 3.97484 | <0.000 |
Edinburg postnatal depression scale (EPDS) was used to measured depression level of postnatal mother. It described the depression level preset in the mother with Placenta Previa mean score is 8.2609 and p value is 0.00 which is less than 0.05.About 30 % of woman got EPDS score greater than 10.This means that 30% of mother had possible depression. Maximum score is 30 and possible depression is 10 or greater.
Table 07: Woman with EPDS score ≥10 and <10
| EPDS Mean± SD P- Value
EPDS ≥ 10 12.680 ±2.020 p 0.00(<0.05) F=1.451, sig=0.1274
|
| EPDS< 10 5.900 ±2.433 p 0.00 (<0.05) |
Shows that mother with EPDS greater and equal had mean of 12.680 and standard deviation 2.020 whereas EPDS less than 10 score had mean of 5.9 and standard deviation of 2.433.While comparing both we have p value 0.00 which is less than 0.05 .
Table 08: Psycho Social Illness Impact on Mother
| Parameters | Frequency | Percentage | |
| Behavior | Politeness | 86 | 86% |
| Rude | 10 | 10% | |
| Confused | 4 | 4% | |
| Ignore | 0 | 0% | |
|
Response to instruction |
Obeys |
76 |
76% |
| Confused | 8 | 8% | |
| Don’t care | 8 | 8% | |
| Other | 8 | 8% | |
|
Awareness of external stimulus |
Responsive |
84 |
84% |
| Response but don’t obey | 11 | 11% | |
| Confused | 6 | 6% | |
| Ignore | 0 | 0% | |
|
Relationship
|
Strong Criticize Family member don’t respond Weak |
90 6 4 0 |
90% 6% 4% 0% |
|
Attention towards child |
Yes |
100 |
100% |
| Aware but don’t response | 0 | 0% | |
| Confused | 0 | 0% | |
| Ignore | 0 | 0% | |
|
Satisfaction with treatment |
strong satisfied |
76 |
76% |
| Satisfied | 24 | 24% | |
| Little satisfied | 0 | 0% | |
| Unsatisfied | 0 | 0% | |
|
Daily Activities |
Perform independently |
37 |
37% |
| Need mild support | 38 | 38% | |
| Moderate support | 15 | 15% | |
| Complete support | 10 | 10% | |
3.4 Social Health
Under social health of mother, it has been observed their behavior 86% of mother behaves politely whereas 10% of mother behaves rudely and remaining 4% looked confused. Almost 76% of mother shows reaction to the instructions, whereas 8% of mother understand but didn’t care and remaining 8% ignored the instructions. 83% of mother was responsive to external stimulus whereas 11% understand but don’t response and remaining 6% were confused. As we talk about the relationship of mother 90% of them have got strong relationship with their family members whereas 6% of the mother criticize their relationship and remaining 4% woman were neglected by their family members. The entire mother told that she gave full attention towards their child. While taking about the daily activities of mother about 37% of mother performed daily activities independently whereas 38% required mild support.15% need moderate support and remaining 10 % need complete support to carry out their daily activities. Out of 100 mother 76% of mother shows strong satisfaction towards treatment, whereas remaining 24% of mother they were satisfied with treatment. There were no any single mothers who weren’t satisfied.
Table 09: Chi square association test result between paired variables.
| Variable 1 | Variable 2 | P-value |
| Need of blood transfusion | Need of MICU | 0.025(<0.05) |
| Present delivery route | Fatigability | 0.021(<0.05) |
| APGAR score | Birth weight | 0.013(<0.05) |
| Mood | Daily activities | 0.034(<0.05) |
| Coping with stressful situation | Relationship | 0.000 (<0.05) |
| History of chronic disease
Orientation
Age Need for NICU Fatigability orientation Response to the instruction mood Attention towards child |
Still birth
Awareness of external stimulus Parity Birth weight Physical problem Awareness of external stimulus Behavior Behavior Fear regarding care of new born |
0.00 0 (<0.05)
0.000 (<0.05) 0.000(<0.05) 0.000(<0.05) 0.000(<0.05) 0.006(<0.05) 0.006(<0.05) 0.001(<0.05) 0.000 (<0.05) |
Table 10: shows the correlation between two variables as their p-value is 0.00(<0.005) which means it is significant
| Variable mean and standard deviation p-value | ||
| Mode of delivery | 1.200±0.402 | 0.000 |
| EPDS | 8.26 ± 3.97 | 0.000 |
| Past abortion | 2.68 ±1.324 | 0.000 |
| Age | 2.34 ± 0.476 | 0.000 |
| Parity | 1.63 ± 0.56237 | 0.000 |
| Chronic disease | 3.36 ± 1.06856 | 0.000 |
| Past mode of delivery | 1.28 ± 0.4512 | 0.000 |
| Blood transfusion | 1.77 ±0.042295 | 0.000 |
| MICU | 1.800 ±0.4020 | 0.000 |
Table shows the correlation between EPDS and different independent variables. As p-value is 0.000 (<0.05).which shows the significant relationship as it affect the psychological condition of mother. It is directly and indirectly is the risk factors to develop psychological problems in the mother during pregnancy and after child birth
3.2 Discussion
The sample included 100 obstetric ward patients with Placenta Previa, women were analysed for age parity, gestational age, clinical characteristics, warning bleeding history, hospitalisation duration, blood transfusion requirement, birth route, and MICU need. EPDS measures historical psychiatric disorder, socioeconomic status, obstetrical history, including miscarriages, stillbirths, stress, social support, thoughts, behaviours, emotion, alertness, cognitivefunction, ability to participate in social role, interpersonal relationship, and depression. Recording APGAR score, birth weight, NICU need, still birth rate, and newborn mortality rate [23]. PROMIS (Patient Reported Outcomes measurement information system) measures psychological repercussions because diagnostic tests cannot. The study focused on Placenta Previa outcomes and mother mental health. Placenta Previa was prevalent in 20-30-year-old women, and 55% were multipara [24]. In the past, 72% of mothers had caesarean sections. 32% of mothers had chronic illnesses. About 8% of mothers reported stillbirths. 54% of mothers had abortions. 80% of Placenta Previa mothers had caesareans. During delivery, 23% of moms need blood transfusion. Various issues require 20% of women to use MICU. 84% of newborns had APGAR 8-10. 71% of babies weighed 2500-3500g. 16% of babies need NICU. 5% of newborns were congenitally abnormal. Physical changes in a pregnant woman’s body are easy to detect, but her mind also changes [25]. Hormonal surges during pregnancy can alter mood, thinking, and memory. All other studies lack patient psychology, this study will reveal Placenta Previa’s psychological effects on women. During pregnancy and postpartum, hormone fluctuations can cause anxiety, sadness, mood swings, irritability, and confusion. The majority of women eventually got over these feelings. However, if not recognised early, some women may develop depression and other mental illnesses [26]. This study examined the psychological effects of motherhood on physical, mental, and social health. Studies on physical, mental, and social health examined psychological issues. The overall status of mothers and babies was favourable, but some women had psychological issues that could lead to mental illness [27]. Recognising and managing the problem early helps reduce childbirth stress. Psychological concerns include fear, relational issues, mental illness, and unpreparedness for the increased duty. About 30% of mothers had EPDS scores above 10, indicating depression [28]. To quantify psychological effects, we examined physical, mental, and social health in Placenta Previa mothers and found that 70% were pleased. 46% of mothers reported mild baby care fear. 41% report little sleep disruption. 10% appeared disoriented and puzzled. 38% needed mild help with daily tasks. About 76% of mothers responded to instructions. 83% of mothers responded to external stimuli, 76% of mothers were satisfied with therapy. Although most women had satisfactory results, some had serious psychological issues. About 23% of mothers needed blood transfusions, whereas 77% did not. Only 5% of mothers needed MICU. A P value of 0.025 (<0.05) indicates a link between blood transfusion and MICU necessity. Age and parity since p = 0.04.66% of women have Placenta Previa between 20-30 years old and 34% between 31-40 years old. 75.6% of women aged 20-30 have placenta previa, while 43.6% of women aged 31-40 have multipara. Placenta Previa was prevalent in 20-30-year-olds and multipara (2-3) [29].Early pregnancy and multipara may cause Placenta Previa. A p-value of 0.013 (<0.05) indicates a link between APGAR score and birth weight. 45.5 % of newborns under 2500gm had APGAR scores between 5-7, while 54.5 % had 8-10 [30]. About 85.9% of newborns with birth weights between 2500g and 3500g had APGAR between 8-10, whereas 14.1% had 5-7. APGAR was 8-10 for 84% of babies weighing 3500-4500g. As the baby gained weight, its APGAR score improved [31]. A p-value of 0.034 (<005) indicates a link between mood and everyday activities, thus, the mother conducted daily tasks independently as her mood improved.70% of mother’s everyday activities were cheerful, whereas 12% were furious [32]. Sad mothers did 10% of everyday activities while confused mothers did 8%. There is a significant association between coping with stress and family relationships (p < 0.05).88% of them have strong relationships and can handle stress. Only 12% of mothers who ignored or avoided difficult situations had healthy relationships [33]. Thus, good relationships depend on individual coping, p-value for the link between chronic illness and stillbirth is 0.000 (<0.05). Chronically sick moms had a higher stillbirth rate, time-place-oriented mothers noticed external stimuli. Both variables were significantly connected (p-value < 0.05). Low birth weight requires NICU. Fear of caring for a newborn increases with attention. Happy women behave well. People’s moods affect their behavior [34].
- CONCLUSIONS
Pregnancy diagnosed with Placenta Preavia may create common psychological responses which can complicate pregnancy and may occurred various psychiatric disorders. After knowing the psychological consequences of women, it provides continuous psychological support during pregnancy and after delivery. In general, the respondents confirmed that mood disturbance, anxiety, depression, low self-esteem, fatigue, poor attitude and stress were among the psychological changes they experienced during pregnancy. This study demonstrated that Placenta Previa was commonly seen in age group 20-30 years, multipara and in the past who had given birth by caesarean section. Overal the status of baby was satisfactory, about 30 % mother had EPDS score greater than 10.It revealed that about 30% of mother had possible depression. Although majority of women had good physical, mental and social health some women had perceived it as very stressful situation and had got chance of developing depression and other psychological problems which can’t be neglected.
REFERENCES
- Sahu, S. A., & Shrivastava, D. (2024). Maternal and Perinatal Outcomes in Placenta Previa: A Comprehensive Review of Evidence. Cureus, 16(5).
- Bukhari, Saima & Attar, Meshari & Khalid, Amna & Riaz, Mariam & Khalid, Henna & Saad, Ammar & Zulfiqar, Rabia. (2024). EVALUATION OF HEPATIC, RENAL AND HEMATOLOGIC PARAMETERS IN PATIENTS ON LONG-TERM LOW-DOSE METHOTREXATE THERAPY IN RHEUMATOID ARTHRITIS. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1439-1446.
- Nahal Mostak Khan, Soheb Ahmed Robin, Lutfullahil Khabir & Sohel Mahmud (2024). Role of Vitamin C in Development of Age Related Cataract. Dinkum Journal of Medical Innovations, 3(01):26-34.
- El Sayed, A. I., Elkashif, M. M. L., Elawany, T. A. A., Fathy, A. M., & Elsaba, H. A. H. F. (2023). Major Placenta Previa in Advanced Age Among Nulliparous With Cesarean Section: A Cross-Sectional Study. International Journal of Childbirth, 13(3), 149-158.
- Riaz, Mariam & Javed, Maham & Bukhari, Saima & Shaheen, Faiza & Khan, Tariq & Khalid, Henna & Zulfiqar, Rabia. (2024). BLOODSTREAM INFECTIONS AND TRENDS OF ANTIMICROBIAL SENSITIVITY PATTERN: A LABORATORY BASED STUDY. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1421-1428.
- Pooja Agarwal & Komal Mishra (2023). Examining the Long-Term Effects of Breastfeeding on Infants’ Neurocognitive and Gross Development. Dinkum Journal of Medical Innovations, 2(02):72-78.
- Flanagan, C., & Troup, L. J. (2024). Psychological flexibility, birth satisfaction and postnatal trauma symptoms in women with abnormally invasive placenta. Journal of Reproductive and Infant Psychology, 42(2), 269-280.
- Zahra, Musarrat & Bukhari, Saima & Khan, Tariq & Zakir, Afsheen & Munshi, Muhammad & Mehnaz, Gul & Zulfiqar, Rabia. (2024). Comparative Analysis Of Incidence Of Non-Opioid Analgesic Self-Medication Practice Among Health Associates. Journal of Population Therapeutics and Clinical Pharmacology. 31. 1649-1656. 10.53555/jptcp.v31i4.5980.
- Sunita Patel, Rebecca Nelson, Jamal Ahammed & Syeda Hajra Batool (2023). Overcoming the Cycle of Mood and Obesity: Metformin’s Prospective Contribution. Dinkum Journal of Medical Innovations, 2(09):345-365.
- Zhou, C., Zhao, Y., & Li, Y. (2022). Clinical Analysis of Factors Influencing the Development of Placenta Praevia and Perinatal Outcomes in First-Time Pregnant Patients. Frontiers in Surgery, 9, 862655.
- Munir, Shaouki & Biswas, Anirudha & Shakil, Jamil & Mouri, Sadia & Mostafa, Shekh Mohammad & Estoque, Arevalo & Tantong, Alkauzar & Zulfiqar, Rabia. (2024). COMPARISON OF QUALITY ASSURANCE, EMPATHY, AND BURNOUT IN HEALTHCARE PEOPLE SETTINGS: A DESCRIPTIVE STUDY OF PATIENTS AND HEALTHCARE ASSOCIATES. Chinese Science Bulletin (Chinese Version). 69. 1267-1276.
- Bartels, H. C., Mulligan, K. M., Lalor, J. G., Higgins, M. F., & Brennan, D. J. (2020). A life changing experience: an interpretative phenomenological analysis of women’s experiences of placenta accreta spectrum. European Journal of Obstetrics & Gynecology and Reproductive Biology, 254, 102-108.
- Suanada Agarwal & Pilar Matud Zee (2023). Sexual Orientation and Psychological Wellness in Women; Psychoanalytic Book Review. Dinkum Journal of Medical Innovations, 2(09):366-369.
- Kashanian, M., Eshraghi, N., Babaei, M. R., Mohammadian‐amiri, M., Ghaemi, M., Aklamli, M., & Eshraghi, N. (2024). Conservative management of placenta previa‐percreta with bladder invasion: A case report. Clinical Case Reports, 12(5), e8879.
- Dane, C., Kizildag, E., Güleç, S., & Dane, B. (2023). Five cases of placenta previa accreta: the maternal and fetal outcome from a tertiary center. EGO European Gynecology and Obstetrics, 5(1), 24-27.
- Gu, Y., Zhou, Y., Li, L., Li, H., Wang, S., Wang, Y., & Zuo, C. (2022). Cook Cervical Ripening Balloon for placenta accreta spectrum disorders with placenta previa: a novel approach to uterus preserving. Archives of Gynecology and Obstetrics, 306(6), 1979-1987.
- Prabin Acharya & Prachi Bhattarai (2023). Perinatal Mortality Rate in South-Asian Countries: A Systematic Review. Dinkum Journal of Medical Innovations, 2(10):418-425.
- Khanday, Zahid & Pantha, Parkash & Pervez, Ayesha & Magdi, Fatma & Mostafa, Mohammad & Hossain, Md. Abul & Tinny, Sejuti Sarker & Zulfiqar, Rabia. (2024). A SYSTEMATIC ANALYSIS OF ROLE OF ARTIFICIAL INTELLIGENCE IN MEDICAL IMAGING: IMPACTS AND THREATS ON RARE DISEASE COMMUNITY. Kokuritsu Iyakuhin Shokuhin Eisei Kenkyūjo hōkoku = Bulletin of National Institute of Health Sciences. 142. 3627-3637.
- Pan, W., Chen, J., Zou, Y., Yang, K., Liu, Q., Sun, M., … & Wang, Z. (2023). Uterus-preserving surgical management of placenta accreta spectrum disorder: a large retrospective study. BMC Pregnancy and Childbirth, 23(1), 615.
- Shegekar, T., & Pajai, S. (2023). A Comprehensive Review of Pregnancy in Sickle Cell Disease. Cureus, 15(6).
- Elitaningrum, P. C., & Prasetyo, B. (2024). Understanding the complex interplay: An in-depth literature review of anemia’s impact on maternal and fetal health throughout pregnancy.
- Swart, T., Shandley, K., Huynh, M., Brown, C. M., Austin, D. W., & Bhowmik, J. (2023). Pregnancy complications and their association with postpartum depression symptoms: a retrospective study. Australian journal of psychology, 75(1), 2247088.
- Ishibashi, H., Miyamoto, M., Shinmoto, H., Soga, S., Matsuura, H., Kakimoto, S., … & Takano, M. (2021). The Use of Magnetic Resonance Imaging to Predict Placenta Previa With Placenta Accreta Spectrum. Obstetric Anesthesia Digest, 41(3), 137-138.
- Zulfiqar, Rabia & Khuwaja, Iqra & Hussain, Syed & Bhuiyan, Mst. Dil Afroz & Shazu, Shahazaman & Ijaz, Hafiza & Akinbode, Akeem Opeyemi & Naser, Maryam & Kareem, Hawraa. (2023). ARTIFICIAL INTELLIGENCE AS A DIAGNOSTIC TOOL IN MEDICINE AND COMMUNITY DENTISTRY: A SYSTEMATIC LITERATURE REVIEW. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 54. 1253-1264.
- Greenwood, L., Mastrobattista, J., Mack, L., Fox, K., Lee, W., & Donepudi, R. (2023). Impact of Pelvic Rest Recommendations on Follow‐Up and Resolution of Placenta Previa and Low‐Lying Placenta. Journal of Ultrasound in Medicine, 42(9), 2023-2030.
- Pathiraja, P. D. M., & Jayawardane, A. (2021). Evaluation of peripartum hysterectomy in a tertiary care unit and its effect on patients’ long-term physical and mental wellbeing: quest is not over when you save the life. Obstetrics and Gynecology International, 2021, 1-8.
- Carusi, D. A., Duzyj, C. M., Hecht, J. L., Butwick, A. J., Barrett, J., Holt, R., … & Shainker, S. A. (2023). Knowledge gaps in placenta accreta spectrum. American Journal of Perinatology, 40(09), 962-969.
- Qi, T., Cohen, A., Miguel, C., Peskin-Stolze, M., & Doulaveris, G. (2024). 291 Association of resolving placenta previa and other early sonographic markers with postpartum hemorrhage. American Journal of Obstetrics & Gynecology, 230(1), S167-S168.
- Agrawal, M., Reddy, L. S., Patel, D., Jyotsna, G., Patel, A., srivani Reddy, L., & Patel Jr, A. (2024). Fetal Reduction by Potassium Chloride Infusion in Unruptured Heterotopic Pregnancy: A Comprehensive Review. Cureus, 16(2).
- Zhou, Y., Song, Z., Wang, X., Zhang, M., Chen, X., & Zhang, D. (2022). Ultrasound-based nomogram for postpartum hemorrhage prediction in pernicious placenta previa. Frontiers in Physiology, 13, 982080.
- Tang, W., Zhou, L. J., Zhang, W. Q., Jia, Y. J., Hu, F. H., & Chen, H. L. (2023). Adverse perinatal pregnancy outcomes in women with schizophrenia: A systematic review and meta-analysis. Schizophrenia Research, 262, 156-167.
- Wang, L. J., Fan, D. Z., Guo, H. X., Chen, B. S., & Liu, Z. P. (2022). Weight gain during pregnancy and placenta morphology: a prospective cohort study. European Review for Medical and Pharmacological Sciences, 26(6), 1978-1983.
- Zhao, H., Wang, Q., Han, M., & Xiao, X. (2023). Current state of interventional procedures to treat pernicious placenta previa accompanied by placenta accreta spectrum: A review. Medicine, 102(37), e34770.
- Wu, Y., Zhang, C., Liu, H., Duan, C., Li, C., Fan, J., … & Huang, H. F. (2020). Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. American journal of obstetrics and gynecology, 223(2), 240-e1.
Publication History
Submitted: January 24, 2024
Accepted: February 13, 2024
Published: February 29, 2024
Identification
D-0249
DOI
https://doi.org/10.71017/djmi.3.2.d-0249
Citation
Ms. Saroja Poudel & Dr. Rajesh Niraula (2024). Comprehensive study of Placenta Previa & Its Psychological Consequences. Dinkum Journal of Medical Innovations, 3(02):174-187.
Copyright
© 2024 DJMI. All rights reserved