

")
Publication History
Submitted: January 24, 2024
Accepted: February 13, 2024
Published: February 29, 2024
Identification
D-0250
DOI
https://doi.org/10.71017/djmi.3.2.d-0250
Citation
Dr. Sujan Pradhan, Dr. Sabi Rana, Dr. Property Bhandari, Dr. Ozone Shrestha & Dr. Pranjal Shrestha (2024). The Correlation of Hearing Loss with Site & Size in Tympanic Membrane Perforation. Dinkum Journal of Medical Innovations, 3(02):188-198.
Copyright
© 2024 DJMI. All rights reserved
188-198
The Correlation of Hearing Loss with Site & Size in Tympanic Membrane PerforationOriginal Article
Dr. Sujan Pradhan 1 *, Dr. Sabi Rana 2, Dr. Property Bhandari 3, Dr. Ozone Shrestha 4, Dr. Pranjal Shrestha 5
- Consultant Otolaryngologist, Samata Hospital. Kathmandu, Nepal.
- Department of ENT and HNS, Kulhudhuffushi Regional Hospital, Maldives.
- Otolaryngologist, HAMS Hospital, Kathmandu, Nepal.
- Pathologist, National Path Lab, Kailali, Nepal.
- Bachelor of Medicine & Bachelor of Surgery (MBBS), Tribhuvan University, Kathmandu, Nepal.
* Correspondence: sujanp122@gmail.com
Abstract: Chronic Otitis Media (COM) is one of the commonest ear disease and important cause of hearing disability. There is chronic infection of the middle ear cleft, in which a non-intact tympanic membrane and discharge are present. Perforation occurring as a result of chronic otitis media leads to significant conductive hearing loss. This study correlate the degree of hearing loss with site and size in tympanic membrane perforation. A cross-sectional study was conducted at Kathmandu Medical College Teaching Hospital, ENT-HNS department. A total of N=87 patients of both gender and age between 15 to 55 years with COM – mucosal inactive type were included in the study. Site and size of tympanic membrane (TM) perforation was assessed using otoscope and otomicroscope. Size of perforation was measured with 27G spinal needle blunted and bent in different calibrations using a measuring tape and size was calculated using the formula. Patients were divided into three groups according to size; Group I (0-9 mm2), Group II (10-29 mm2), Group III (≥30 mm2). The TM was divided into five segments anterosuperior, posterosuperior, anteroinferior, posteroinferior and subtotal for the localization of the site of perforation. Data thus collected was statistically analyzed. Patients with Group I perforation had an average hearing loss of 31.22 ± 7.53 decibel (dB). Group II had an average hearing loss of 42.76 ± 8.27 dB. Group III had an average hearing loss of 62.5 ± 2.88 dB. Maximum hearing loss was noted in patients with subtotal perforation with an average hearing loss of 47.97 ± 9.05 dB. Average hearing loss was found to be higher in posterior quadrant perforations than in anterior quadrant perforations. This difference was statistically significant with “p” value of “0.031”. The larger the size of the perforation, the greater the degree of hearing loss. The degree of hearing loss is also influenced by the site of the perforation on the TM, as posterior quadrant perforations have a greater degree of hearing loss than anterior quadrant perforations.
Keywords: Chronic otitis media, Hearing loss, Perforation, Tympanic membrane
- INTRODUCTION
The condition known as Chronic Otitis Media (COM) is one of the most frequent types of ear illness that an otologist would see in underdeveloped countries. To put it simply, Chronic Otitis Media (COM) is one of the most prevalent ear diseases and a significant contributor to hearing impairment in Nepal [1]. A stage of ear disease in which there is a chronic infection of the middle ear cleft which includes the Eustachian Tube, middle ear, and mastoid, in which a nonintact tympanic membrane (for example, perforation or tympanostomy tube) and discharge (otorrhea) are present [2]. It is quite probable that it is the consequence of an earlier acute case of otitis media, a negative middle ear pressure, or otitis media featuring effusion [3]. Infectious, allergy, environmental, socioeconomic, racial, and tubal dysfunction are some of the factors that contribute to the etiology and pathogenesis of chronic obstructive pulmonary disease. It has been hypothesized that the widespread incidence of COM in underdeveloped nations can be attributed to a combination of factors, including poor living circumstances, overcrowding, inadequate cleanliness, and inadequate nutrition [4]. In at least 0.5 percent of the population, perforation is a complication that arises as a consequence of chronic otitis media [5]. The prevalence of deafness was 16.6% in the age range starting at five years old and older. There were 15,845 patients who participated in the survey, and 7.2% of them had chronic suppurative otitis media (CSOM) of the tubo-tympanic type, whereas 0.9% had CSOM of the attico-antral type [6]. It also demonstrated that CSOM was responsible for approximately one-third of the preventable cases of deafness, the former terminology of Chronic Suppurative Otitis Media, which was referred to as tubo-tympanic (TT) and attico-antral (AA), has been abandoned and has been replaced with the terms mucosal and squamous, respectively [7]. Due to the fact that difficulties can arise in every case with active COM regardless of the pathophysiology, the words “safe” and “unsafe” are deceptive. A permanent hole of the pars tensa is one of the characteristics of the inactive mucosal COM, which is the third type of COM [8]. However, the mucosa of the middle ear is not associated with inflammation, remnant of the pars tensa, tympanosclerosis, a dimeric membrane, or a thick scar may surround the perforation [9]. In active mucosal chronic otitis media (COM), there is chronic inflammation within the mucosa of the middle ear and mastoid, along with varying degrees of edema, submucosal fibrosis, hypervascularity, and an inflammatory infiltrate [10]. Additionally, there is an increase in the number of goblet cells and basal cell hyperplasia in the middle ear epithelium, which leads to the production of mucopurulent discharge that drains through a tympanic membrane (TM) perforation [11]. Active COM is typically characterized by the degradation of the ossicular chain. In adults, the most prevalent manifestations of COM are hearing impairment, which occurs in around 80 percent of cases, and ear discharge, which occurs in approximately 70 percent of cases [12]. In order to allow sound to fall directly on the middle ear, perforation of the TM reduces the surface area of the membrane that is available for sound transmission [13]. As the temperature difference between the inner and outer surfaces of the TM decreases, the pressure gradient between them becomes unimportant [14]. A decrease in the differential in sound pressure across the TM is the consequence of this, which leads to a reduction in the ossicular coupling. Due to the fact that the sound pressure difference across the TM is the primary driving force behind the motion of the drum and ossicle, perforation in the TM reduces the effectiveness with which the TM transmits the sound waves to the ossicular chain [15]. This results in a conductive type of hearing loss that can range from being negligible to fifty decibels. The closure of the perforation requires surgical intervention in order to be successful. Myringoplasty and tympanoplasty are the surgical treatments that must be performed in order to treat COM mucosal type inflammation [16]. The extent to which COM mucosal patients experience an improvement in their hearing after surgery is contingent upon a number of parameters, including the location and size of the perforation, the ossicular condition, the surgical method, the type of graft, and the function of ET [17]. In order for doctors to have a better understanding of the severity and frequency of hearing loss that can be the result of holes of varying sizes and locations, there is a need for a more detailed description of the effects that perforations have on the function of the middle ear [18]. When clinicians get access to such information, they will be able to determine whether the hearing loss is entirely the result of a perforation or whether there are other pathologies that are contributing to the hearing loss [19]. Chronic Otitis Media (COM) is a chronic inflammation of the mucoperiosteal lining of a part or whole of the middle ear cleft. This inflammation can result in long-term or, more frequently, permanent changes in the tympanic membrane. These changes can include atelectasis, dimer formation, perforation, tympanosclerosis, retraction pocket development, or cholesteatoma [20].
- MATERIALS AND METHODS
The study follow the cross-sectional study design conducted in the department of Otorhinolaryngology and Head and neck surgery, Kathmandu Medical College and teaching hospital, Sinamangal. Convenient sampling technique has been used where Sample size (N) has been calculated using following formula:
where
n = sample size
z = 1.96
= prevalence of TM perforation12
= 1-p
e = allowable error
n= n = 87
Hence sample size is 87, proforma, Otoscope, Pure tone audiometer (GSI Pello), Microscope (ZEISS), 27G spinal needle, measuring tape. All the patients with TM perforation from the age 15 to 55 years were included in the study. Detailed history and clinical examination of the ear, nose and throat was done. Based on the duration of disease patient were divided in to three groups: Group A (>1 year), Group B (1–5 years), Group C (> 5 years). Otoscopic examination was done to determine the site of TM perforation. The site of perforation was drawn in the TM diagram present in the proforma and was confirmed by respected registered MS ENT-HNS surgeons. On the basis of the quadrant/s of the TM, the site of perforation was divided into antero-superior (AS), postero-superior (PS), antero-inferior (AI), posteroinferior (PI) and subtotal (involving all four quadrants mentioned above). On the basis of perforation in relation to the handle of the malleus, the site was also divided into anterior, posterior, and combined (involving both anterior and posterior perforation) perforation groups. The data collected and entered in the SPSS Version 20 for analysis. Percentage, mean and standard deviation of all was calculated.
- RESULTS AND DISCUSSION
3.1 Demographic Profiling
The total number of the patients enrolled in the study was 87, who presented with inactive mucosal disease with conductive hearing loss after considering all exclusion criteria as mentioned above. The age of the patients in this study, ranged from ≥15 years to ≤ 55 years of age. Out of these, patients with age group of 15 to 24 years were 23 (26.4%), of 25 to 34 years were 37 (42.5%), of 35 to 44 years were 12 (13.8%), of 45 to 54 years were 15. (17.2%). Out of 87 patients in the study, 49 (56.3%) were male and 38 (43.7%) were female. Of the 87 patients included in this study, 46 (52.8%) belonged to the rural community, while 41 (47.2%) belonged to the urban community. Out of 87 patients, left ear was involved in 48(55.2%) patients and right ear was involved in 39(44.8%) patients.
Table 01: Showing demographic profile of the patients participated
| Age | Range (mean ± SD) | 31.34 ± 9.68 |
| Gender | Male
Female |
49
38 |
| Geography | Urban
Rural |
41
46 |
| Ear involved | Right
Left |
39
48 |
3.2 Chief complaints
Out of 87 patients, 53 patients presented with chief complaints of otorrhea with hearing loss, 27 patients presented with otorrhea, and 6 patients presented with hearing loss as their chief complaint, whereas 1 patient presented with otorrhea with otalgia as their chief complaints.
Table 02: Distribution of patients based on chief complaint/s
| CHIEF COMPLAINT/S | NO. OF PATIENTS |
| Otorrhea | 27 |
| Otorrhea with hearing loss | 53 |
| Hearing loss | 6 |
| Otorrhea with otalgia | 1 |
3.3 Duration of disease
Among 87 patients, 23 (26.4%) patients (Group A) had the disease for less than 1 year, 38 (43.7%) patients (Group B) had disease in the range of 1–5 years, and 26 (29.9%) patients (Group C) had disease for more than 5 years.
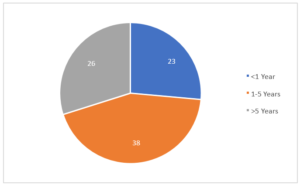
Figure 01: Distribution of patients based on duration of disease
3.4 Duration of disease and hearing loss
The mean hearing loss in patients (Group A) with duration of disease less than 1 year was found to be 33.09 ± 6.25 (dB), in patients (Group B) with duration of disease between 1 to 5 year was 38.66 ± 10.6 (dB) and in patients (Group C) with duration of disease more than 5 year was 47.23 ± 10.51 (dB).
Table 03: Duration of disease and mean hearing loss
| DURATION | HEARING LOSS (Mean ± SD) dB |
| <1 year (Group A) | 33.09 ± 6.25 |
| 1-5 years (Group B) | 38.66 ± 10.6 |
| >5 years (Group C) | 47.23 ± 10.51 |
Using one-way ANOVA (F 2,84 = 13.596, p < 0.001), the observed difference was shown to be statistically significant. The longer the duration of the disease, the greater the hearing loss.
Table 04: Showing relationship between duration of disease and mean hearing loss (ANOVA)
| Sources | Sum of Squares | df | Mean Square | F | P – value |
| Between groups | 2521.443 | 2 | 2521.443 | 13.596 | <0.001* |
| Within groups | 7788.994 | 84 | 7788.994 | ||
| Total | 10310.437 | 86 |
*Significant at p- value<0.05
3.5 Tuning Fork Test and interpretation
On the tuning fork test, Rinne’s test was negative in all diseased ears, i.e., 87 (100%) patients. The Weber’s test was lateralized to the worse ear in 85 (97.7%) patients, while (2.3%) patients had indeterminate Weber’s tests. The Absolute bone conduction (ABC) test revealed all 87 (100%) patients had heard the tuning fork for the same duration as the examiner.
Table 05: Tuning fork test and interpretation
| TUNING FORK
TEST |
INTERPRETATION | NO. OF PATIENTS |
| Rinne
|
Positive Negative | –
87 (100%) |
| Weber | Lateralized to disease ear Not lateralized to disease ear | 85 (97.7 %)
2 (2.3%) |
| Absolute bone conduction | Same duration Shorter duration | 87 (100%)
– |
3.6 Site of perforation
Among 87 patients, each of 6 (6.9%) patients had perforation involving the anterosuperior (AS), antero-inferior (AI), and postero-superior (PS) quadrants, 8 (9.2%) patients had perforation involving the postero-inferior (PI) quadrant, and 30 (34.5%) patients had subtotal perforation. The remaining 18 (35.6%) patients had perforations involving two quadrants of the TM, among which 5 (5.7%) patients had AS and AI quadrant involvement, 8 (9.2%) patients had PS and PI quadrant involvement, and 18 (20.7%) patients had AI and PI quadrant involvement.
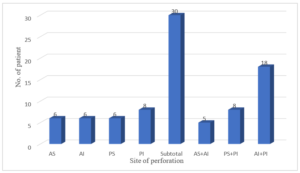
Figure 02: Distribution of patients based on site of perforation
Among 87 patients, 17 (19.5%) had perforation present in the anterior quadrant, 22 (25.3%) had perforation present in the posterior quadrant, and 48 (55.2%) patients had perforation involving both the anterior and posterior quadrants (combined).
Table 06: Distribution of patients based on site of perforation
| SITE OF PERFORATION | NO. OF PATIENTS |
| Anterior | 17 (19.5%) |
| Posterior | 22 (25.3%) |
| Combined | 48 (55.2%) |
3.6 Hearing Loss according to site of perforation
The mean hearing loss (dB) was found to be 28.67 ± 2.87, 26.17 ± 0.75, 32.33 ± 6.65 and 37.13 ± 13.65 for patients who had perforation involving AS, AI, PS and PI quadrant respectively. Patients who presented with subtotal perforation had mean hearing loss of 47.97 ± 9.05 dB. The mean hearing loss in patients who had perforation involving the AS + AI quadrant was found to be 34.00 ± 4.00 dB. Patients with perforation involving the PS + PI quadrants had mean hearing loss of 40.87 ± 10.30 dB, whereas patients with AI + PI quadrant perforation had a mean hearing of 39.00 ± 8.11 dB.
Table 07: Site of perforation and mean hearing loss
| SITE OF PERFORATION | HEARING LOSS (Mean ± SD) dB |
| AS | 28.67 ± 2.87 |
| AI | 26.17 ± 0.75 |
| PS | 32.33 ± 6.65 |
| PI | 37.13 ± 13.65 |
| Subtotal | 47.97 ± 9.05 |
| AS + AI | 34.00 ± 4.00 |
| PS + PI | 40.87 ± 10.30 |
| AI + PI | 39.00 ± 8.11 |
The mean hearing loss was found to be 29.35 ± 4.18 dB in patients who had perforation involving the anterior quadrant, 37.18 ± 10.95 dB in patients who had perforation involving the posterior quadrant. Patients with combined perforation had mean hearing loss of 44.60 ± 9.67 dB, which was highest among the group.
Table 08: Site of perforation and mean hearing loss
| SITE OF PERFORATION | HEARING LOSS (Mean ± SD) dB |
| Anterior | 29.35 ± 4.18 |
| Posterior | 37.18 ± 10.95 |
| Combined | 44.60 ± 9.67 |
The difference between groups as determined by one-way ANOVA (F 2,84 = 18.172, p < 0.001) was statistically significant.
Table 09: Showing relationship between site of perforation and mean hearing loss (ANOVA)
| Sources | Sum of Squares | df | Mean Square | F | P – value |
| Between groups | 4898.325 | 2 | 2449.163 | 18.172 | <0.001* |
| Within groups | 5412.112 | 84 | 64.430 | ||
| Total | 10310.437 | 86 |
*Significant at p- value<0.05
A Bonferroni’s post hoc test revealed that hearing loss was statistically significant when each site of perforation was compared to one another (p < 0.05).
Table 10: Showing relationship between different sites of perforation and mean hearing loss
| Groups | P – value |
| Anterior VS Posterior | 0.031* |
| Anterior VS Combined | 0.000* |
| Posterior VS Combined | 0.008* |
*Significant at p-value <0.05
3.7 Size of perforation
Out of 87 patients, 31 (35.6%) had a perforation of size belonging to group I (0-9 mm2), 52 (59.8%) had a perforation of size belonging to group II (10-29 mm2) and 4 had a perforation of size belonging to group III (≥ 30 mm2).
Table 11: Distribution of patients based on size of perforation
| 3.1 Demographic Profiling | 3.1 Demographic Profiling |
| Group I (0-9 mm2) | 31 (35.6%) |
| Group II (10-29 mm2) | 52 (59.8%) |
| Group III (≥ 30 mm2) | 4 (4.6%) |
3.8 Hearing Loss according to size of perforation
The mean hearing loss in patients with a perforation size of group I (0-9 mm2) was 31.22 ± 7.53 dB, 42.76 ± 8.27 dB in patients with a perforation size of group II (10-29 mm2), and 62.5 ± 2.88 dB in patients with a perforation size of group III (≥30 mm2), which was the highest among the groups.
Table 12: Size of perforation and mean hearing loss
| SIZE OF PERFORATION | HEARING LOSS (Mean ± SD) dB |
| Group I (0-9 mm2) | 31.22 ± 7.53 |
| Group II (10-29 mm2) | 42.76 ± 8.27 |
| Group III (≥ 30 mm2) | 62.5 ± 2.88 |
A spearman’s rank order correlation was used to determine the relationship between hearing loss and size of perforation. There was a strong positive correlation between hearing loss and size of perforation, which was statistically significant (SR85 = 0.68, p < 0.001). There was a statistically significant difference between degree of hearing loss and size of perforation, as determined by one-way ANOVA (F 2,84 = 38.013, p < 0.001).
Table 13: Showing relationship between size of perforation and mean hearing loss (ANOVA)
| Sources | Sum of Squares | df | Mean Square | F | P – value |
| Between groups | 3113.803 | 2 | 1556.901 | 18.172 | <0.001* |
| Within groups | 7196.634 | 84 | 85.674 | ||
| Total | 10310.437 | 86 |
*Significant at p- value<0.05
A Bonferroni’s post hoc test revealed a statistically significant difference between all three groups when compared to one another (p < 0.001).
Table 14: Showing relationship between different sizes of perforation and mean hearing loss
| Groups | P – value |
| Group I VS Group II | <0.001 * |
| Group I VS Group III | <0.001 * |
| Group II VS Group III | <0.001 * |
*Significant at p-value <0.05
3.9 Discussion
This study aimed to connect hearing loss with TM perforation site and size, it covered conductive hearing-loss chronic otitis media-mucosal inactive individuals. The most common age group in this study was 25–34 years, with 37 (43%) patients, followed by 15–24 years, with 23 (26%) individuals. The average age of presentation was 31.34 ± 9.68 years for males and 30.32 ± 9.94 years for females. A study found that out of 700 patients, 86.71 percent fell between the 10-40 age category, with a mean age of 31.56 ± 7.85 years for males and 28.67 ± 9.40 for females. This finding was similar to the present study, maybe because patients are becoming more socially and professionally aware of their hearing at this age [21]. Out of 87 patients, 49 (56%) were male and 38 (44%) were female, with a 1.3:1 male-female ratio and slight male predominance. In a study 52 patients (52%) were male and 48 (48%) were female, resulting in a 1.14:1 male-to-female ratio, results were similar to the present study, maybe because in our society, men are still more involved in social and professional contexts than women [22]. Most chronic suppurative otitis media patients were rural, similarly, comparable study found that CSOM was lower in Kathmandu schoolchildren than in rural Nepal [23]. This may be due to illiteracy, poor sanitation, inadequate hygiene, and a lack of effective health facilities in rural areas. These factors led to a higher illness prevalence in rural areas [24]. In this study, 42 (48.2%) of 87 patients had left ear disease, 34 (39.1%) had right ear illness, and 11 (12.7%) had bilateral ear disease. Most patients reported recurring otorrhea and hearing loss, although one patient presented with otorrhea and otalgia due to COM and superimposed otitis externa [25]. Similar to the present study, [26] found that ear discharge length affects hearing loss. The longer the ear discharge, the higher the hearing loss. With a p-value of 0.023.4, ear discharge duration was associated with hearing loss. In contrast, it observed no link between disease duration and hearing loss (p-value >0.05). The tuning fork test showed a negative Rinne test in all 87 individuals. 85 patients had the Weber test lateralized to the afflicted ear. Two patients had no Weber test lateralization to the afflicted ear, possibly because both ears had similar hearing loss [27]. The study indicated that individuals with mixed perforation had the largest mean hearing loss (44.60 ± 9.67dB) compared to those with only anterior or posterior perforation, based on the position of perforation in reference to the malleus handle. Analysis revealed a substantial difference (p<0.001). Patients with posterior perforation had a higher mean hearing loss (37.18 ± 10.95dB) compared to those with anterior perforation (29.35 ± 4.18dB). The difference in hearing loss was statistically significant (p<0.031) [28]. A study found that posterior perforations result in greater hearing loss than anterior ones (p<0.05). The present investigation found comparable outcomes [29]. Like the present study, a study found that postero-inferior perforations cause higher hearing loss than antero-inferior ones. This is likely due to circular window exposure and ossicular fixation. Postero-inferior perforations remove the round window’s sound shielding, causing higher hearing loss than other quadrants [30]. A study found higher hearing loss in the posterior quadrant. Comparison of perforation site and hearing loss indicated statistical significance (p=0.047) [31]. Similar findings to this study may be attributable to removal of the “round window baffle” on hearing threshold. Recent models on sound energy transmission through TM into the middle ear reveal that this may not be the primary cause due to the complicated way of sound transmission over the middle ear. It discovered no changes in round window and oval window pressures for similar-sized TM perforations at different sites, indicating that hearing loss was unaffected by the site [32].
- CONCLUSIONS
Over time, chronic otitis media (COM) has become one of the most prevalent ear diseases and a significant contributor to hearing impairment. There is a persistent infection of the middle ear cleft, which is characterized by the presence of a tympanic membrane that is partially detached and discharge. A considerable amount of conductive hearing loss is the result of perforation that occurs as a consequence of chronic otitis media. It is necessary for doctors to have a better understanding of the effect that perforations have on the function of the middle ear in order for them to be able to predict the severity and frequency of hearing loss that is associated with perforations associated with different sizes and locations. This study determined the correlation of hearing loss with site & size in Tympanic Membrane Perforation. The ENT-HNS department of Kathmandu Medical College Teaching Hospital was the location of a cross-sectional study that was carried out. The study comprised a total of 87 patients with COM – mucosal inactive type. These patients ranged in age from 15 to 55 years old and could be either male or female. The results shown that average hearing loss among patients who had Group I perforation was 31.22 decibels (dB), with a standard deviation of 7.53 dB. Group II had an average hearing loss of 42.76 decibels, with a standard deviation of 8.27 decibels. Group III had an average hearing loss of 62.5 decibels, with a standard deviation of 2.88 decibels. Patients with subtotal perforation caused the greatest amount of hearing loss, with an average hearing loss of 47.97 decibels (± 9.05 decibels). When compared to perforations in the anterior quadrant, it was discovered that the average hearing loss was greater in the posterior quadrant with perforations. The “p” value for this difference was “0.031,” which indicates that it was statistically significant. The severity of the hearing loss is proportional to the size of the perforation, which makes the perforation larger. Perforations in the posterior quadrant of the TM are associated with a greater degree of hearing loss than those in the anterior quadrant of the TM. This is because the placement of the perforation on the TM is another factor that factors into the degree of hearing loss.
REFERENCES
- Kolluru, K., Kumar, S., & Upadhyay, P. (2021). A study of correlation between tympanic membrane perforation size with hearing loss in patients with inactive mucosal chronic otitis media. Otology & Neurotology, 42(1), e40-e44.
- Bukhari, Saima & Attar, Meshari & Khalid, Amna & Riaz, Mariam & Khalid, Henna & Saad, Ammar & Zulfiqar, Rabia. (2024). EVALUATION OF HEPATIC, RENAL AND HEMATOLOGIC PARAMETERS IN PATIENTS ON LONG-TERM LOW-DOSE METHOTREXATE THERAPY IN RHEUMATOID ARTHRITIS. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1439-1446.
- Nahal Mostak Khan, Soheb Ahmed Robin, Lutfullahil Khabir & Sohel Mahmud (2023). Role of Vitamin C in Development of Age Related Cataract. Dinkum Journal of Medical Innovations, 2(12):515-523.
- Basheer, H. M. U., Ikram, A., & Hanif, A. (2023). Degree of Hearing Loss in Association with Site of Tympanic Membrane Perforation: A Systematic Review. Pakistan Journal of Medical & Health Sciences, 17(01), 2-2.
- Riaz, Mariam & Javed, Maham & Bukhari, Saima & Shaheen, Faiza & Khan, Tariq & Khalid, Henna & Zulfiqar, Rabia. (2024). BLOODSTREAM INFECTIONS AND TRENDS OF ANTIMICROBIAL SENSITIVITY PATTERN: A LABORATORY BASED STUDY. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 55. 1421-1428.
- Asbin Bandhari, Syeda Hajra Batool, Aatiqa Tariq, Abdullah Hassan, Pooja Bhanarjee & Parshu Ram (2023). A Comprehensive Analysis of Neurosurgeons’ Conversations to Preserve Non-Traditional Brain Networks. Dinkum Journal of Medical Innovations, 2(06):207-216.
- Zahra, Musarrat & Bukhari, Saima & Khan, Tariq & Zakir, Afsheen & Munshi, Muhammad & Mehnaz, Gul & Zulfiqar, Rabia. (2024). Comparative Analysis Of Incidence Of Non-Opioid Analgesic Self-Medication Practice Among Health Associates. Journal of Population Therapeutics and Clinical Pharmacology. 31. 1649-1656. 10.53555/jptcp.v31i4.5980.
- Castelhano, L., Correia, F., Colaço, T., Reis, L., & Escada, P. (2022). Tympanic membrane perforations: the importance of etiology, size and location. European Archives of Oto-Rhino-Laryngology, 279(9), 4325-4333.
- Nabeela Riaz, Rabia Zulfiqar, Muhammad Naveed Akhter & Msooma Sheikh (2023). Dentinogenesis Imperfecta type II Underwent Whole Mouth Rehabilitation Employing Various Treatment Modalities. Dinkum Journal of Medical Innovations, 2(06):201-206.
- Xie, P., Peng, Y., Hu, J., Peng, A., & Yi, S. (2020). Assessment of hearing loss induced by tympanic membrane perforations under blast environment. European archives of oto-rhino-laryngology, 277, 453-461.
- Marie Diack, Derak Stewart, Parshu Kirby & David Moris (2023). Challenges with Parent/Caregiver Medication Administration in Peadiatrics and the Importance of Patient Education: A Systematic Review. Dinkum Journal of Medical Innovations, 2(01):22-28.
- Nafis, A. A. M., Hossan, M. A., Islam, M. A., & Al Mamun, A. (2022). Correlation of Hearing Loss with the Site and Size of Tympanic Membrane Perforation. SAS J Surg, 10, 641-648.
- Khanday, Zahid & Pantha, Parkash & Pervez, Ayesha & Magdi, Fatma & Mostafa, Mohammad & Hossain, Md. Abul & Tinny, Sejuti Sarker & Zulfiqar, Rabia. (2024). A SYSTEMATIC ANALYSIS OF ROLE OF ARTIFICIAL INTELLIGENCE IN MEDICAL IMAGING: IMPACTS AND THREATS ON RARE DISEASE COMMUNITY. Kokuritsu Iyakuhin Shokuhin Eisei Kenkyūjo hōkoku = Bulletin of National Institute of Health Sciences. 142. 3627-3637.
- Peter John, Irina Yang & Aparna Goel (2022). A Systematic Literature Review of Importance of Emotional Competence in Healthcare Management. Dinkum Journal of Medical Innovations, 1(01):19-26.
- Casale, G., Shaffrey, E., & Kesser, B. W. (2020). Correlation between hearing loss and middle ear volume in patients with a tympanic membrane perforation. The Laryngoscope, 130(4), E228-E232.
- Bhiryani, M. A., Panchal, A. J., Kumar, R., Kapadia, P. B., & Mandal, M. M. (2022). A Study to Assess the Effect of Size & Site of Tympanic Membrane Perforation on Hearing Loss. Indian Journal of Otolaryngology and Head & Neck Surgery, 74(Suppl 3), 4460-4466.
- Bhiryani, M. A., Panchal, A. J., Kumar, R., Kapadia, P. B., & Mandal, M. M. (2022). A Study to Assess the Effect of Size & Site of Tympanic Membrane Perforation on Hearing Loss. Indian Journal of Otolaryngology and Head & Neck Surgery, 74(Suppl 3), 4460-4466.
- Nida Ishfaq & Yang Chan (2022). An Analysis of Nutritional Awareness among Diabetic Patients. Dinkum Journal of Medical Innovations, 1(01):13-18.
- Hussain, M., Wasif, M., Awan, M. S., Khalid, S., Sheikh, Z., & Iftikhar, H. (2021). Use of endoscope in teaching of otolaryngology residents about site and size of tympanic membrane perforation and its impact on degree of hearing loss in adult patients: A cross sectional study. JPMA. The Journal of the Pakistan Medical Association, 71(1 (Suppl 1)), S14.
- Khanday, Zahid & Pantha, Parkash & Pervez, Ayesha & Magdi, Fatma & Mostafa, Mohammad & Hossain, Md. Abul & Tinny, Sejuti Sarker & Zulfiqar, Rabia. (2024). A SYSTEMATIC ANALYSIS OF ROLE OF ARTIFICIAL INTELLIGENCE IN MEDICAL IMAGING: IMPACTS AND THREATS ON RARE DISEASE COMMUNITY. Kokuritsu Iyakuhin Shokuhin Eisei Kenkyūjo hōkoku = Bulletin of National Institute of Health Sciences. 142. 3627-3637.
- Kim, Y. H., Lee, D. Y., Lee, D. H., & Oh, S. (2022). Tympanic membrane perforation after intratympanic steroid injection: a systematic review and meta-analysis. Otolaryngology–Head and Neck Surgery, 166(2), 249-259.
- Ghimire, B., Basnet, M., Aryal, G. R., & Shrestha, N. (2022). Tympanic Membrane Perforation among Patients Presenting to Department of Otorhinolaryngology of a Tertiary Care Hospital: A Descriptive Cross-sectional Study. JNMA: Journal of the Nepal Medical Association, 60(247), 246.
- Rasheed, A. M. (2023). Does the Location of a Small Tympanic Membrane Perforation Affect the Dgree of Hearing Loss in Adult Patients with Inactive Mucosal Chronic Suppurative Otitis Media?. The International Tinnitus Journal, 27(2), 135-140.
- Selaimen, F. A., Rosito, L. P. S., Silva, M. N. L., Silva, A. L., Stanham, V. D. S., & Costa, S. S. (2021). Central versus marginal tympanic membrane perforations: does it matter? An analysis of 792 patients. Acta Oto-Laryngologica, 141(2), 122-128.
- Wicaksono, A. B., Samodra, E., Fitriana, M., Trihandoko, F., Khoiria, A. H., & Dewanti, D. A. K. (2022). The influence of tympanic membrane perforation site on the hearing level of conductive hearing loss in chronic suppurative otitis media. Journal of the Medical Sciences (Berkala Ilmu Kedokteran), 54(3).
- Selaimen, F. A., Rosito, L. P. S., da Silva, M. N. L., Stanham, V. D. S., Sperling, N., & da Costa, S. S. (2022). Tympanic membrane perforations: a critical analysis of 1003 ears and proposal of a new classification based on pathogenesis. European Archives of Oto-Rhino-Laryngology, 1-7.
- Jabłońska, J., Pietraś, A., Partycka-Pietrzyk, K., & Mielnik-Niedzielska, G. (2022). HEARING LOSS IN CHILDREN AFTER TYMPANIC MEMBRANE PERFORATION: CLUSTER ANALYSIS OF 27 CASES. Journal of Hearing Science, 12(4).
- Illes, K., Gergő, D., Keresztely, Z., Dembrovszky, F., Fehervari, P., Banvoelgyi, A., … & Horvath, T. (2023). Factors influencing successful reconstruction of tympanic membrane perforations: a systematic review and meta-analysis. European Archives of Oto-Rhino-Laryngology, 280(6), 2639-2652.
- Zulfiqar, Rabia & Khuwaja, Iqra & Hussain, Syed & Bhuiyan, Mst. Dil Afroz & Shazu, Shahazaman & Ijaz, Hafiza & Akinbode, Akeem Opeyemi & Naser, Maryam & Kareem, Hawraa. (2023). ARTIFICIAL INTELLIGENCE AS A DIAGNOSTIC TOOL IN MEDICINE AND COMMUNITY DENTISTRY: A SYSTEMATIC LITERATURE REVIEW. Zhonghua er bi yan hou tou jing wai ke za zhi = Chinese journal of otorhinolaryngology head and neck surgery. 54. 1253-1264.
- Karakuş, M. F., Karakurt, S. E., Çolak, M., & DERE, H. H. (2020). The effect of perforation size and site on graft success and hearing in Cartilage Tympanoplasty with mastoidectomy. Middle Black Sea Journal of Health Science, 6(3), 364-368.
- Bhukar, S., Kumari, M., & Goel, A. Correlation of Size of Tympanic Membrane Perforation & Degree of Hearing Loss and Frequency Specific Hearing Gain Following Tympanoplasty. International Journal of Health Sciences, (III), 7521-7531.
- Motegi, M., Yamamoto, Y., Akutsu, T., Tada, T., Kurihara, S., Takahashi, M. & Kojima, H. (2022). Radiological and audiological prediction for ossicular fixation in chronic otitis media and tympanic membrane perforation. Otology & Neurotology, 43(1), 80-89.
Publication History
Submitted: January 24, 2024
Accepted: February 13, 2024
Published: February 29, 2024
Identification
D-0250
DOI
https://doi.org/10.71017/djmi.3.2.d-0250
Citation
Dr. Sujan Pradhan, Dr. Sabi Rana, Dr. Property Bhandari, Dr. Ozone Shrestha & Dr. Pranjal Shrestha (2024). The Correlation of Hearing Loss with Site & Size in Tympanic Membrane Perforation. Dinkum Journal of Medical Innovations, 3(02):188-198.
Copyright
© 2024 DJMI. All rights reserved