

")
Publication History
Submitted: August 19, 2024
Accepted: August 28, 2024
Published: August 31, 2024
Identification
D-0312
DOI
https://doi.org/10.71017/djmi.3.8.d-0312
Citation
Muneshwor Sah, Ram Bahadur K.C, Prasanna Bahadur Amatya & Arati Kattel (2024). Association between Abo-Rh Blood Groups and Type-2 Diabetes Mellitus: Comparative Cross Sectional Study. Dinkum Journal of Medical Innovations, 3(08):619-629.
Copyright
© 2024 The Author(s).
619-629
Association between Abo-Rh Blood Groups and Type-2 Diabetes Mellitus: Comparative Cross Sectional StudyOriginal Article
Muneshwor Sah 1*, Ram Bahadur K.C 2, Prasanna Bahadur Amatya 3, Arati Kattel 4
- National Academy of Medical Sciences, Bir Hospital, Kathmandu, Nepal.
- National Academy of Medical Sciences, Bir Hospital, Kathmandu, Nepal.
- National Academy of Medical Sciences, Bir Hospital, Kathmandu, Nepal.
- Lumbini Eye institute Siddharthanagar, Rupandehi, Nepal.
* Correspondence: muneshwor.sah72@gmail.com
Abstract: Diabetes mellitus is a disease of abnormal carbohydrate metabolism that are characterized by hyperglycemia which is associated with a relative or absolute impairment in insulin secretion, along with varying degrees of peripheral resistance to the action of insulin. Type-2 diabetes mellitus (T2DM), which is responsible for significant morbidity and mortality is a disease of continued scientific research. This study evaluated any association between ABO-RH blood groups among T2DM and healthy individuals. A hospital-based comparative cross-sectional study was conducted for one year in Department of Endocrinology, Department of Internal medicine and surgical ward of Bir Hospital, National Academy of Medical Sciences, Kathmandu, Nepal. The study included total N=384 participants above 20 years of age were selected, out of which 192 were normal healthy controls (non-diabetics) and 192 participants were T2DM irrespective of glucose control, treatment and gender. Blood samples were collected from the Patients after consent had been obtained and then ABO blood groups of all subjects were determined and recorded by Slide Agglutination method at Hematology laboratory and Blood bank. Data were analyzed by chi square test and the results showed that there was no significant association among the various ABO blood groups. The data revealed that blood group B was significantly more common among diabetic patients n=76 (39.58%) and non-diabetic n=63 (32.81%) healthy populations whereas blood group AB was significantly less common among both populations i.e. n=48 (12.50%) in an order of B > A > O > AB. The frequency of Rh-positive and Rh-negative blood were 95.31% and 4.69% respectively. There was a significant difference between healthy subjects and diabetic patients in blood group B and Rh-positive groups. Highest mean HbA1C seen in blood group A among male (9.32) and female (7.75) along with more complications seen in blood group B but no statistical significance achieved. Subjects with blood group “B” are at high risk while individuals with blood group “AB” are at low risk of evolving type 2 diabetes. It is suggested that subjects with blood group “B” should be closely monitored by physicians as these subjects have an increased risk of type 2 diabetes. Large studies are needed to confirm these results.
Keywords: Blood groups ABO-RH, Diabetes mellitus, Association
- INTRODUCTION
The term “diabetes” (Greek; siphon) was first coined by Araetus of Cappodocia (81-133 A.D.) and the word “mellitus” (Latin; honey sweet) was added by Surgeon-General Thomas Willis of Britain in 1675 after rediscovering the sweetness of urine. History of this disease however goes back to more than 1500 B.C. where Egyptians described it as “too great emptying of urine”[1,2]. Diabetes mellitus refers to a group of common metabolic disorders that share the phenotype of hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Several distinct types of DM are caused by a complex interaction of genetics and environmental factors [3]. The classic symptoms of untreated diabetes are weight loss, polyuria, polydipsia and polyphagia [4]. Increasing incidence with DM worldwide, it is likely to continue to be a leading cause of morbidity and mortality in the future. Immune mediated diabetes or juvenile onset diabetes, which results 5-10% of those with diabetes, occur as a result of autoimmunity against the insulin-producing beta cells, resulting in complete or near-total insulin deficiency [5]. The diagnosis of T1DM is done by finding the evidence of autoimmunity (the presence of anti-islets cell antibodies (ICA)-antiglutamic acid decarboxylase (GAD), anti-islet-associated protein 2 (IA2) antibodies in the blood. Thus, genetic markers are present from birth, immune markers are detectable after the onset of the autoimmune process, whereas metabolic markers can be identified with sensitive tests once enough beta cell damage has been occurred, but before the onset of symptomatic hyperglycemia [6]. However various risk factors have been proposed but none of them have been validated with precision. These factors include enterovirus infections, diet, obesity, vitamin D deficiency, immunization and low birth weight. The clinical features are only apparent when 90% or more of the beta cells are lost [7]. Compared to type 2 diabetes mellitus, where both decreased insulin release (not due to an autoimmune etiology) and insulin resistance play a significant role, type 1A diabetes has a very distinct pathophysiology. Although inflammation (e.g., interleukin-1 mediated) may have a role in islet beta cell death in both types of diabetes, genome-wide association studies show that type 1 and type 2 diabetes’ genetic loci do not overlap [8]. HLA-DQalpha, HLA-DQbeta, HLA-DR, preproinsulin, the PTPN22 gene, CTLA-4, interferon-induced helicase, IL2 receptor (CD25), a lectin-like gene (KIAA0035), ERBB3e, and an undefined gene at 12q are among the genes whose polymorphisms are known to affect the risk of type 1A diabetes [9,10]. The relationships were validated by a meta-analysis of information from genome-wide association studies, which also discovered four additional risk loci (BACH2, PRKCQ, CTSH, and C1QTNF6) linked to an elevated risk of type 1 diabetes [11].Islet cell autoantibodies (ICAs) were initially found in the blood of autoimmune polyendocrine insufficiency patients; they have now been found in 85% of people with newly diagnosed type 1 diabetes and in pre-diabetic participants. Autoantibodies can be found using radioassays because they react with particular islet autoantigens [12,13]. In a study of 892 children with diabetes and 2291 healthy children in Europe, certain pregnancy-related and perinatal variables were linked to a slight increase in the risk of type 1 diabetes. Preeclampsia, infant respiratory illness, maternal age >25 years, and jaundice, particularly those caused by ABO blood group incompatibility; protective factors were low birth weight and short birth length. One cohort analysis discovered a weak but substantial direct link between type 1 diabetes risk and birth weight [14,15]. Type 2 DM is a heterogeneous group of disorders characterized by variable degrees of insulin resistance, impaired insulin secretion, and increased hepatic glucose production. Hyperglycemia, insulin resistance, and a relative impairment in insulin production are the hallmarks of type 2 diabetes mellitus. Although type 2 diabetes is a heterogeneous disease with patients suffering varied levels of impaired insulin production and insulin action, the diagnostic criteria for the disease rely exclusively on measures of raised glycemia without clear understanding of the underlying pathophysiology (insulin resistance)[16]. The burden of type 2 diabetes mellitus (T2DM) is increasing worldwide and raising concern in which pathophysiologic mechanisms for the association between ABO-RH blood group with T2DM and its associated factors are still not well understood [17]. Increasing trend result fast epidemic in some countries of the world leading to number of people affected leading to double in the next decade which is due to increase in ageing factor especially in poorly developed countries[18]. Among all the major types of diabetes, T2DM is far more common which cover more than 90% of all cases than either type 1 diabetes mellitus (T1DM) or gestational diabetes [19]. Type 2 DM is caused mainly due to lifestyle factors (physical inactivity, sedentary lifestyle, cigarette smoking and generous consumption of alcohol ) and genetic. Over the past ten years, there has been an alarming increase in the prevalence of type 2 diabetes, which is largely attributed to the obesity and sedentary lifestyle trends [20]. Type 2 diabetes has a complex etiology [21], typically, patients have both insulin resistance in variable degrees and faulty insulin production (beta cell dysfunction), neither of which are frequently assessed in the clinical setting. Both factors have a role in type 2 diabetes, with increased insulin action demand caused by insulin resistance predominantly “environmental” variables associated with overeating, sedentary behavior, and the accompanying overweight and obesity are the primary causes with aging and genetics playing a less significant role and inadequate insulin secretion [22,23]. Thus, GDM provides a distinctive opportunity to study the early pathogenesis of diabetes and also to develop interventions regarding prevention the disease. Study of blood groups, mainly ABO and Rh systems has been given high priority because of its medical importance [25]. Many researchers have made attempts to determine the significance of particular ABO phenotypes for susceptibility to disease. However, along with their expression on RBCs, ABO antigens are also highly expressed on the surface on a variety of human cells and tissues, including the epithelium, sensory neurons, platelets, and the vascular endothelium [26]. ABO antigens are also expressed on vascular endothelium and through unclear mechanisms, associated with levels of the procoagulant proteins factor VIII (FVIII) and von Willebrand factor (VWF) and markers of endothelial function such as p-selectin and soluble intracellular adhesion molecule [27] and is the most studied group in the human population out of more than 100 blood group systems involving over 500 antigens [28]. Diabetes is a complex, chronic illness requiring continuous medical care with multi factorial risk reduction strategies beyond glycemic control, seen both in the developed and the developing countries but the rate of increase is significantly higher in developing world. According to World Health Organization (WHO), 422 million people have diabetes mellitus (DM) worldwide and the number is increasing from an estimated 30 million cases in 1985 to 382 million in 2013. If such trend continues, more than half a billion population of the world will be diabetic by 2035[29].
- MATERIALS & METHODS
Hospital based comparative cross sectional prospective observational study design Bir Hospital, NAMS, Kathmandu, Nepal. The hospital is one of the largest tertiary centre of Nepal and has Data from FY 2074/75 showed out of 11600 inpatients, 344(2.90%) were type 2 diabetic mellitus.In FY2075/76 showed out of 12605 inpatients, 305(2.41%) were type 2 diabetic mellitus. In FY 2076/77 showed out of 10562 inpatients, 297(2.81%) were type 2 diabetic mellitus. Patients with type-2 DM patients admitted under Department of Endocrinology, Department of Internal medicine and Department of General Surgery of Bir hospital, NAMS, Kathmandu, Nepal. Study period is one year, sample size calculated using for comparison between two groups:
Here, n= 2 (Zβ + Zα)2 * (1-P)/(P1-P2)2
where,
n= total sample size
P1 =Proportion of the B blood group among healthy controls i.e. 18.9%
P2 = Proportions of the B blood group among T2DM patients i.e. 33%56
Zβ= power at 80% i.e. 0.842 (from Z table)
Zα = level of significance at 95% i.e. 1.96 (from Z table)
P1-P2= difference in proportion of events in two groups
P = pooled prevalence = P1-P2/2
Total sample size calculated 306 (153 participants in each group), after adjusting 10% non repsone rate, finale sample size N=384 (192 participants in each groups). A total of 384 subjects taken in this study with 192 making up the test group (diabetics) and 192 (non-diabetics) as control. All patients with T2DM visiting OPD and admitted in endocrinology Internal medicine and surgical ward in Bir Hospital under the inclusion criteria and not falling under the exclusion criteria taken. ABO-Rh blood grouping done by Slide agglutination test (In labs, around 2 to 3 ml of blood was drawn from the peripheral veins and collected in EDTA vial. ABO slide agglutination test was carried out to determine blood groups of patients using anti A, B and D vials (IgG + IgM). Slide agglutination test is used for ABO RH typing.Fasting blood sugar and prandial sugar is checked by ERBA Manheim XL SysPack -Trinder method By ERBA Manheim XL SysPack – particle enhanced immunoturbidimetric test .HbA1C determined directly without measurement of total hemoglobin. Following the ethical clearance from the Institutional Review Board (IRB) of the NAMS, patient explained about the purpose of the study and methods to be used. Informed written consent taken, every precaution taken to maintain the privacy of the patient as possible. Data collected using structured Porforma containing the demographic details of the study population meeting the inclusion criteria. The investigation (blood grouping and Rh typing) required for my study which were already sent by respective consultant filled in predesigned proforma sheet. The first blood group antigen system, recognized in 1900, was ABO, The major blood groups of this system are A, B, AB, and O. O type RBCs lack A or B antigens. The genes that determine the A and B phenotypes are found on chromosome 9p and are expressed in a Mendelian codominant manner. The Rh antigens are found on a 30- to 32-kDa RBC membrane protein that has no defined function. The presence of the D antigen confers Rh “positivity,” while persons who lack the D antigen are Rh negative. The D antigen is a potent alloantigen. About 15% of individuals lack this antigen, data collected for T2DM as well as controls checked for completeness, cleaned, arranged, and categorized manually. Data entered in and analyzed using statistical software IBM-SPSS (Statistical Package for Social Sciences) version 24.0. Descriptive analysis performed for each variable. Frequency and percentage computed for categorical variable. In Bivariate analysis, chi square test employed to identify the one-to-one relationship between predictors and outcome variables. Independent sample t-test used for continuous variables. To adjusting confounding variables, binary logistic regression used to identify the relationship between predictors and outcome variables. The P-value ≤ 0.05 considered as statistically significant.
- RESULTS & DISCUSSIONS
Table 01 showed distribution of ABO blood group in T2DM and healthy population by gender. Out of total 384 participants equal in each group i.e. 192 T2DM and 192 healthy population, highest participant were male (n=98) with blood group B (n=42, 42.86%) involving T2DM in order of B > O > A >AB whereas highest participants were female (n=158) in healthy population with similar blood group B (n=50, 31.65%) in order of B > A > O > AB. There was no significant association among blood groups in both genders i.e. male (p-value 0.897) and female (p-value 0.577).
Table 01: Distribution of ABO blood group inT2 diabetics and healthy individual by gender
| BLOOD GROUPS | Male | p-value | Female | p-value | ||
| Healthy individual
(n=34) |
Diabetic individual
(n=98) |
Healthy individual
(n=158) |
Diabetic individual(n=94) | |||
| A | 9 (26.47) | 20 (20.41) | 0.897 | 46 (29.11) | 26 (27.66) | 0.577 |
| B | 13 (38.24) | 42 (42.86) | 50 (31.65) | 34 (36.17) | ||
| AB | 4 (11.76) | 11 (11.22) | 24 (15.19) | 9 (9.57) | ||
| O | 8 (23.53) | 25 (25.51) | 38 (24.05) | 25 (26.60) | ||
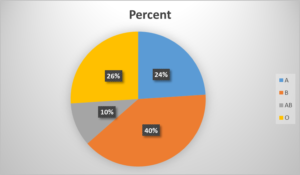
Figure 01: Distribution of ABO blood groups among T2DM patients
Figure 01 showed distribution of ABO blood groups among T2DM patients where blood group B comprised maximum percentage 40% followed by blood group O (26%), blood group A (24%) and least as blood group AB (10%) respectively. Table 02 showed distribution of ABO blood groups among T2DM and healthy population. In diabetic population (n=192), blood group B (n=76, 39.58%) were the highest in number followed by blood group O (n=50, 26.04%), blood group A (n=46, 23.96%) and blood group AB (N=20, 10.42%) respectively where as in healthy population, blood group B is highest (n=63,32.81%) similar as T2DM followed by blood group A (n=55, 28.65%), blood group O (n=46, 23.96%) and blood group AB (28, 14.58%) respectively. However, there was no significant association among the various ABO blood groups as shown in table below.
Table 02: Distribution of ABO blood groups among T2DM and healthy individuals
| Blood group | Total
(N=384) |
Healthy individual
(n=192) |
Diabetic individual
(n=192) |
Chi square test | P-value1 |
| N (%) | n (%) | n (%) | |||
| A
B AB O |
101 (26.30)
139 (36.20) 48 (12.50) 96 (25.00) |
55 (28.65)
63 (32.81) 28 (14.58) 46 (23.96) |
46 (23.96)
76 (39.58) 20 (10.42) 50 (26.04) |
3.51 | 0.318 |
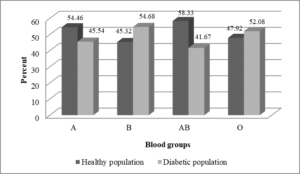
Figure 02: Distribution of ABO blood groups among T2DM and healthy individual
Figure 02 showed distribution of ABO blood groups among T2DM and healthy population in bar diagram
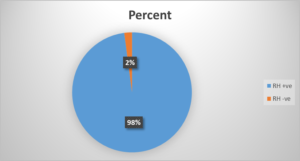
Figure 03: Distribution of RH blood groups among T2DM patients
Figure 03 showed distribution of rhesus blood groups among T2DM patients where the maximum percentage 98% among RH +ve group of patients.
Table 03: Distribution of RH blood groups among T2DM and healthy individual
| Blood group | Total | Healthy individual | Diabetic individual | Chi square test | P-value |
| N (%) | n (%) | n (%) | |||
| RH +ve
RH –ve |
366 (95.31)
18 (4.69) |
178 (92.71)
14 (7.29) |
188 (97.92)
4 (2.08) |
5.82 | 0.016* |
Table 03 showed distribution of rhesus blood groups among T2DM and healthy population. Maximum number of T2DM patients were RH+ (n=188, 97.92%) followed by RH- (n=4, 2.08%) where as maximum number of healthy populations were also RH+ (n=178, 92.71%) followed by RH- (n=14, 7.29%) respectively with significant association (P value < 0.05) between RH+ and RH- blood group.
Table 04: Relationship of ABO blood group and HbA1c level.
| Blood groups | HbA1c | |
| Male
Mean (SD) |
Female
Mean (SD) |
|
| A | 9.32 (2.03) | 7.75 (2.18) |
| B | 8.38 (1.39) | 8.50 (1.73) |
| AB | 7.73 (0.81) | 7.94 (1.90) |
| O | 7.98 (1.10) | 8.13 (1.54) |
Table 04 showed relationship of ABO blood group and HbA1c level. Blood group A has highest mean value (9.32 ) in male participants followed by blood group B, O and AB where as blood group B has highest mean value (8.50 ) in female participants followed by blood group O, AB and A respectively.
Table 05: Distribution of ABO blood groups by HbA1c among T2DM
| Blood groups | Mean | Standard deviation |
| A
B AB O |
8.43
8.43 7.83 8.06 |
2.24
1.54 1.37 1.33 |
Table 05 showed distribution of ABO blood group by HbA1c among T2DM patients and data showed blood group A and B have got similar mean value with 8.43 followed by blood group O and AB.
Table 06: Distribution of ABO blood group in diabetic population by complications
| BLOOD GROUPS | Complications | Chi square test | p-value1 | |
| Yes (%) | No (%) | |||
| A | 12 (25.53) | 34 (23.45) | 0.748 | 0.862 |
| B | 20 (42.55) | 56 (38.62) | ||
| AB | 5 (10.64) | 15 (10.34) | ||
| O | 10 (21.28) | 40 (27.59) | ||
Table 06 showed distribution of ABO blood group in T2DM participants on the basis of complication in T2DM. Greater percentage of complication was seen in patient with blood group B (n=20, 42.55%) followed by blood group A (n=12, 25.53%), O (n=10, 21.28%) and AB (n=5, 10.64%) with no significant association seen between blood group with or without complications.
Table 07: Distribution of ABO blood group in diabetic population by drugs
| BLOOD GROUPS | Drugs | Chi square test | p-value | |
| OHA
n (%) |
Insulin
n (%) |
|||
| A | 38 (24.05) | 8 (23.53) | 0.927 | 0.819 |
| B | 64 (40.51) | 12 (35.29) | ||
| AB | 15 (9.49) | 5 (14.71) | ||
| O | 41 (25.95) | 9 (26.47) | ||
Table 07 showed distribution of ABO blood groups in T2DM patient on the basis of drug used. Most patient of blood group B are on oral hypoglyceamic agents (n=64, 40.51%) and very few patients are on insulin therapy (n=12, 35.29%) followed by blood group O, A and AB which is similar to insulin therapy as well with no significant association between drugs and diabetes mellitus seen.
- DISCUSSION
DM is a chronic, metabolic endocrinal disorder which is responsible for significant morbidity and mortality [30]. In the past, large number of studies about association between chronic and metabolic diseases with ABO and RH blood groups had been carried out. DM (especially T2DM) is affected by many environmental factors but it has also a hereditary character [31]. Whether DM have also association with ABO and RH blood groups have been a subject of interest for long time. ABO phenotype has been linked to a number of diseases’ susceptibilities. For instance, it is discovered that gastric cancer is higher typical for blood group A, whereas duodenal and gastric ulcers or Schizophrenia is more prevalent among people with blood type O [32]. This study was conducted in Bir hospital, NAMS, Kathmandu, Nepal in which total of 384 subjects was enrolled with 192 making up the test group (diabetics) and 192 (non-diabetics) as control. All patients with T2DM visiting OPD and admitted in endocrinology Internal medicine and surgical ward under the inclusion criteria and not falling under the exclusion criteria were taken in a study period of 12 months. The blood groups of all patient were documented. This study was a comparative cross sectional study about the association between ABO and RH blood groups with type-2 diabetes mellitus. This study demonstrated that the frequency of blood group B (n=76, 39.58%) was significantly higher among type 2 diabetes mellitus patients with even similar blood group B (n=63, 32.81%) among healthy populations followed by blood group O, A and AB. Study done in TUTH, the oldest health institution of Nepal, reported that blood group O to be the most common blood group [33]. Despite the commonest blood group, it was not the most common blood group in the diabetic population in this study. It also found a negative association between blood groups A and O, and concluded that that those blood groups had lesser chance of DM [34,35]. Similar study conducted from Pakistan did a descriptive cross-sectional study from January 2001 to December 2001 in the department of anatomy in collaboration with clinical pathology laboratory and outpatient diabetic clinics, Isra university, Hyderabad and department of physiology, university of Sindh and outpatients of Liaquat university of medicine and health Sciences, Hyderabad, Pakistan in a 490 T2DM patients and reported that frequency of blood group B was significantly higher whereas group O was significantly lower. A case control study also reported similar observation of higher frequency and interrelationship of blood group B among diabetic patients and the findings are consistent to this study and altered in the study done prospective cohort study showed blood group A with increased risk of diabetes mellitus. In the population of Pakistan, it was reported that blood group O has the highest distribution among diabetics. But a negative association was found between diabetes and blood group O in the study population, showing Blood group O was significantly less common in diabetic patients (38.5%), while it was higher in non-diabetics (44.5%). Another study conducted in India at the endocrinology department of the medical college and hospital in Kolkata discovered a higher relative risk for diabetic individuals with blood types AB, A, and B [36]. Studies regarding the association between ABO blood groups and type 2 diabetes mellitus are inconclusive. Some of the studies showed an association [37] while few studies showed evidence against presence of any association existing between ABO blood groups and type 2 diabetes mellitus [38]. This study showed patients having blood group B are more likely to have type 2 diabetes mellitus whereas blood group AB are less likely to have diabetes. Blood group B was strongly associated with incidence of T2DM in the study done in the department of physiology, surgery and medicine in King Saud university in Riyad, Saudi Arabia [39]. They also found out low association with blood group O which contradicted this study where blood group AB was the lowest in prevalence [40]. Another study done in Saudi Arabia did not find any association with Rhesus group and diabetes, unlike this study. Disparities might be due to different nature of the study carried out in the different types of races. Although there is considerable controversy about whether HbA1c is appropriate for diagnosis of (type 2) diabetes in which there occur slower with a more gradual increase in glucose levels over time. A continuum exists from health through to diabetes, from low risk through to high risk of complications, it is now explicitly accepted in many countries as a diagnostic test and for monitoring. The issue of day-to-day variability in glucose readings can be avoided with the use of HbA1c, and more crucially, it eliminates the requirement that the patient fast and make prior meal preparations [41]. In our study blood group B with type 2 diabetes mellitus was found to be more associated with complications followed by blood group A, O and AB respectively but with no significant association seen between blood group with or without complications which was supported by previous study on Punjabi population in Selangor, Malaysia showed Blood groups O and A were less likely to become obese than blood groups B and Rh positive, but blood groups AB were less likely to become obese [42,43].
- CONCLUSIONS
In this study 384 participants were involved in which 192 were type 2 diabetic patients (cases) whereas 192 were healthy population (control) irrespective of their blood glucose level or anti-diabetic medications were enrolled and subjected to blood tests for ABO-RH blood grouping. A comparative cross-sectional study about the association of ABO-RH blood group with T2DM was done. Although the studies from Nepal showed blood group O to be the most common and blood group AB to be the least common blood groups, the most common blood group in diabetic patients in this study was blood group B with highest male participants followed by blood group O, A and AB respectively. However, there was no significant association among the various ABO blood groups Similarly, RH positive was most common among diabetic patients i.e. 98% RH positive and 2% RH negative with significant association (P value < 0.05) between RH+ and RH- blood group. HbA1c among T2DM patients showed blood group A and B have got similar mean value with whereas on the basis of complications blood group group B have highest with no significant association seen between blood group with or without complications and patient are most on oral hypoglycaemic agent than insulin. Despite numerous studies addressing this issue, it is still unclear how ABO blood types relate to diabetes mellitus. The processes by which either the A or B antigens could alter the risk of DM have not been satisfactorily explained by any study. To solve this issue, more study is required. Based on the findings of the this study, it has been proposed that blood group B positive people in the areas need to pay special attention to T2DM because they are highly susceptible to the disease. People of other blood groups also need to pay special attention because they have high chances of developing complications from the disease.
REFERENCES
- Fauci AS. Harrison’s principles of internal medicine: McGraw-Hill Education; 2015.
- King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes care. 1998;21(9):1414-31.
- Anisha Shrestha, Archana Pandey Bista, Kalpana Paudel & Madhusudan Subedi (2024). Experiences of Nurses Regarding Caring Behavior in Intensive Care Units. Dinkum Journal of Medical Innovations, 3(07):483-492.
- Ahmed AM. History of diabetes mellitus. Saudi medical journal. 2002;23(4):373-8.
- Lakhtakia R. The history of diabetes mellitus. Sultan Qaboos University Medical Journal. 2013;13(3):368.
- Cooke DW, Plotnick L. Type 1 diabetes mellitus in pediatrics. Pediatrics in review. 2008;29(11):374-85.
- Kamil M, Ali Nagi Al-Jamal H, Mohd Yusoff N. Association of ABO blood groups with diabetes mellitus. Libyan Journal of Medicine. 2010;5(1):4847.
- Diabetes A. Association A, American PA. Diagnosis and Classification of Diabetes Mellitus Diabetes Care. 2013;36:S67-74.
- Association AD. Diagnosis and classification of diabetes mellitus. Diabetes care. 2010;33(Supplement_1):S62-S9.
- Rafael Angelo Cruz, Angelita E. Amoroso & Andre Angelo Tanque (2024). The Economic Impact of Care & Treatment of Diabetic Foot Ulcers at a Tertiary Government Hospital in the Philippines: A Retrospective Cohort Study. Dinkum Journal of Medical Innovations, 3(07):510-522.
- Paschou SA, Papadopoulou-Marketou N, Chrousos GP, Kanaka-Gantenbein C. On type 1 diabetes mellitus pathogenesis. Endocrine connections. 2018;7(1):R38-R46.
- Larsen CM, Faulenbach M, Vaag A, Vølund A, Ehses JA, Seifert B, et al. Interleukin-1–receptor antagonist in type 2 diabetes mellitus. New England Journal of Medicine. 2007;356(15):1517-26.
- Sandra Rumi Madhu (2024). A Study on Anemia in Adolescent Girls Due to Food Habit at Gazipur District in Bangladesh. Dinkum Journal of Medical Innovations, 3(06):469-482.
- Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature. 2007;447(7145):661-78.
- Todd JA, Walker NM, Cooper JD, Smyth DJ, Downes K, Plagnol V, et al. Robust associations of four new chromosome regions from genome-wide analyses of type 1 diabetes. Nature genetics. 2007;39(7):857-64.
- Cooper JD, Smyth DJ, Smiles AM, Plagnol V, Walker NM, Allen JE, et al. Meta-analysis of genome-wide association study data identifies additional type 1 diabetes risk loci. Nature genetics. 2008;40(12):1399-401.
- Atkinson MA, Maclaren NK. The pathogenesis of insulin-dependent diabetes mellitus. New England journal of medicine. 1994;331(21):1428-36.
- Vehik K, Hamman RF, Lezotte D, Norris JM, Klingensmith G, Bloch C, et al. Increasing incidence of type 1 diabetes in 0-to 17-year-old Colorado youth. Diabetes care. 2007;30(3):503-9.
- Dahlquist GG, Patterson C, Soltesz G. Perinatal risk factors for childhood type 1 diabetes in Europe. The EURODIAB Substudy 2 Study Group. Diabetes care. 1999;22(10):1698-702.
- Zahidur Rahman Khan & Dr. Sabrina Tymee (2024). Evaluation of Prognostic Role of Serum CRP in Acute Stroke Patients. Dinkum Journal of Medical Innovations, 3(06):460-468.
- Legese B, Abebe M, Fasil A, Schneider JG. Association of ABO and Rh Blood Group Phenotypes with Type 2 Diabetes Mellitus at Felege Hiwot Comprehensive Referral Hospital Bahir Dar, Northwest Ethiopia. International Journal of Chronic Diseases. 2020;2020:1-9.
- Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman medical journal. 2012;27(4):269.
- DeFronzo RA, Ferrannini E, Groop L, Henry RR, Herman WH, Holst JJ, et al. Type 2 diabetes mellitus. Nature reviews Disease primers. 2015;1(1):1-22.
- Sullivan PW, Morrato EH, Ghushchyan V, Wyatt HR, Hill JO. Obesity, inactivity, and the prevalence of diabetes and diabetes-related cardiovascular comorbidities in the US, 2000–2002. Diabetes care. 2005;28(7):1599-603.
- Stumvoll M, Goldstein BJ, Van Haeften TW. Type 2 diabetes: principles of pathogenesis and therapy. The Lancet. 2005;365(9467):1333-46.
- Md. Hasan Moshiur Shawon & Prof. Dr. Shanjoy Kumar Paul (2024). Risk Factors of Urinary Tract Infection Caused by Extended-Spectrum Beta-Lactamases-Producing Bacteria in Children . Dinkum Journal of Medical Innovations, 3(02):102-117.
- Kahn CR. Insulin action, diabetogenes, and the cause of type II diabetes. Diabetes. 1994;43(8):1066-85.
- Surendra Prasad Bhatta, Dr. Binita Pradhan & Dr. Pratibha Mishra (2024). Relationship between Screening and Diagnostic Performance of 50gm GCT vs. 75gm DIPSI test of Gestational Diabetes Mellitus: A Cross Sessional Study of Paten Hospital, Lalitpur. Dinkum Journal of Medical Innovations, 3(05):416-423.
- DeFronzo RA, Ferrannini E. Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes care. 1991;14(3):173-94.
- Buchanan TA, Xiang AH. Gestational diabetes mellitus. The Journal of clinical investigation. 2005;115(3):485-91.
- Abdul Mumin, Abdullah Al Amin, A.K.M. Shahriar Kabir, Rifat Ara Noor & Urmi Rahman (2024). Role of C- Reactive Protein (CRP) and Neutrophil Lymphocyte Ratio (NLR) in detecting severity & Predicting outcome of Acute Pancreatitis patients. Dinkum Journal of Medical Innovations, 3(01):01-12.
- Hosoi E. Biological and clinical aspects of ABO blood group system. The journal of medical investigation. 2008;55(3, 4):174-82.
- Eastlund T. The histo-blood group ABO system and tissue transplantation. Transfusion. 1998;38(10):975-88.
- Wiggins K, Smith N, Glazer N, Rosendaal F, Heckbert S, Psaty B, et al. ABO genotype and risk of thrombotic events and hemorrhagic stroke. Journal of thrombosis and haemostasis. 2009;7(2):263-9.
- Shovit Dutta (2024). Knowledge & Practice about Personal Hygiene among Primary School Students in Rural Chattogram, Bangladesh . Dinkum Journal of Medical Innovations, 3(02):72-88.
- D FARHUD D, Yeganeh MZ. A brief history of human blood groups. Iranian journal of public health. 2013;42(1):1.
- Guyton A, Hall J. Blood types; transfusion; tissue and organ transplantation. Guyton AC, Hall JE Textbook of Medical Physiology Eleventh Edition, Philadelphia. 2006:452-53.
- Gundrajukuppam DK, Vijaya SBK, Rajendran A, Sarella JD. Prevalence of principal Rh blood group antigens in blood donors at the blood bank of a tertiary care hospital in Southern India. Journal of Clinical and Diagnostic Research: JCDR. 2016;10(5):EC07.
- Anupama Sharma, Dr. Himanshu Shah & Dr. Vandana Mourya (2024). The evaluation of maternal morbidity and perinatal morbidity & mortality in Breech Delivery and Its Comparison with Mode of Delivery. Dinkum Journal of Medical Innovations, 3(02):89-101.
- Prabin Kumar Jha, Dr. Bindu Laxmi Shah, Dr. Shruti Kumari Thakur & Dr. Avinash Thakur (2024). Effectiveness of Dexamethasone as an Adjuvant to Bupivacaine in Supraclavicular Brachial Plexus Block. Dinkum Journal of Medical Innovations, 3(01):13-25.
- Daniels G. ABO, Hh and Lewis systems. Human blood groups. 2002:7-98.
- Pinkston JA, Cole P. ABO blood groups and salivary gland tumors (Alabama, United States). Cancer Causes & Control. 1996;7(6):572-4.
- Slater G, Itzkowitz S, Azar S, Aufses AH. Clinicopathologic correlations of ABO and Rhesus blood type in colorectal cancer. Diseases of the colon & rectum. 1993;36(1):5-7.Abro, S. U., Saleem, Q., Begum, A., Azhar, S., Naseer, A., & Qureshi, A. A. (2020). Association of BMI (Body Mass Index) to haemoglobin and red blood cell indices among adolescents. The Professional Medical Journal, 27(10), 2210-2215.
Publication History
Submitted: August 19, 2024
Accepted: August 28, 2024
Published: August 31, 2024
Identification
D-0312
DOI
https://doi.org/10.71017/djmi.3.8.d-0312
Citation
Muneshwor Sah, Ram Bahadur K.C, Prasanna Bahadur Amatya & Arati Kattel (2024). Association between Abo-Rh Blood Groups and Type-2 Diabetes Mellitus: Comparative Cross Sectional Study. Dinkum Journal of Medical Innovations, 3(08):619-629.
Copyright
© 2024 The Author(s).