

")
Publication History
Submitted: August 19, 2024
Accepted: August 28, 2024
Published: August 31, 2024
Identification
D-0308
DOI
https://doi.org/10.71017/djmi.3.8.d-0308
Citation
Nujhat Minhaj, Mohasin Mia & Rukhshana Afroz Afrin (2024). Level and Pattern of Cervical Lymph Node Metastasis from Gingivo Buccal Sulcus & Palatal Mucosa of Maxilla in Oral Squamous Cell Carcinoma. Dinkum Journal of Medical Innovations, 3(08):570-580.
Copyright
© 2024 The Author(s).
570-580
Level and Pattern of Cervical Lymph Node Metastasis from Gingivo Buccal Sulcus & Palatal Mucosa of Maxilla in Oral Squamous Cell CarcinomaOriginal Article
Nujhat Minhaj 1*, Mohasin Mia 2, Rukhshana Afroz Afrin 3
- Asst.Registrar, Dhaka Dental College Hospital, Dhaka, Bangladesh.
- Asst.Registrar, Dhaka Dental College Hospital, Dhaka, Bangladesh.
- Asst. Professor, Update Dental College Hospital, Dhaka, Bangladesh.
* Correspondence: nujhat45minhaj@yahoo.com
Abstract: Head and neck cancers (HNCs) represent a serious global health issue, it is estimated that more than 1.4 million new cases of HNC, which include cancers that originate in oral or nasal cavity, nasopharynx, oro-pharynx, hypopharynx, larynx or thyroid gland. The term ‘Oral Cancer’ is used to describe any malignancy that arises from oral tissues and accounts for the largest percentage of malignant head and neck tumours. Oral squamous cell carcinoma in maxilla is quite rare, one of the main positive prognostic factors is the abscence of metastatic cervical lymph node. This study observed the cervical level and pattern of lymph node metastasis from maxillary gingivo buccal sulcus and palatal mucosa in oral squamous cell carcinoma. Analytical cross sectional study was conducted in the Department of Oral & Maxillofacial surgery, Dhaka Dental College Hospital. Histologically confirmed squamous cell carcinoma of maxilla treated with neck dissection (Previously untreated patients) and who were tumour size T1-T4, Lymph node involvement cN0/cN+ (clinically and with sonographic examination). All the findings were included in data collection sheet which were then be analyzed and result were prepared. After collection, data editing and clearing were done manually and prepared for data entry and analysis by using SPSS (statistical package for social science) version 26. After analysis of data it was presented in the form of tables with interpretation. Out of 50 SCC patients, majority of the study patients belonged to the age group of ≥ 61 years (34%) followed by the age group 41- 50 years (30%), 51 – 60 years (30%) and ≤ 40 years (6%). The mean age ± SD: 56.02 ± 10.63 and the age range from 35 year to 80 year. Male female ratio was 1:1. Maximum (42%) of the lesions located in the gingiva buccal sulcus (GBS) followed by GBS + palatal mucosa (34%) and palatal mucosa (12%). Ultrasonographically negative lymph nodes were confirmed by histological examination where 12.90% become positive and 87.10% become negative. Oral squamous cell carcinoma of gingivobuccal sulcus, alveolar mucosa and palatal mucosa of maxilla needs prophylactic neck dissection in case of N0 neck. Most of the cases of anterior maxilla metastasis to jugulodigastric lymph nodes. Ultrasonograph of neck is not only non-invasive investigation, but also needs MRI for proper evaluation.
Keywords: Cervical Lymph Node, Metastasis, Gingivo Buccal Sulcus, Palatal Mucosa
- INTRODUCTION
Head and neck cancers (HNCs) represent a serious global health issue. It is estimated that there were more than 1.4 million new cases of HNC, which include cancers that originate in oral or nasal cavity, nasopharynx, oro-pharynx, hypopharynx, larynx or thyroid gland [1]. The term ‘Oral Cancer’ is used to describe any malignancy that arises from oral tissues and accounts for the largest percentage of malignant head and neck tumours. Globally, oral cancer is the sixth most common cancer [2,3]. It is a major health problem in the Indian sub-continent [4]. The majority (84-97%) of oral malignancies are SCCs. It accounts for 90% of oral cancer in Bangladesh [5]. It is an age related disease and 60% of the patients are over the age of 40 years [6]. Due to lack of pain, OSCC and its precursor lesions are often discovered late or as an incidental finding within the context of a routine (medical) examination [7]. The time of diagnosis, however, significantly influences the prognosis and essentially determines the success of potential therapy. A delayed diagnosis of more than four weeks has a significant influence on the prognosis [8]. In addition to the time of diagnosis and consequently the size of the tumour, the presence of lymph node metastasis in the neck in terms of locoregional spread is the most important prognostic indicator [9]. Cervical lymph node metastases in OSCC, which account for more than 90% of oral malignancies, are common [10]. Lymphatic metastases most often occur in level I and II [11,12]. The high incidence of occult cervical lymph node metastasis of approximately 25% in a clinical N0 case situation underscores the clinical significance and the resulting therapeutic difficulties [13,14,15]. The lymphatic drainage of maxilla is generally predictable and flows via two routes: a) via the submandibular nodal group and then to superior jugular chain or b) via the retropharyngeal plexus and again on to the superior jugular chain. Some recent studies indicate the metastatic risk in maxillary gingival SCC is much higher than expected, and suggest that elective neck dissection (END) should be recommended in patients with cN0 [16].Although factual data for metastasis of SCC of the tongue/ floor of the mouth and the benefits of prophylactic neck dissection have been published [17,18], there are only a few studies concerning the behavior of cervical metastases (CM) of SCC of the maxilla with a reported incidence ranging from 0.5% to 5.0% [19,20]. Upper gingival-buccal cancers (UGBCs) are biologically more aggressive than lower gingival-buccal cancers, which have a comparatively better disease-free survival even in advanced stages [21]. The aggressive behavior is possibly because of late presentation of UGBC and early invasion of the infratemporal fossa [22]. But it is striking that the incidence of cervical lymph node metastasis from cancer of the maxilla is significant [23,24]. In the context of Head and Neck Squamous Cell Carcinoma (HNSCC), intratumoral and peritumoral lymphangiogenesis has been correlated with lymph node metastasis [25]. The exact role of the regional lymph node system in the spread of HNSCC has yet to be fully defined, although it is established that they are not simple mechanical barriers, but are involved in conferring anti-tumour immunity, primarily through cytotoxic T-lymphocytes [26]. Prognosis of patients with maxillary GBS & palatal mucosal squamous cell carcinoma is difficult to predict, despite the diagnosis and therapeutic progress in the field of oncology. Even now, half of the patients afflicted, will die within the first two years of diagnosis [27]. There are various factors that influence prognosis, such as, patient factors (age, sex etc.) and tumour factors (site, size, histopathological grade and metastasis). Among all factors the development of lymphatic metastasis is considered as the single most important factor influencing the outcome of the patient with OSCC. The five-year survival rate of patients with squamous cell carcinoma of the upper digestive tract is reduced by almost 50% with the development of cervical metastasis [27]. The number, size, and location of positive cervical lymph nodes define the N stage for HNSCC and provide important information regarding prognosis and selection of treatment [28]. The number of cervical lymph nodes histologically positive for SCC provides one of the simplest, and perhaps most important, prognostic markers in head and neck cancer [28]. Lymph node number exhibit a strong dose–response correlation with distant metastasis and survival [29].On the other hand, extra nodal extension (ENE) occurs in roughly 60% of patients with positive cervical nodes and is of paramount importance in predicting patient outcomes. So the presence of ENE also increases the risk of distant metastatic disease [30]. In addition, it is a significant predictor of poor disease-free, cause- specific, and overall survival [31]. The presence of ENE conferred the highest risk of death, resulting in a sixfold increased risk of death when compared with node-negative patients. In contrast, patients with positive nodes but no ENE experienced a threefold increased risk of death [32].The presence of nodal metastasis independently decreased 5-year survival by more than 50% and nearly doubled the rate of distant metastasis [32]. As the high incidence rate of cervical metastasis in squamous cell carcinoma of the oral cavity is a strong argument in favour of an elective treatment of the ipsilateral side of the neck, no consensus has yet been reached on the need for contralateral neck dissection or radiotherapy. Implications of such treatment on the contralateral side include the advantage of treating subclinical disease on one hand, but on the other hand, as they have a poor prognosis, treatment may lead to a significant increase in morbidity and even mortality without improvement [33,34]. Squamous cell carcinomas of anterior two-third of hard palate, maxillary gingivaland maxillary alveolous are rare relative to other oral subsites. Regional metastatic rates and survival benefit demonstrate the value of selective neck dissection over a wait-and-watch approach for maxillary squamous cell carcinomas. So, the results of this study will help us to establish a correlation between tumour staging and lymphnode metastasis and guide the neck dissection for lesions involving maxilla. The aim of this study is to assess the level and pattern of cervical lymph node metastasis in maxillary squamous cell carcinoma both clinically before surgery and histopathologically after surgical intervention. It will help us to find out the relationship between tumour staging and lymph node metastasis and guide the neck dissection for lesions involving maxillary GBS& palatal mucosa.
- MATERIALS & METHODS
This is a Descriptive cross-sectional study, performed at the Department of Oral and Maxillofacial Surgery in Dhaka Dental College and Hospital, Mirpur-14, Dhaka, Bangladesh. Sample size of this study was estimated using the following statistical formula:
n = z2pq / d2
Where,
n = the desired sample size.
z = the standard normal distribution, which is 1.96 at 5% level of significance which corresponds to 95% confidence level.
p (prevalence ) = 5% ( p = 0.05 ) of oral squamous cell carcinoma patient in maxilla
q = ( 1 – p ) = ( 1 – 0.05 )
d = 0.05 which is the degree of accuracy or precision level which is set at 5% of p.
Using above formula the expected sample size:
n = (1.96 )2 × 0.05 ( 1 – 0.05 ) / ( 0.05 )2= 72.9904
So the estimated sample size was 73.
Though it is one year study time, so sample size 50 was convenient, patients who admitted in the Department of Oral & Maxillofacial Surgery, Dhaka Dental College Hospital, as a diagnosed case of oral squamous cell carcinoma of maxilla clinically & histologically was included in the study. Each maxillary bone has the shape of a pyramid, it’s base adjacent to the nasal cavity, apex being the zygomatic process and it’s body constituting the maxillary sinus. The maxilla connects with surrounding facial structures through four processes: alveolar, frontal, zygomatic and palatine. It articulates superiorly with the frontal bone, the zygomatic bone laterally, palatine bone posteriorly and with the upper teeth through the alveolar process inferiorly. Anteriorly, it forms the inferior and lateral borders of the pyriform aperture and articulates with the nasal bones medially at the anterior border of the frontal process. Metastasis is the process whereby primary malignant tumour spreads to form secondary tumour at a distant site discontinuous with the primary tumour. The TNM system for describing the anatomical extent of head and neck cancer is based on the assessment of three components, namely T, the extent of the primary tumour, N, the presence or absence and extent of regional lymph-node metastases and M, the presence or absence of distant metastasis. Two classifications have been described for each head and neck site i.e. cTNM that is evidence acquired before primary treatment and based on information available prior to first definitive treatment. pTNM that is based on evidence acquired before treatment, supplemented or modified by additional information acquired either surgically or pathologically. There are four distinct growth patterns, Initial cancerous deposits in the sub capsular sinus, resulting in replacement of the architecture of the node before extra-capsular spread. Extensive infiltration of metastatic deposits into the lymphatic sinuses, leaving the germinal centers and trabecular intact. Deposition of a malignant embolus within the subcapsular sinus with simultaneous arrest of tumour within capsular or juxtacapsularlymphatics. Capsular or juxtacapsular emboli growth with no intranodal cancer.
- RESULTS & DISCUSSIONS
Figure 01 shows, 50% (25) are male and 50% (25) are female. The male & female ratio is 1:1
Figure 01: Distribution of the patients according to sex. (n=50)
Table 01: Distribution of the patients according to age.
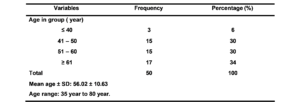
Majority of the study patients belongs to the age group of ≥ 61 years (34%) followed by the age group 41- 50 years (30), 51 – 60 years (30%) and ≤ 40 years (6%). The mean age ± SD: 56.02 ± 10.63 and the age range from 35 year to 80 year.
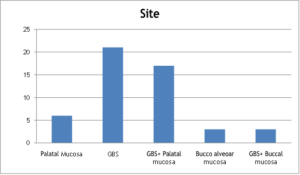
Figure 02: Distribution of the patients according to site (n=50)
The distribution of the patients according to site. Among 50 patients, maximum (42%) of the lesions located in the gingiva buccal sulcus (GBS) followed by GBS + palatal mucosa (34%) and palatal mucosa (12%). Bucco alveolar mucosa and GBS + buccal mucosa affect with the same frequency (6%).
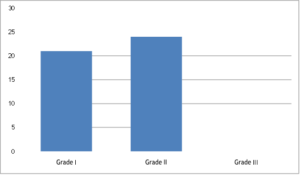
Figure 03: Histologic types of primary lesions (Conventional grading) (n=50)
Grade II lesions are the most prevalent in the study patiens (48%). 42% and 10% of the lesions are the Grade I and Grade III respectively in the conventional grading system.
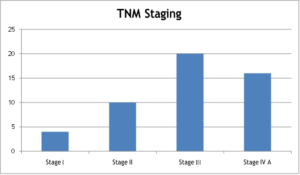
Figure 04: Distribution of the patients according to TNM staging (n=50).
Most of the cases are in Stage III (40%) followed by Stage IV A (32%), Stage II (20%) and Stage I (8%) according to TNM Staging system.
Table 02: Association between clinical staging and pathological staging of lymph node(n=50)
| Clinical staging of lymph
Node |
Pathological staging of lymph node | Total | ||||
| N0 | N1 | N2A | N2B | N2C | ||
| N0 | 12 (80%) | 3 (20%) | 0 | 0 | 0 | 15 (10%) |
| N1 | 17 (68%) | 5 (20%) | 0 | 3 (12%) | 0 | 25 (100%) |
| N2A | 1
(33.33%) |
1 (33.33%) | 0 | 1 (33.33%) | 0 | 3 (100%) |
| N2B | 0 | 1 (20%) | 2 (40%) | 2 (40%) | 0 | 5 (100%) |
| N2C | 2 (100%) | 0 | 0 | 0 | 0 | 2 (100%) |
| Total | 32 (64%) | 10 (20%) | 2 (4%) | 6 (12%) | 0 | 50 (100%) |
The cross tabulation between clinical staging of lymph nodes and pathological staging of lymph nodes. Clinically suspected N0 case was confirmed by histological examination where 20% become N1..Among 25 clinically suspected N1 cases are confirmed hy histological examination where 68% become N0, 20% N1 and 12% N2B.
Table 03: Relationship between Ultrasonographic finding and histological finding of lymph node (n=50)
| Ultrasonographic
finding of lymph node |
Histological finding of lymph node | Total | |
| Positive | Negative | ||
| Positive | 13 (68.42%) | 6 (31.58%) | 19 (100%) |
| Negative | 4 (12.90%) | 27 (87.10%) | 31 (100%) |
| Total | 17 (34%) | 33 (66%) | 50 (100%) |
Table 03 shows cross relationship between ultrasonographic finding of lymph node and histological finding of lymph node. Ultrasonographically positive lymph nodes were confirmed by histological examination where 68.42% become positive and 31.58% become negative. Ultrasonographically negative lymph nodes were confirmed by histological examination where 12.90% become positive and 87.10% become negative.
Table 04: Relationship between Ultrasonographic finding and histological finding of lymph node (n=50)
| Ultrasonographic
finding of lymph node |
Histological finding of lymph node | Total | |
| Positive | Negative | ||
| Positive | 13 (68.42%) | 6 (31.58%) | 19 (100%) |
| Negative | 4 (12.90%) | 27 (87.10%) | 31 (100%) |
| Total | 17 (34%) | 33 (66%) | 50 (100%) |
Table 04 shows cross relationship between ultrasonographic finding of lymph node and histological finding of lymph node. Ultrasonographically positive lymph nodes were confirmed by histological examination where 68.42% become positive and 31.58% become negative. Ultrasonographically negative lymph nodes were confirmed by histological examination where 12.90% become positive and 87.10% become negative. The sensitivity, specificity, positive predictive value, negative predictive value & Accuracy of Ultrasonographic technique for determining metastatic cervical lymph node were 76.47%, 81.82%, 68.42%, 87.10% and 80% respectively.
Table 05: Relationship between primary site of OSCC of maxilla & histopathological cervical level of LN metastasis.
| Level of LN | Primary Site | ||||
| Submandibular LN | Palatal Mucosa (-) | GBS 07 (14%) | GBS+
Palatal Mucosa 06 (12%) |
Buccal+ Alveolor+ GBS
02 (4%) |
Buccal+ GBS
01 (2%) |
| Jugulodigastric LN | Palatal
Mucosa (-) |
02 (4%) |
(-) |
(-) |
(-) |
Total 36% LN metastasis according to histopathological report. Among them, 14% in lelvel Ib from GBS, 4% in IIa from GBS, 12% in Ib from GBS & palatal mucosa, 4% in Ib buccal, alveolor mucosa & GBS, 2% in Ib from buccal & GBS.
- DISCUSSION
The presence of metastatic cervical lymph nodes is very important with regard to patient prognosis and treatment planning. The cervical lymph nodes should be suggested as metastatic in patients with primary carcinoma of the head and neck and treated accordingly. However, this does not mean that every palpable lymph node is metastatic; it may be a reactive lymph node. On the other hand, there may be positive lymph nodes pathologically, even though there is no palpable lymph node. The presence of cervical lymph node metastasis in oral squamous cell carcinoma often also changes the extent of surgical treatment or radiotherapy and chemotherapy [4].The LN drainage of the maxillary alveolus, GBS and hand palate is generally predictable & flows via two routes: via the submandibular nodal group (Ib) & then to the sup. jugular chain (Ila) or via the retro- pharyngeal plexus (Vlla) and again on to the sup. jugular chain [15]. In the study [10], total metastatic rate was 34% in 100 cases; whereas in our study, it is 36% in 50 cases. Our study is dissimilar with this study, in another study, [21] showed 37.9% LN metastasis in OSCC arising from the upper oral cavity among 66 patients. Our study is much of a muchness with this study. In the study [32] positive LNS were mostly detected at levels I-III and it is almost same in our study which is shown in table above. There was no significant difference in metastatic rate between primary sites of maxillary gingiva and anterior part of hard palate [11]. Tumour involving the gingivo-buccal sulcus presented a significantly higher risk of metastasis in the study [29]. In our study, it is about 34%. cervical LN metastasis in OSCC of maxilla where GBS involvement is about 14%. In our study, second common site of LN metastasis in maxillary SCC is GBS with anterior part of hard palate. A study showed skip metastasis was seen in 4.31% cases jugulodigastric nodes from maxillary SCC whereas our study, we’ve found 4% jugulodigastrie LN metastasis from GBS of maxilla. It is well known that palpation is an inaccurate technique to stage cancer in the neck [16]. The drawback of palpation method for evaluating neck lymph node is that it is a subjective method and is totally operator and experience dependent. It can be competitive with other investigation modalities if the skill can be improved by repeated examinations of neck. Examination of cervical nodes should be done systemically. Knowledge of grouping and location of cervical lymph nodes is necessary. For Sub maxillary and Sub mental nodes: Roll the fingers against inner surface of Mandible with patient’s head gently tilted towards one side. Deep cervical lymph nodes should be palpated, one side at a time [24]. Gently bend the patient’s head forward and roll your fingers over the deeper muscles along the carotid arteries. For palpation of preauricular nodes, roll your finger in front of the ear, against the maxilla. In the study [15], sensitivity, specificity, positive predictive value, negative predictive value & accuracy of palpation method for determining metastatic cervical lymph node were 64%, 85%, 78%, 74% and 75%. In a study sensitivity, specificity, positive predictive value, negative predictive value & accuracy of palpation method for determining metastatic cervical lymph node were 75.6%, 60%, 88.6%, 37.5% and 72.5% [31]. Our study result is comparable to the study result [24], the comparison proves that the sensitivity value and the negative predicitive value was almost same with the study result respectively, though there were some dissimilarity exists in other values. In my study palpation method showed high sensitivity (83.33%) and negative predictive value (80%) which has limited clinical value as probably many metastatic lymph nodes were palpable. The sensitivity would have been lower if the study was limited to No neck population [33]. Sonographic criteria, such as nodal size and configuration ofthe lesion, and Doppler Sonographic criteria have been studied extensively for their value to differentiate between benign and malignant lymphatic disease in the neck. The minimal axial diameter appears to be the most accurate size criterion, compared to the maximal axial diameter and the longitudinal diameter. Regarding the aspect of lymph nodes on sonograms, the echogenic hilus appears to be a reliable parameter. The configuration (shape) of the node might be important, but some authors doubt its value. Following the above criteria the patients were evaluated with a high- resolution sonography machine with use of color and power Doppler. After clinical and Sonographic evaluation the subjects were treated by neck dissection and evaluated by histopathological examinations [34].
- CONCLUSIONS
Lymphatic metastasis effects on prognosis, decision making for treatment plan. The presence of cervical lymph node metastasis in oral squamous cell carcinoma often also changes the extent of surgical treatment or radiotherapy and chemotherapy. Performing neck dissection in N0 neck of maxillary carcinoma prevents recurrence rate. This study revealed that maximum SCC patients (48%) were moderately differentiated and most of the cases were in Stage III (40%) according to TNM staging. Ultrasonographically positive lymph nodes were confirmed by histological examination where 68.42% become positive and 31.58% become negative. Ultrasonographically negative lymph nodes were confirmed by histological examination where 12.90% become positive and 87.10% become negative. USG is operator and skill dependent so it was an important drawback of this technique. Lymphatic metastasis is common in neck region for oral SCC of maxillary GBS, alveolar and anterior two-third of hard palate. Early diagnosis with proper evaluation of oral SCC is necessary for good prognosis of the disease. Neck dissection is must as prophylactic management in case of maxillary SCC. High resolution Doppler sonography might be an adjunct tool in diagnosing metastatic nodes in oral SCC patients. USG is not only the non-invasive tool but also need to do MRI for neck evaluation. More studies are needed to analyze in detail the distribution delays among patients. Routine examination of the oral cavity by dental practitioners and other health care providers helps in the early detection of premalignant and malignant oral disease. General practitioners including dentists can play a significant role in disseminating information regarding oral cancer. The government and non-government organization (NGO) should take necessary steps to increase the awareness among the people of Bangladesh by arranging various programs.
REFERENCES
- Aldosimani, M., Verdonschot, R.G., Iwamoto, Y., Nakazawa, M., Mallya, S.M., Kakimoto, N., Toyosawa, S., Kreiborg, S. and Murakami, S.. Prognostic factors for lymph node metastasis from upper gingival carcinomas. Oral radiology, 2022, 38(3), pp.389-396.
- Argiris A, Karamouzis MV, Raben D, Ferris RL. Head andneck cancer. Lancet 371(9625):1695–1709.
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics,2008.CA. CA: Cancer J Clin, 2008, 58(2):71-96
- ICMR, National Cancer Registry of Indian Council for Medical Research,annual report 1984, 1987. New Delhi ICMR. Jackson SR, Stell PM. Second radical neck dissection.ClinOtolaryngol 1991; 16:52-58.
- Steinkamp HJ, et al. Reactive enlargement of cervical lymph nodes and cervical lymph node metastasis: sonography and computed tomography. AktuelleRadiol 1992;2:188-95.
- Sparano A, Weinstein G, Chalian A, Yodul M, Weber R. Multivariate predictors of occult neck metastasis in early oral tongue cancer. Otolaryngology—Head and Neck Surgery. 2004 Oct;131(4):472-6.
- Lambert R, Sauvaget C, de Camargo Cancela M, Sankaranarayanan R. Epidemiology of cancer from the oral cavity and orophar-ynx. Eur J GastroenterolHepatol , 2011, 23(8):633–641
- Anisha Shrestha, Archana Pandey Bista, Kalpana Paudel & Madhusudan Subedi (2024). Experiences of Nurses Regarding Caring Behavior in Intensive Care Units. Dinkum Journal of Medical Innovations, 3(07):483-492.
- Capote A, Escorial V,Munoz-Guerra MF, Rodriguez-Campo FJ,Gamallo C, Naval L. Elective neck dissection in early-stageoral squamous cell carcinoma— does it influence recurrence and survival?HeadNeck, 2007, 29(1):3–11
- Hiratsuka H, Miyakawa A, Nakamori K, Kido Y, Sunakawa H, Kohama GI. Multivariate analysis of occult lymph node metastasis as a prognostic indicator for patients with squamous cell carcinoma of the oral cavity. Cancer: Interdisciplinary International Journal of the American Cancer Society. 1997 Aug 1;80(3):351-6.
- Yang, H., Son, N.H., Lee, S.H., Kim, D., Kim, H.J., Cha, I.H. and Nam, W., Predictive modelling of level IIb lymph node metastasis in oral squamous cell carcinoma. Scientific Reports, 2021. 11(1), pp.1-
- Jami Parvin Nitu, Kamrun Nahar, G. R. M. Shafy Parvez, Sumaiya Sabrin, Mahbub Ur Rahim & ANM Shamsul Islam (2024). Experiences of Dental Surgeon in Providing Dental Health Care during Covid-19 Pandemic. Dinkum Journal of Medical Innovations, 3(06):434-441.
- Woolgar JA. The topography of cervical lymph node metasta-ses revisited: the histological findings in 526 sides of neck dissection from 439 previously untreated patients. Int J Oral Max Surg , 2007, 36(3):219-225
- Mishra P, Sharma AK. A 3-year study of supraomohyoid neck dissection and modified radical neck dissection type I in oral cancer:with special reference to involvement of level IV node metastasis.Eur Arch Otorhinolaryngol, 2010, 267(6):933– 938
- Yuen AP, Ho CM, Chow TL, Tang LC, Cheung WY, Ng RW, Wei WI, Kong CK, Book KS, Yuen WC, Lam AK, Yuen NW, Trendell-Smith NJ, Chan YW, Wong BY, Li GK, Ho AC, Ho WK, Wong SY, Yao TJ Prospective randomized study of selective neck dissection versus observation for N0 neck of early tongue carcinoma.HeadNeck , 2009, 31 (6):765-772.
- Qu, Y., Liu, Y., Su, M., Yang, Y., Han, Z. and Qin, L., The strategy on managing cervical lymph nodes of patients with maxillary gingival squamous cell carcinoma. Journal of Cranio-Maxillofacial Surgery, 2019, 47(2), pp.300-304.
- Chiu RJ, Myers EN, Johnson JT. Efficacy of routine bilateral neck dissection in the management of supraglottic cancer. Otolaryngol Head Neck Surg, 2004, 131(4):485– 488
- Haddadin KJ, Soutar DS, Oliver RJ, Webster MH, Robertson AG,MacDonald DG. Improved survival for patients with clinically T1/T2, N0 tongue tumors undergoing a prophylactic neck dissection.Head Neck, 1999, 21(6):517–525
- Binahmed A, Nason RW, Hussain A, Abdoh AA, Sandor GK. Treatment outcomes in squamous cell carcinoma of the maxillary alveolus and palate:a population-based study. Oral Surg Med Oral Pathol Oral RadiolEndod, 2008 105(6):750-75
- Hanna E, Suen J. Management of cervical metastases in head and neck cancer. AdvOtolaryngol Head Neck Surg 1999; 13:287-320.
- Roshan Gyawali, S. Rajarajan, Yuvraj Regmi & Sachin Aryal (2024). Preparation of Co-Amorphous System Formulation of Poorly Aqueous Soluble API’s for Suitable Acidic & Basic Drug for Oral Drug Delivery. Dinkum Journal of Medical Innovations, 3(06):442-459.
- Pathak KA, Mathur N, Talole S, Deshpande MS, Chaturvedi P, PaiPS,et al. Squamous cell carcinoma of the superior gingival-buccal complex. Oral Oncol2007;43:774-9.
- Kruse AL, Gratz KW. Cervical metastases of squamous cell carcinoma of the maxilla: a retrospective study of 9 years. Head Neck Oncol, 2009 1:28
- SimentalJr AA, Johnson JT, Myers EN. Cervical metastasis from squamous cell carcinoma of the maxillary alveolus and hard palate. The Laryngoscope. 2006 Sep;116(9):1682-4.
- Beasley NJ. Prevo R, Banerji S et al.Intra-tumorallymphangiogenesis and lymphnode metastasis in head and neck cancer.Cancer research 2002;62:1315- 20.
- John C Watkinson, Ralph W golber. Stell and Maran’s Textbook of Head and Neck Surgery and Oncology (2012). 5th edition; p.662.
- Haberal I, Çelik H, Göçmen H, Akmansu H, Yörük M, Özeri C. Which is important in the evaluation of metastatic lymph nodes in head and neck cancer: palpation, ultrasonography, or computed tomography?. Otolaryngology—Head and Neck Surgery. 2004 Feb;130(2):197-201.
- Mamelle G, Pampurik J, Luboinski B, et al. Lymph node prognostic factors in head and neck squamous cell carcinomas. Am J Surg.1994;168(5):494–498
- Mantravadi RV, Skolnik EM, Haas RE, et al. Patterns of cancer recurrence in the postoperatively irradiated neck. Arch Otolaryngol. 1983;109(11):753–756
- Leemans CR, Tiwari R, Nauta JJ, et al. Regional lymph node involvement and its significance in the development of distant metastases in head and neck carcinoma. Cancer. 1993;71(2):452–456
- Naito K. Analysis of cervical metastatic lymphadenopathy by ultrasonography. Nihon IgakuHoshasenGakkaizasshi. Nippon ActaRadiologica. 1990 Aug 1;50(8):918-27.
- Lefebvre JL, Castelain B, De la Torre JC, et al. Lymph node invasion in hypopharynx and lateral epilarynx carcinoma: a prognostic factor. Head Neck Surg. 1987;10(1):14–18
- Soo KC, Spiro RH, King W. Squamous carcinoma of the gums. Am J Surg 1988;156:281–285.
- Johnson NW. Orofacial neoplasms: global epidemiology, risk factors and recommendations for research. International dental journal. 1991 Dec 1;41(6):365-75.
Publication History
Submitted: August 19, 2024
Accepted: August 28, 2024
Published: August 31, 2024
Identification
D-0308
DOI
https://doi.org/10.71017/djmi.3.8.d-0308
Citation
Nujhat Minhaj, Mohasin Mia & Rukhshana Afroz Afrin (2024). Level and Pattern of Cervical Lymph Node Metastasis from Gingivo Buccal Sulcus & Palatal Mucosa of Maxilla in Oral Squamous Cell Carcinoma. Dinkum Journal of Medical Innovations, 3(08):570-580.
Copyright
© 2024 The Author(s).