

")
Publication History
Submitted: October 02, 2024
Accepted: October 20, 2024
Published: October 31, 2024
Identification
D-0339
DOI
https://doi.org/10.71017/djmi.3.10.d-0339
Citation
Ruhaima Issah Zorro & Amadu Baba (2024). High Antenatal Attendance, Low Facility Delivery: Assessment of Factors Influencing Facility Delivery in a University Hospital in Ghana. Dinkum Journal of Medical Innovations, 3(10):733-749.
Copyright
© 2024 The Author(s).
733-749
High Antenatal Attendance, Low Facility Delivery: Assessment of Factors Influencing Facility Delivery in a University Hospital in GhanaOriginal Article
Ruhaima Issah Zorro 1*, Amadu Baba 2
- Department Of Nursing and Midwifery, Faculty of Allied Health and Pharmaceutical Sciences, Tamale Technical University, Ghana.
- Department Of Nursing and Midwifery, Faculty of Allied Health and Pharmaceutical Sciences, Tamale Technical University, Ghana.
* Correspondence: iruhaima@tatu.ed.gh
Abstract: In Ghana, though there has been a decline in maternal mortality from 760 deaths per 100,000 live births in 1990 to 319 deaths per 100,000 live births in 2015, it is still very high. Complications that may arise from pregnancy are impossible to predict. Thus, World Health Organization (WHO) duly recommends delivery by a skilled birth attendant (SBA). This study is to access the factors contributing to the high ANC coverage, but low facility delivery in the Tamale Technical University Hospital. The study used analytical cross-sectional design to include 293 pregnant women attending ANC at Ta TU Hospital. Using simple random SPSS version 26 and STATA version 17 was used for data entry and analysis. The demographic characteristics of the respondents was analyzed and presented using descriptive statistics in the form of frequency and percentages. Logistic regression used to determine the factors contributing high ANC coverage but low skilled delivery. Age, education, previous pregnancy experience, presence of medical professionals, the desire to avoid complications, and the desire to reduce waiting time and medication costs were all found to be significant(p<0.001) Age, education, and previous pregnancy experience play significant roles in the preference for delivering at the hospital. Factors such as the presence of medical professionals, the desire to avoid complications, and the desire to reduce waiting time and medication costs are associated with a higher likelihood of choosing Ta TU Hospital for delivery. However, the study also identifies challenges in accessing the hospital during labor and highlights concerns related to staff confidence, cost, and facility resources as reasons for choosing alternative delivery locations. These findings indicate a need for improved healthcare infrastructure, staff training, and cost-related support to encourage facility-based deliveries.
Keywords: antenatal attendance, low facility delivery, influencing factors
- INTRODUCTION
Low-and middle-income countries (LMIC) contribute about 99% of the maternal deaths that occur worldwide [1]. An investigation into the factors that lead to maternal deaths in Africa reveals that the majority of these deaths are the result of direct obstetric complications, the most prominent of which are hemorrhage, hypertension, sepsis, and obstructed labor, all of which manifest themselves around the time of labor and delivery. However, it is possible to avoid loss of life due to these complications. The maternal mortality rate in Ghana is still quite high, despite the fact that it has decreased from 760 deaths per 100,000 live births in 1990 to 319 deaths per 100,000 live births in 2015. This represents a significant decrease. It is impossible to correctly predict the complications that may arise during pregnancy. Consequently, the World Health Organization (WHO) emphasizes the importance of having a skilled birth attendant (SBA) perform the delivery. There have been numerous summits and international conferences held all over the world, and the presence of an SBA at delivery has been anxiously re-echoed in each of these events. Numerous studies [2] have highlighted the significance of skilled delivery in terms of its impact on the reduction of mortality rates among pregnant women and newborns. Every year, there are more than 200 million conceptions that take place. Nevertheless, approximately forty percent of these conceptions go on to result in complications related to pregnancy among women all over the world [3]. Labor and delivery that takes place within medical facilities has been shown to be one of the most effective methods for reducing the risk of maternal mortality and morbidity, as well as for enhancing the health of newborns. Despite the fact that this is acknowledged, a sizeable proportion of births take place outside of medical facilities in countries with low incomes [4]. There are 830 maternal deaths that take place every single day around the world as a result of complications related to pregnancy and labor. This underutilization is one of the tragic consequences that causes these deaths. In addition, there are implications for infants when the delivery takes place outside of the facility. A total of 3.0 million neonatal deaths and 2.65 million stillbirths occurred around the world in 2008 [5], with the majority of these deaths occurring outside of health care facilities. Further, home delivery is linked with increased risk of third stage delivery issues including retained placenta, post- partum hemorrhage [6]. Ghana has a population of about 32 million and a population density of 124, with females accounting for about 51 % of the population with an estimated total fertility rate of 4. According to the Ghana Demographic and Health Survey (2014) report, inhabitants reside almost equally in urban and rural areas. In Ghana, health facilities administer health care through maternity homes, Community-based Health Planning and Services (CHPS) health post, public, private and mission hospitals. However, the distribution of these health care facilities is skewed in favor of the urban areas [7]. Consequently, nine out of ten women in Ghana have utilized ANC services from health professionals during their recent pregnancy. However, the high prevalence of ANC usage does not translate into the use of health facility for delivery. The 2014 Ghana Demographic and Health Survey (GDHS) report revealed that an overwhelming 97% of women received ANC at least once during their recent pregnancy, but 73% went on to deliver in a health facility where SBAs are available. According to a study [8], Skilled delivery in the Upper East Region of Northern Ghana is high (84.1%), though there are variations across the thirteen districts in the region. The 2014 annual report of the Bielsa district showed that an appreciable 71.5% of pregnant women received ANC services once during pregnancy, 90.7% made at least four follow up visits before delivery while only 46.2% delivered in a health facility. These findings on ANC utilization and health facility delivery put together demonstrate that a gap exists between receiving ANC services from health facilities and delivery in health facilities. The global expectation each day is that, about one thousand five hundred (1,500) maternal mortalities occur whilst five hundred and thirty-six thousand (536.000) maternal mortalities occur every year based on the World Health Organization report [9]. The lower income nations are recording majority of these maternal mortalities since the rate at which women become pregnant is higher as compared to the developed nations. Maternal mortalities recorded in the developed nations are as low as nine (9) per 100.000 live births as compared to four hundred and fifty (450) in the lower income nations. Undoubtedly the risk of maternal mortality in the lower income nations is higher than the developed nations [10]. The utmost health divisions between the developed countries and the underdeveloped countries are maternal mortality. About 99% of all maternal mortalities occur in the lower income nations worldwide [11]. However, African countries felt the highest burden of this tragedy thereby accounting for 40% of the world’s total maternal mortalities [12]. Uptake of skilled delivery is considered to be the panacea for decreasing both maternal deaths and diseases significantly [13]. Most nations where uptake of skilled delivery is greater than eighty percent (80%) have MMRs less than 200 [14]. This is attributed to the various developments of professional midwifery during the 20th century for the significant decrease in maternal mortalities in the developed nations [15]. Most of the pregnant women still utilize TBAs or relatives for skilled delivery service in the lower income nations. Traditional birth attendants are well respected in the communities they reside in Ghana because they attend to the pregnant women throughout pregnancy and child birth. The Ghana health services under the ministry of health previously built the capacity of existing traditional birth attendants and trained new ones to improve on early identification of health conditions and prompt referrals and safe deliveries devoid of complications and infections. The capacity building and the training of new ones came as a result of the shift toward community-based interventions when the 1987 International Safe Motherhood Initiative was introduced. This made the TBAs to be seen as ambassadors of mortality reduction for years [16]. Despite the training that was provided to TBAs, there was no significant improvement in the fight against maternal mortality, according to the findings of a number of studies conducted by the World Health Organization (WHO), the United Nations Population Fund (UNFPA), and the Ministry of Health. As a result, it is necessary to abandon the training of TBAs and instead focus on facility delivery by means of trained professionals and improved access to emergency obstetric care services in order to increase the rate of maternal survival. Delays by TBAs in some of the referrals have rather increased postpartum infections despite their training and capacity building. TBAs remain one of the most visited in most of the villages in Ghana despite the curtailment of their training [17]. The death of pregnant women in Ghana due to pregnancy related complications is still in the ascendency moving from 414 to approximately 560 per 100,000 live births [18]. Pregnancy outcomes mostly depend on the attitudes of skilled birth attendant since it plays a vital role complemented by cost, supposed quality of care and nearness to services. Therefore, uptake of skilled delivery is affected by the above-mentioned components of care thus both medical and non-medical either positively or negatively [19]. An author [20] found that despite the fact that care given to pregnant women during pregnancy helps in preventing diseases or early identification and management of diseases and also preparation toward childbirth, most pregnant women access it only when there is complications. It also detected that difficulty in accessing suitable care by pregnant women with complications at the appropriate facilities is due to lack of structured referral policies between the CHPS compounds or zones, health centers and hospitals [21]. Also, there are delays that occur at the various health facilities thus the time the clients report at the health facilities and when the needed services are rendered by the health professionals [22]. Moreover, lack of logistics, medications, health apparatus and health professionals result in the lackadaisical attitude and haphazard response to obstetric emergencies at the health centers during uptake of skilled delivery. An author [23] found that the main demotivating factor towards uptake of skilled delivery is the way health professionals behave toward the clients. For instance, the inhumane, unprofessional and rude treatment clients receive from health professionals deters them from uptake of skilled delivery and even do not recommend facility delivery to others because of what they experienced at the facility before. An author [24] for instance found that discouragement of birth preparedness by the Swahili culture since it is believed that birth preparedness could lead to obstetric complication for instance stillbirth hence influencing facility delivery. That is why this study assess the factors contributing to uptake of skilled delivery. Additionally, understanding what informs decisions on place of delivery, the preferred health care professional to attend to or TBA so that it will update the policy makers and the health professional on the best policies and interventions to make and implement. This study is to assess the factors contributing to the high ANC coverage, but low facility delivery in the Tamale Technical University Hospital, to assess the socio-cultural factors influencing facility delivery, to find out the attitudes of health staff towards clients during delivery services, to assess women’s knowledge level about the significance of facility delivery.
- MATERIALS & METHOD
Sagnarigu, which is located in the Northern Region of Ghana, is the location of the Tamale Technical University Hospital. On November 17th, 2017, it formed itself as a company. Additionally, it provides services for both in-patients and out-patients. The inhabitants of the facility and those in the nearby area experienced a sense of relaxation as a result of its operation. The outpatient department (OPD), the emergency unit, the reproductive and child health (RCH) unit, the disease control and prevention unit, the nutrition department, the maternity department, the pharmacy, the male ward, the female ward, the pediatric ward, the laboratory, and finally the stores are all elements that make up this facility. This means that it offers a wide range of services to its customers. The study utilized a quantitative research methodology and utilized an analytical cross-sectional design. The majority of the participants in the study were women who were in their reproductive age (WIFA), which refers to women who were between the ages of 15 and 49 and who had children between the ages of 0 and 12 months old as well as pregnant women. Key informant interviews by purposive selection of health staff who conduct deliveries and have in depth knowledge on skilled delivery care and services were conducted. The Sample Size was determine using the Cochran (1977) formulae below
Where;
z = the value for the given confidence interval =90% or 1.645
d = margin of error; = 10%
p = proportion of skilled delivery = 26 % (0.26)
q = (1-p) and n = Base sample size required = (1- 0.26) = 0.74
Pregnant Women
A method of sampling that was chosen at random was utilized in order to pick the respondents at the hospital area. It was necessary to employ this method in order to eliminate any possibility of sample bias. We continued to collect data until we reached a point of saturation, at which point responses were being repeated and no new information was being brought to light. Obtaining the data for the study came from primary sources. The primary data for the study consisted of information that was acquired at firsthand from the individuals who participated in the survey. The information that was acquired from the interactions with all of the people that were visited or encountered during the course of the study is included in this. More specifically, they were women who were of reproductive age and healthcare personnel in general, particularly nurses and midwives who were responsible for delivering babies. The use of questionnaires was crucial in the collection of these insights. A well-crafted questionnaire served as the primary instrument for the collection of data from the field. The questionnaire had a structured format and had questions with limited room for open-ended responses in order to facilitate the process of responding to the questionnaire. However, because the bulk of the population was illiterate, it was not possible for them to self-administer the information. During an interview, the researcher, with the assistance of a group of assistants, delivered it to the individuals who participated in the study. In addition, there were a few questions that were open-ended, which gave respondents the opportunity to openly express their viewpoint on the subject matter to the extent that it was required. Throughout the questionnaire, there were sections that were intended to reflect the subtopics that were being investigated. Additionally, there were interviews that were not just structured but also directed by carefully crafted interview guides. I used SPSS (Statistical Package for Social Sciences, Version 26) to perform the analysis on the data collected in the field. The quality of the data was ensured by the researcher by first evaluating the accuracy of the questions and the manner in which the respondents answered them. This was done to ensure that only responses that were pertinent to the questions were obtained. Before the questions were entered into the software for processing, any extraneous variables that were discovered as responses to any question or questions were modified accordingly. Self-discipline and the ethics of data management were closely adhered to, which ensured that only replies received from the field were coded and entered into the system. Additionally, the analyst’s own judgment was not taken into consideration during the process of entering the data. From the data collected in the field, a descriptive analysis was carried out, and logical deductions were drawn with reference to the previously examined literature. We made use of frequency distribution in order to improve interpretations wherever it was required. Delivery by a Qualified Health practitioner: The dependent variable in this study is delivery by a qualified health practitioner. The socio-cultural factors that are considered include men and in-laws as decision makers about the location of the delivery; burial rites for the placenta; perceptions of unfaithfulness on the part of women as a result of problems or delayed delivery; and the lack of involvement of men and other family members in matters pertaining to mothers. In addition, the research utilized proper research processes and conducts, and it followed a sequential structure, which is considered to be acceptable in the field of research. It was also possible for the target respondents, who were expecting moms, as well as the public health nurse and the midwives, to participate in the survey on purpose. This assisted in preventing the likelihood of induced responses from the staff members, which in turn helped to strengthen the validity of the findings achieved. There was complete anonymity and confidentiality of the data obtained.
- RESULTS & DISCUSSION
Table 01 show the distribution of the demographic characteristics of the respondents. According to the data, the respondents can be divided into four distinct age groups. The age group that makes up the largest portion of the sample is the 26-35 age group, which accounts for 37.5% of the total, followed by the 36-45 age group, which accounts for 29.4%. 18% of the respondents are between the ages of 18 and 25, and 14.3% of the respondents are between the ages of 46 and 55. Based on this distribution, it appears that the majority of the sample is comprised of individuals who are of working age, with a sizeable proportion of them being in their late twenties to mid-thirties. The respondents’ educational attainment is reflected in the education category of the survey. Seventy-seven point five percent of respondents have completed secondary education, making it the most prevalent degree of education. Next in line is tertiary education, which accounts for 19.5% of the total population. 24.6% of the population has completed primary school, while 18.4% of the population has not completed any formal education. Taking into account this distribution, it can be seen that the sample contains individuals with a rather varied range of educational backgrounds, with a sizeable proportion having completed at least secondary school. The respondents’ employment situations are highlighted in the occupation category of the survey instrument. Those who are self-employed make up the largest group, accounting for 41.6% of the sample, followed by those who are working part-time, which accounts for 15.0%. The percentage of people who are employed full-time is 9.6%, while the percentage of people who are students and those who are jobless is 8.9% and 24.9%, respectively. Based on the statistics, it appears that there is a wide range of occupational statuses, with a significant number of individuals working part-time and as self-employed individuals.
Table 01: Socio-demographic characteristics of respondents
| Characteristics | Frequency | Percentage (%) |
| Age | ||
| 18-25 | 55 | 18.8% |
| 26-35 | 110 | 37.5% |
| 36-45 | 86 | 29.4% |
| 46+ | 42 | 14.3% |
| Education | ||
| No formal education | 54 | 18.4% |
| Primary education | 72 | 24.6% |
| Secondary education | 110 | 37.5% |
| Tertiary education | 57 | 19.5% |
| Occupation | ||
| Employed (full-time) | 28 | 9.6% |
| Employed (part-time) | 44 | 15.0% |
| Self-employed | 122 | 41.6% |
| Student | 26 | 8.9% |
| Unemployed | 73 | 24.9% |
| Marital Status | ||
| Divorced | 12 | 4.1% |
| Married | 281 | 95.9% |
| No. of Children | ||
| One | 73 | 24.9% |
| Two | 150 | 51.2% |
| Three or more | 70 | 23.9% |
During their current pregnancy, the respondents attended ANC at a rate of nearly 97% (96.6%), while only 2.7% did not attend as part of their pregnancy. In accordance with global health standards, which highlight the significance of antenatal care (ANC) in ensuring the health of both the mother and the baby during pregnancy, this high ANC attendance rate is compatible with those recommendations. There have been a number of studies and guidelines that highlight the benefits of regular ANC visits in terms of lowering the incidence of maternal and newborn mortality. A sizeable proportion of the respondents underwent several visits to the ANC: 32.8% of them went there two to three times, 39.9% went there four to six times, and 23.9% went there seven times or more. The aforementioned statement is in accordance with the established norms that require a minimum of four visits to the ANC during a healthy pregnancy. The findings of this survey indicate that a sizeable proportion of the population that participated in the research followed these guidelines. The biggest reasons for attending ANC were to monitor the health of the baby (60.8% of pregnant women) and to have routine checkups (29.7% of pregnant women). This is consistent with the primary goals of antenatal care, which include monitoring the health of the mother as well as the developing fetus, as well as recognizing and treating any potential issues that may arise.
Table 02: Antenatal Care at Tamale Technical University Hospital
| Characteristics | Frequency | Percentage (%) |
| ANC attendance (current pregnancy) | ||
| No | 8 | 2.7% |
| Yes | 283 | 96.6% |
| No. ANC visit at TaTU Hospital | ||
| Once | 10 | 3.4% |
| 2-3 times | 96 | 32.8% |
| 4-6 times | 117 | 39.9% |
| 7 or more times | 70 | 23.9% |
| Reason for ANC | ||
| Getting advice and information | 3 | 1.0% |
| Monitoring the baby’s health | 178 | 60.8% |
| Receiving vaccination | 25 | 8.5% |
| Routine check-ups | 87 | 29.7% |
| Information of facility delivery | ||
| No | 24 | 8.2% |
| Yes | 269 | 91.8% |
| Encouragement on Facility delivery | ||
| No | 58 | 19.8% |
| Yes | 235 | 80.2% |
| ANC education | ||
| No | 78 | 26.6% |
| Yes | 215 | 73.4% |
| Education of home delivery risk | ||
| No | 76 | 25.9% |
| Yes | 217 | 74.1% |
72.7% of the respondents gave birth to their child at a location other than TaTU Hospital, while 27.3% gave birth in TaTU Hospital. It appears from this that the majority of the respondents chose to have their babies delivered outside of a hospital setting. People who did not give birth at TaTU Hospital listed the following as the key reasons for their decision: a lack of faith in the hospital’s staff (69.5%), the cost of delivery services (11.7%), the distance to the hospital (18.8%), and a preference for giving birth at home (2.8% each). Many variables, including family members (49.3%), joint decision (23.0%), and self-determination (27.7%), played a role in the decision to deliver the baby outside of the hospital.
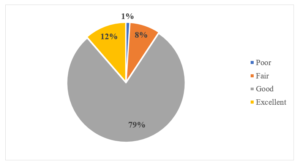
Figure 01: Overall Delivery Experience
Perceived advantages of facility delivery included Access to medical professionals (43.0%), Availability of necessary equipment (11.6%), Clean and sterile environment (1.0%), Emergency care in case of complications (44.4%) The following are some of the perceived drawbacks of facility delivery: the high expense of delivery (one percent), the absence of customized care (forty-three percent), and the distance from home (eleven point six percent). Facilities and resources that are insufficient (44.4%). It appears from the statistics that a sizeable proportion of respondents made the decision to give birth to their kid at a location other than Ta TU Hospital. This decision was mostly motivated by a lack of trust in the personnel at the hospital as well as financial reasons. In the process of deciding whether or not to have the baby delivered outside of the home, family members had a crucial influence. It seems that some of the respondents have a tough time gaining access to Ta TU Hospital while they are in labor, while others did not have any substantial difficulty.
Table 03: Respondents knowledge on the importance of facility delivery
| Characteristics | Frequency | Percentage (%) |
| Place of delivery of Child | ||
| Ta TU Hospital | 80 | 27.3% |
| Elsewhere | 213 | 72.7% |
| Reason for Not delivering at TaTU hospital | ||
| Cost of delivery services | 25 | 11.7% |
| Lack of confidence in the hospital’s staff | 148 | 69.5% |
| Distance to the hospital | 40 | 18.8% |
| Preference for home birth | 6 | 2.8% |
| Decision for Outside delivery | ||
| Family members | 105 | 49.3% |
| Joint decision | 49 | 23.0% |
| Myself | 59 | 27.7% |
| Challenges in Accessing the Ta TU Hospital during labor | ||
| No | 40 | 50.0% |
| Yes | 40 | 50.0% |
| Overall experience | ||
| Excellent | 33 | 11.3% |
| Fair | 24 | 8.2% |
| Good | 230 | 78.5% |
| Poor | 3 | 1.0% |
| Advantage of facility delivery | ||
| Access to medical professionals | 126 | 43.0% |
| Availability of necessary equipment | 34 | 11.6% |
| Clean and sterile environment | 3 | 1.0% |
| Emergence care in case of complications | 130 | 44.4 % |
| Disadvantage of facility delivery | ||
| High cost of delivery | 3 | 1.0% |
| Lack of personalized care | 126 | 43.0% |
| Distance from home | 34 | 11.6% |
| Inadequate facilities/resources | 130 | 44.4% |
Figure 01 is a pareto bar chart that illustrates the order in which the criteria that determined whether or not to deliver at Ta TU Hospital were considered. The majority of respondents choose to give birth at Ta TU hospital due to its closeness to the hospital, followed by receiving a referral from Ta TU personnel, then being able to afford the service, then having a positive reputation of the staff, and finally having the necessary equipment available.
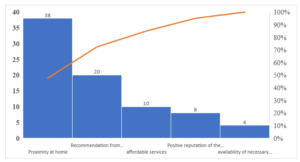
Figure 02: Factors influencing Decision to Deliver at Ta TU Hospital
The fact that the F-statistic for the model is 8.70, with 5 and 288 degrees of freedom for the residuals, respectively, and that the related p-value (Prob > F) is extremely close to zero (0.0000) indicates that the entire model is statistically significant at the level of statistical significance. R squared is a statistical measure that indicates the extent to which the independent variables (predictors) in the model are responsible for explaining the overall variation in the dependent variable (response). The R-squared value is around 0.1329, which indicates that the model accounts for roughly 13.29% of the variability in the response variable according to the data.
Table 04: Regression Model Summary
| Source | SS | Df | MS | Number of Obs / F (5,293) | 293/8.70 |
| Model | 7.51348817 | 5 | 1.50269763 | Prob > F | 0.0000 |
| Residual | 49.0416842 | 284 | .172681987 | R-squared/Adj. R square | 0.1329/0.1176 |
| Total | 56.5551724 | 289 | .195692638 | Root MSE | .41555 |
Through the use of multiple linear regression, a total of 293 women who were attending antenatal care at Tamale Technical University Hospital were analyzed in order to establish the factors that influence their preference for birth at the hospital. Based on the findings of the survey, it was determined that age was a statistically significant factor (F=4.58, P-value=0.000, 95%CI (0.07494-0.18805). Given that the coefficient for age is 0.132, it can be deduced that the preference for delivery at Ta TU Hospital is anticipated to increase by 0.132 units on average for every one-unit increase in age. A statistically significant relationship was also discovered between education and the variables (F=2.66, P-Value=0.008, 95%CI (0.0175-0.11773)). Education has a coefficient of 0.068 in this equation. Based on this information, it can be inferred that the preference for delivery at Ta TU hospital is anticipated to increase by an average of 0.068 units for every one-unit increase in educational level. According to Stephenson and Tsui (2002), who conducted a study in which they discovered that a sizeable proportion of women who had completed at least secondary school were associated with facility delivery, these findings are in agreement with the findings of a number of other researchers. At the Ta TU hospital, however, occupation did not appear to be a significant predictor of delivery. With a 95% confidence interval of -0.03052, 0.05404, the T-test was 0.55, and the P-value was 0.585. Based on this information, it appears that occupation does not appear to be a statistically significant predictor of delivery among pregnant women who are attending ANC at Ta TU Hospital. There is no significant correlation between marital status and the likelihood of giving birth at Ta TU hospital. The t-statistics were 0.90, the p-value was 0.371, and the 95% confidence interval was (-0.36276, 0.13580). Marital Status has a coefficient of -0.113, which is negative. A decline in the preference for delivery at Ta TU hospital is connected with being married, according to the negative coefficient, which shows that this preference is negative. In terms of the variable that represents the number of children, the coefficient is 0.046. According to this, it is anticipated that the dependent variable will increase by an average of 0.046 units for every new child that is added to the population. On the other hand, the t-statistic is 1.49, and the p-value is 0.138, which indicates that the Number of Children variable does not meet the criteria for statistical significance at the usual significance level of 0.05. The fact that the confidence interval for 95% contains 0 lends credence to this conclusion.
Table 05: Multiple Linear Regression demographic factors influencing preference to delivery at Ta TU hospital
| Delivering at Ta TU Hospital | Coef. | Std. Err. | T | P>t | 95% CI | |
| Age | .132 | .028 | 4.58 | 0.000 | .07495 | .18805 |
| Education | .068 | .025 | 2.66 | 0.008 | .01751 | .11773 |
| Occupation | .012 | .021 | 0.55 | 0.585 | -.03052 | .05404 |
| Marital status | -.113 | .126 | -0.90 | 0.371 | -.36276 | .13580 |
| No of Children | .046 | .031 | 1.49 | 0.138 | -.01483 | .10651 |
| _cons | 1.322 | .308 | 4.29 | 0.000 | .71646 | 1.929 |
The regression model appears to be statistically significant (F-statistic=6.40, p-value=0.000), and it explains a substantial proportion of the total variation in the response variable (R-squared is relatively high at 0.3726). R-squared is approximately 0.3726, indicating that the model explains about 37.26% of the variability in the response variable
Table 06: Regression Model Summary
| Source | SS | Df | MS | Number of obs / F (23, 248) | 272/6.40 |
| Model | 20.0699976 | 23 | .87260859 | Prob > F | 0.0000 |
| Residual | 33.7976495 | 248 | .136280845 | R-squared/Adj RS | 0.3726/0.3144 |
| Total | 53.8676471 | 271 | .198773605 | Root MSE | .36916 |
There is a 39.5% increase in the likelihood of delivering at Ta Tu Hospital when there is a medical professional engaged, provided that all other variables remain unchanged. The fact that the coefficient is positive implies that there is an increase in the likelihood of selecting Ta Tu Hospital for delivery when there is a medical expert present. According to the t-statistic (t): -4.21, the p-value is less than 0.001, and the 95% confidence interval is between -0.5799 and -0.2101. This effect is statistically significant. There does not appear to be a statistically significant relationship between the availability of equipment and the possibility of delivering a baby at Ta Tu Hospital. The coefficient is negative, but it does not differ from zero statistically (p = 0.139). The t-statistic (t) is -1.48, and the 95% confidence interval (CI) is [-0.2014, 0.0283]. The presence of emergency care does not appear to have a statistically significant impact on the likelihood of delivering at Ta Tu Hospital (p = 0.185), t-statistic (t): -1.33, and 95% Confidence Interval (95% CI): [-0.1898, 0.0368]. This is similar to the situation with the availability of equipment. On the other hand, it does not appear that a clean environment has a statistically significant effect on the chance of selecting Ta Tu Hospital for delivery (p = 0.575), t-statistic (t): 0.56, and 95% Confidence Interval (95% CI): [-0.0756, 0.1358]. (p = 0.552), the t-statistic (t): -0.60, and the 95% confidence interval (CI): [-0.1637, 0.0876] indicate that supportive personnel does not have a statistically significant impact on the likelihood of hospital delivery. It does not appear that the high cost of service has a significant impact on the chance of selecting Ta Tu Hospital for delivery (p-value = 0.347), t-statistic (t): 0.94, and 95% confidence interval (CI): [-0.0744, 0.2111]. According to the p-value, which is 0.376, a lengthy waiting time does not have a statistically significant impact on the hospital preference for delivery. t-statistic (t): 0.89 (95% confidence interval [CI]: [-0.0575, 0.1517]). Distance does not appear to have a statistically significant effect on the likelihood of delivering at Ta Tu Hospital (p = 0.177), t-statistic (t): 1.35 (95% CI): [-0.0332, 0.1794. The t-statistic (t): 0.87, with a 95% confidence interval of [-0.0678, 0.1756], showed that the perception of inadequate facilities does not have a statistically significant impact on the likelihood of delivering the baby in a hospital setting (p-value = 0.384). The fear of losing the baby has a p-value of 0.053, which indicates that it has a marginally significant effect on the likelihood of giving birth in a hospital. This suggests that it may have some influence, but it’s not highly statistically significant. t-statistic (t): 1.94 (95% CI): [-0.0015, 0.2303]. Coefficient (Coef.): 0.114 indicate that, for every unit increase in fear of losing unborn child increases preference of delivering at Ta TU hospital by 0.114. Avoidance of complications has a significant and positive effect on the likelihood of delivering at Ta Tu Hospital (p < 0.001). The odds of choosing Ta Tu Hospital increase by approximately 28.1% when individuals want to avoid complications. t-statistic (t): 4.64, 95% CI): [0.1619, 0.4010]. the Coefficient of 0.281 indicates that, for every unit increase in avoidance of complications will increase the chance of delivery at Ta TU hospital by 0.281. The desire to reduce waiting time significantly increases the likelihood of hospital delivery (p < 0.001). Individuals who want to reduce waiting time are approximately 20.5% more likely to choose Ta Tu Hospital. t-statistic (t): 3.69 p-value (P>t): 0.000) and (95% CI): [0.0956, 0.3145]. Wanting to reduce the cost of medication significantly increases the likelihood of hospital delivery (p < 0.001). Those who aim to reduce medication costs are approximately 35.0% more likely to choose Ta Tu Hospital. t-statistic (t): 5.83p-value= 0.000, (95% CI): [0.2322, 0.4694]. The desire for more trained staff does not significantly affect the likelihood of hospital delivery (p = 0.894). t-statistic (t): -0.13. p-value = 0.894 95%, (95% CI): [-0.1305, 0.1139]. The absence of antenatal care (ANC) visits does not significantly impact the likelihood of hospital delivery (p = 0.771), t-statistic (t): 0.29, p-value = 0.771, (95% CI): [-0.0630, 0.0849]. The reason for ANC visits has a marginally significant effect on hospital delivery choice (p = 0.124). It may have some influence, but it’s not highly statistically significant. t-statistic (t): 1.54, p-value = 0.124, (95% CI): [-0.0118, 0.0982]. The availability of ANC information does not significantly impact the likelihood of hospital delivery (p = 0.410), t-statistic (t): -0.83, p-value=0.410, (95% CI): [-0.1679, 0.0687]. Facility delivery encouragement has a positive effect on the likelihood of hospital delivery, but it’s not statistically significant at the conventional significance level (p = 0.206). t-statistic (t): 1.27, (95% CI): [-0.0419, 0.1937]. the Coefficient of 0.075 means that, a unit increase in encouragement of pregnant women to deliver at Ta TU hospital increases the chance of delivering at Ta TU hospital by 0.075.
Table 07: Multiple Linear regression on factors influencing delivery at Ta TU Hospital
| Delivery at Ta Tu Hospital | Coef. | Std. Err. | t | P>t | 95% CI | |
| Medical professional | -.395 | .093 | -4.21 | 0.000 | -.5799 | -.2101 |
| Availability of equipment | -.086 | .058 | -1.48 | 0.139 | -.2014 | .0283 |
| Emergency care | -.076 | .057 | -1.33 | 0.185 | -.1898 | .0368 |
| Clean environment | .030 | .053 | 0.56 | 0.575 | -.0756 | .1358 |
| Supportive staff | -.038 | .063 | -0.60 | 0.552 | -.1637 | .0876 |
| High cost of service | .068 | .072 | 0.94 | 0.347 | -.0744 | .2111 |
| Long waiting time | .047 | .053 | 0.89 | 0.376 | -.0575 | .1517 |
| Distance | .073 | .054 | 1.35 | 0.177 | -.0332 | .1794 |
| Inadequate facilities | .053 | .062 | 0.87 | 0.384 | -.0678 | .1756 |
| Fear of losing baby | .114 | .058 | 1.94 | 0.053 | -.0015 | .2303 |
| Avoidance of complication | .281 | .060 | 4.64 | 0.000 | .1619 | .4010 |
| Reduce waiting time | .205 | .055 | 3.69 | 0.000 | .0956 | .3145 |
| Reduce cost of medication | .350 | .060 | 5.83 | 0.000 | .2322 | .4694 |
| More trained staff | -.008 | .062 | -0.13 | 0.894 | -.1305 | .1139 |
| No ANC Visits | .010 | .037 | 0.29 | 0.771 | -.0630 | .0849 |
| Reason for ANC | .043 | .0279 | 1.54 | 0.124 | -.0118 | .0982 |
| ANC information | -.049 | .060 | -0.83 | 0.410 | -.1679 | .0687 |
| Facility delivery encouragement | .075 | .059 | 1.27 | 0.206 | -.0419 | .1937 |
| _cons | 1.750 | .409 | 4.28 | 0.000 | .9446 | 2.5569 |
12.44 is the value of the F-statistic, and the model and residuals each have 9 and 226 degrees of freedom, separately. There is a strong indication that the whole model is statistically significant because the accompanying p-value (Prob > F) is extremely near to zero (0.0000).The proportion of the overall variance in the dependent variable (response) that can be attributed to the independent variables (predictors) described in the model is denoted by the symbol -squared. The R-squared value is roughly 0.3312, which indicates that the model accounts for approximately 33.12% of the variability in the response variable. In light of the fact that the p-value for the F-statistic is quite low, the regression model seems to be statistically significant. Furthermore, it explains a moderate part of the overall variation in the response variable (the R-squared value is roughly 0.3312).
Table 08: Regression Model Summary
| Source | SS | df | MS | Number of obs/ F (9, 226) | 236/12.44 |
| Model | 13.052 | 9 | 1.450 | Prob > F | 0.0000 |
| Residual | 26.353 | 226 | .1166 | R-squared/Adj RS | 0.3312/0.3046 |
| Total | 39.406 | 235 | .1676 | Root MSE | .34148 |
In the event that all other factors remain unchanged, individuals who have previously given birth have a probability of delivering their babies at Ta TU Hospital that is roughly 0.297 times higher than those who have not previously given birth. Statistically significant (p < 0.001), the t-statistic (t) is 4.43, and the 95% confidence interval (CI) is between 0.165 and 0.429.Women who want to give birth to their child at a location other than Ta TU Hospital are roughly 0.263 times less likely to choose Ta TU Hospital as their place of delivery as compared to women who want to give birth at Ta TU Hospital. The t-statistic (t) for this effect is -2.48, and the 95% confidence interval (confidence interval) for it is [-0.472, -0.054]. This effect is statistically significant (p = 0.014). With a t-statistic (t) of -1.26 and a 95% confidence interval (CI) of [-0.210, 0.046], it would seem that the existence of problems in pregnancy does not appear to have a statistically significant effect on the likelihood of delivering at Ta TU Hospital (p = 0.209). Individuals who have a positive perception of maternal health policies are roughly 0.284 times more likely to give birth at Ta TU Hospital in comparison to individuals who do not have such a perception. With a p-value of less than 0.001, this effect is highly statistically significant., the t-statistic (t) was 6.51, and the 95% confidence interval (CI) was [0.198, 0.370]. A t-statistic (t) of -1.52 indicates that the perception of maternal health care does not have a statistically significant effect on the likelihood of giving birth at Ta TU Hospital (p = 0.130). The 95% confidence interval for this finding is as follows: [-0.178, 0.023]. On the basis of the t-statistic (t): 0.91 and the 95% confidence interval (CI): [-0.165, 0.445], it would suggest that the attitude of the staff does not have a statistically significant impact on the likelihood of delivering at Ta TU Hospital (p = 0.366). The t-statistic (t): -0.01, with a 95% confidence interval (CI) of [-0.122, 0.121], indicates that the cost of delivery does not have a statistically significant impact on the chance of selecting Ta TU Hospital as the location for delivery (p = 0.991). With a t-statistic (t) of 0.23 and a 95% confidence interval (CI) of [-0.081, 0.102], it would suggest that the availability of transport does not have a statistically significant impact on the likelihood of giving birth at Ta TU Hospital (p = 0.815). There is a slightly significant relationship between the perceived benefits of hospital delivery and the likelihood of giving birth at Ta TU Hospital (p = 0.056) according to the correlation coefficient. According to this, those who have a greater perception of the advantages of hospital delivery may be more likely to select Ta TU Hospital as their hospital of choice. t-statistic (t): 1.92 (95% confidence interval [CI]: [-0.000, 0.008]). The coefficient of 0.004 suggests that the likelihood of delivery in Ta TU hospital increases by 0.004 for every unit increase in the perceived advantage of hospital delivery on the other hand. For the purpose of determining the likelihood of giving birth at Ta TU Hospital, there are a number of factors that are statistically significant. Having a previous pregnancy, the location where an individual would like to give birth to their kid, and their impression of the rules that govern maternal health are some of the factors that are considered. The perceived advantages of giving birth in a hospital can have a marginally significant impact on the outcome. It would indicate that other considerations, such as problems during pregnancy, perceptions of maternal health services, attitudes of staff members, the cost of delivery, and the availability of transportation, do not appear to have a substantial impact on the decision to give birth in a hospital.
Table 09: Multiple Linear regression on other factors influencing delivery at Ta TU Hospital
| Delivering at Ta TU Hospital | Coef. | Std. Err. | t | P>t | 95% CI. | |
| Previous pregnancy | .297 | .067 | 4.43 | 0.000 | .165 | .429 |
| Place wish to deliver a child | -.263 | .106 | -2.48 | 0.014 | -.472 | -.054 |
| Complication in pregnancy | -.082 | .065 | -1.26 | 0.209 | -.210 | .046 |
| Maternal health policies | .284 | .043 | 6.51 | 0.000 | .198 | .370 |
| Maternal health service | -.077 | .051 | -1.52 | 0.130 | -.178 | .023 |
| Staff attitude | .140 | .155 | 0.91 | 0.366 | -.165 | .445 |
| Cost of delivery | -.001 | .062 | -0.01 | 0.991 | -.122 | .121 |
| Transport availability | .012 | .047 | 0.23 | 0.815 | -.081 | .102 |
| Benefits of Hospital Delivery | .004 | .002 | 1.92 | 0.056 | -.000 | .008 |
| _cons | .675 | .491 | 1.37 | 0.171 | -.292 | 1.641 |
DISCUSSION
The finding that age is a statistically significant predictor of preference for delivery at Tatu Hospital (p-value = 0.000) aligns with research such as the 2014 Ghana Demographic and Health Survey (GDHS) [25]. According to the fact that the coefficient for age is positive, it can be deduced that there is an anticipated rise in the preference for giving birth at Tatu Hospital as the age of the individual grows. There is a prevalent notion that older moms tend to seek safer delivery alternatives, and this finding shows that older women may be more likely to choose facility-based deliveries. This findings are in keeping with the common thinking. According to previous research, including that conducted by Stephenson and Tsui (2002), the significance of education (p-value = 0.008) in affecting preference for delivery at Tatu Hospital is consistent with the findings of the current study. Based on the fact that the coefficient for education is positive, it can be deduced that there is a direct correlation between the amount of education and the preference for facility-based delivery. According to this conclusion, education plays a significant role in increasing awareness about the advantages of having a skilled attendant present during childbirth and in making healthcare facilities more accessible [26]. That occupation is not a significant predictor of delivery at Tatu Hospital (p-value = 0.585) is consistent with the findings of some research that have discovered that occupation does not have a major impact on the decisions that mothers make regarding their healthcare. Given these information, it appears that employment status might not be a significant determinant in the decision to deliver at a certain facility. According to the findings of [27], which revealed that marital status does not have a significant association with skilled attendance, the conclusion that marital status is not a significant predictor of delivery at Tatu Hospital (p-value = 0.371) is consistent with [27]. The fact that the coefficient is negative, on the other hand, suggests that getting married is connected with a drop in the preference for delivering at Tatu Hospital. This may be paradoxical, and more examination into this phenomenon may be beneficial. That the number of children in a household does not have a major impact on the decision to give birth at Tatu Hospital is suggested by the fact that the result indicates that the number of children is not a statistically significant predictor of delivery preference (p-value = 0.138). Other studies have found that the number of children is a significant determinant in maternal healthcare decisions [28], but this study contradicts those findings. When medical experts are present, there is a significant increase in the likelihood of selecting Tatu Hospital as the location for birth (p0.001). Several research have shown that skillful attendance at birth, which is provided by medical experts, is a significant factor in determining the health outcomes of both the mother and the newborn [29]. This finding is consistent with other studies. Because having access to professional care during delivery is associated with decreased rates of maternal and newborn death, it is an essential component in the decision-making process for maternal healthcare. There is a considerable rise in the likelihood of selecting Tatu Hospital for delivery (p < 0.001), since the desire to reduce waiting time and medicine expenses is a key factor. This aligns with the findings of research that suggests that considerations such as cost and convenience can have a significant impact on the decisions that are made about maternal healthcare. Reducing the amount of time that pregnant women have to wait and the amount of money that they have to spend on medicine are both appealing incentives that encourage them to choose facility-based delivery [30]. Some aspects, such as the availability of equipment, the presence of emergency care, a clean atmosphere, supportive personnel, high cost of service, long waiting time, distance, and the perception of poor facilities, do not have a statistically significant impact on the process of selecting a hospital for the delivery of a baby. The lack of significance may be related to particular contextual elements that were not captured in the research, despite the fact that some of these findings may come as a surprise to some individuals. Concerns about the possibility of losing the baby and the reasons for going to the ANC are examples of factors that have a moderately significant impact on the decision to deliver the baby in a hospital. In light of these findings, it appears that these factors might have some influence; however, the relevance of these factors might be contingent on other contextual variables that were not investigated in the study. There is a significant difference (p < 0.001) between the persons who had a previous pregnancy and those who do not have a previous pregnancy who are approximately 0.297 times more likely to deliver at Ta TU Hospital. It would appear from this that previous experiences with pregnancy play a role in determining the selection of Ta TU Hospital as the location for delivery. For nulliparous women, it is not uncommon for them to prefer facility-based births [31], despite the fact that this finding is in line with the concept that prior experience may raise a person’s level of comfort with a specific healthcare facility. In terms of the possibility of giving birth at Ta TU Hospital, it does not appear that the existence of problems in pregnancy has a statistically significant impact on those odds. Compared to the findings of other research, which have demonstrated that problems during pregnancy frequently cause women to choose to give birth in a facility due to the necessity of receiving emergency obstetric care [32], this specific study contradicts those findings. In this particular instance, the lack of significance may be due to the circumstances. Approximately 0.284 times more likely to give birth at Ta TU Hospital are individuals who have a positive perception of the country’s policies toward maternal health. Within the realm of healthcare decisions, this research sheds insight on the significance of perceived policy support. There is a possibility that women will be more likely to opt for facility-based deliveries if they have the perception that maternal health policies are supportive. In spite of this, it is of the utmost importance to acknowledge that the way in which individuals and areas perceive policy might vary. Within the context of the possibility of giving birth at Ta TU Hospital, the perceived benefits of hospital delivery have a marginally significant impact. This indicates that those who perceive a greater number of benefits associated with hospital delivery may be more likely to select Ta TU Hospital. According to the marginally significant p-value, there may be some influence; however, it is possible that the influence is not highly statistically significant. Various factors, including the perception of maternal health services, the attitude of staff, the cost of delivery, and the availability of transportation, do not appear to have statistically significant effects on the choice of hospital delivery and should be investigated further. The reasons for this perception may vary from person to person and should be investigated further. It is possible that these findings are dependent on the context, and they do not align with the findings of studies such as the one [33], which indicated that the attitudes of health personnel and the conditions of the facility had a major impact on the delivery choices that were made. The results of this study shed light on the intricate interplay of elements that is responsible for the selection of Ta TU Hospital as the location for the delivery of the baby. Others, such as problems during pregnancy and the attitude of the staff, do not demonstrate substantial influence, despite the fact that certain characteristics, such as prior pregnancy and desired place of delivery, are in line with expectations.
- CONCLUSIONS
The poll sheds light on a number of different aspects that have a role in the decisions that respondents make regarding their maternal healthcare when they are receiving antenatal treatment at Ta TU Hospital. There are a number of factors that influence a woman’s preference to give birth in a hospital setting, including her age, level of education, and previous pregnancy experience. There are a number of factors that are related with a higher possibility of selecting Ta TU Hospital for delivery. These factors include the availability of medical specialists, the desire to avoid difficulties, and the need to reduce waiting time and prescription expenditures. Furthermore, the study highlighted concerns linked to staff confidence, cost, and facility resources as reasons for choosing alternate birth places. Additionally, the study outlines problems that arise when attempting to reach the hospital during labor. The results of this study suggest that there is a requirement for enhanced healthcare infrastructure, personnel training, and cost-related support in order to promote facility-based healthcare delivery.
- RECOMMENDATIONS
Based on the findings, the following recommendations are made:
- Ta TU Hospital should focus on improving its healthcare infrastructure to enhance the confidence of pregnant women in its services. This includes ensuring the availability of necessary equipment, maintaining a clean and sterile environment, and providing adequate facilities and resources.
- Training programs should be implemented to enhance the skills and attitude of healthcare staff, addressing concerns raised by respondents regarding staff confidence and personalized care.
- Strategies to reduce the cost of delivery services should be explored, such as subsidizing healthcare costs or providing financial assistance to economically disadvantaged individuals.
- Efforts should be made to improve transport accessibility to the hospital to address the challenges faced by some respondents in accessing the facility during labor.
- Continued efforts to provide information and education about the benefits of facility delivery, antenatal care, and potential risks of home delivery are crucial to raising awareness and encouraging expectant mothers to make informed choices.
- Engaging the community, especially family members, in discussions and decision-making regarding delivery location can help address concerns and promote facility-based deliveries.
REFERENCES
- Abugri, J., Med, S. E. K., Educ, K., & Akum, A. E. A. (2013). Factors Associated with Skilled Delivery: A Case of the Upper East Region of Ghana. Developing Country Studies, 3(10), 88-98.
- Adjei, G. (2015). The Maternal Mortality in Ghana. Midwifery Today with International Midwife, 1(116), 41-43.
- Ambruoso, L., Abbey, M., & Hussein, J. (2005). The Availability of Life-Saving Obstetric Services in Developing Countries: An In-Depth Look at the Signal Functions for Emergency Obstetric Care. International Journal of Gynecology & Obstetrics, 88(2), 113-120.
- Bell, J., Hussein, J., & Potts, A. (2003). The impact of regionalization of maternity care on the place of birth in England: A systematic review. Journal of Public Health, 25(1), 67-79.
- Boah, M., Dankwah, A. E., Abugri, J. O., Adjei, K., & Gudu, B. (2018). Factors Contributing to High Antenatal Care Coverage and Low Facility Delivery in the Upper East Region of Northern Ghana: A Cross-Sectional Study. BMC Pregnancy and Childbirth, 18(1), 482.
- Amrit Raj Subedi (2024). Combined Pleural Fluid Cholesterol and Total Protein in Differentiation of Exudates and Transudates in Cases Presenting in Tribhuvan University Teaching Hospital. Dinkum Journal of Medical Innovations, 3(09):630-644.
- Bulatao, R. A., & Ross, J. A. (2000). Antenatal care and skilled delivery: Effects on maternal mortality and morbidity in the developing world. WHO Safe Motherhood Technical Consultation.
- Carlough, M., & McCall, M. (2005). Skilled birth attendance: What does it mean and how can it be measured? A clinical skills assessment of maternal and child health workers in Nepal. International Journal of Gynecology & Obstetrics, 89(2), 200-208.
- Carter, S. M. (2010). Maternal Mortality and Family Patterns in Sub-Saharan Africa: New Evidence from Maternity Histories in Rural Ghana. Population Studies, 64(1), 45-65.
- Gavino S. Nuñez Ii, Chelsea Angela R. Plasencia, Blessie B. Doble, Shiena Mitchelle L. Baldoza & Maricris B. Dionson (2024). Evaluation of Self-Care Practices of Pregnant Women in Barangay Apas, Cebu City, Philippines. Dinkum Journal of Medical Innovations, 3(08):581-596.
- Carter, S. M. (2010). Maternal Mortality and Family Patterns in Sub-Saharan Africa: New Evidence from Maternity Histories in Rural Ghana. Population Studies, 64(1), 45-65.
- Cochran, W. G. (1977). Sampling techniques (3rd ed.). Wiley.
- Cotter, K., Hawken, M., Temmerman, M., & Low, N. (2006). Treatment of sexually transmitted infections for HIV prevention: End of the road or new beginning? AIDS, 20(5), 651-662
- Creswell, J. W. (2007). Qualitative inquiry and research design: Choosing among five approaches. Sage Publications.
- Justice Badam Parmaak (2024). A Review on Occupational Health & Safety Implementation Protocols of the Mining & Petroleum Industries in Ghana. Dinkum Journal of Medical Innovations, 3(08):609-618.
- Dankwah, E., Abugri, J., & Med, S. E. K. (2019). Determinants of the Utilisation of Skilled Care during Delivery in Northern Ghana: A Cross-Sectional Study. Clinical Medicine Research, 8(5-6), 90-98.
- (2018). District Health Information Management System II. Ghana Health Service. [URL]
- Esena, R. K., & Sappor, M. M. (2013). Factors Associated with the Utilization of Skilled Delivery Services in the Ga East Municipality of Ghana. International Journal of Reproductive Medicine, 2013, 456282.
- Esena, R. K., Sappor, M. M., Adjei, K., Abugri, J., & Gudu, B. (2013). Factors Associated with Low Uptake of Skilled Delivery Services among Women in Rural Northern Ghana: A Cross-Sectional Study. BMC Pregnancy and Childbirth, 13, 131.
- Gabrysch, S., Civitelli, G., Edmond, K. M., Mathai, M., Ali, M., & Bhutta, Z. A. (2011). New Signal Functions to Measure the Ability of Health Facilities to Provide Routine and Emergency Newborn Care. PLoS Medicine, 8(4), e1001079.
- Gage, A. J. (2007). Barriers to the utilization of maternal health care in rural Mali. Social Science & Medicine, 65(8), 1666-1682.
- Charissa Rosamond D. Calacday (2024). Patient Safety Culture in Selected Government Hospitals in the National Capital Region (NCR) Towards Improved Healthcare Practices. Dinkum Journal of Medical Innovations, 3(05):349-357.
- Graham, W. J., Bell, J. S., & Bullough, C. H. (2001). Can skilled attendance at delivery reduce maternal mortality in developing countries? Studies in Health Services Organization & Policy, 17, 97-130.
- Gudu, W., & Addo, B. O. (2017). A Two-Year Review of Maternal Mortality at the Korle Bu Teaching Hospital, Accra, Ghana. Journal of Asian and African Studies, 52(4), 421-434.
- Kamwendo, F., & Bullough, C. (2005). What causes maternal mortality? A qualitative study of maternal deaths in Malawi. In Beyond the Numbers: Reviewing Maternal Deaths and Complications to Make Pregnancy Safer (pp. 85-96). WHO
- Koblinsky, M., Matthews, Z., Hussein, J., Mavalankar, D., Mridha, M. K., Anwar, I., … & Bhandari, N. (2006). Going to scale with professional skilled care. The Lancet, 368(9544), 1377-1386.
- Rukmani Kafle (2024). Medication Adherence to Psychotropic Drugs among Patient Attending OPD of Teaching Hospital Chitwan Medical College Teaching Hospital, Nepal. Dinkum Journal of Medical Innovations, 3(04):321-336.
- Samson, A. (2012). Violence against Women: Maternal Health in Afghanistan. The Lancet, 379(9811), e55.
- Rakesh Kumar Mahato, Sagar Pokharel & Avinash Sahani (2024). Knowledge & Practice Regarding Neonatal Resuscitation among Health Care Providers in Tertiary Care Hospitals of Nepal. Dinkum Journal of Medical Innovations, 3(03):257-270.
- Thaddeus, S., & Maine, D. (1994). Too far to walk: Maternal mortality in context. Social Science & Medicine, 38(8), 1091-1110.
- (2008). The Millennium Development Goals Report 2008. United Nations.
- Sohel Mahmud, Sharmin Ara Yasmin, Nahal Mostak Khan, Soheb Ahmed Robin & Lutfullahil Khabir (2024). Demographic Profile & Associated Risk Factors of Patients with Retinal Vein Occlusion in a Tertiary Eye Hospital. Dinkum Journal of Medical Innovations, 3(01):64-71.
- (2014). World Population Dashboard. United Nations Population Fund.
Publication History
Submitted: October 02, 2024
Accepted: October 20, 2024
Published: October 31, 2024
Identification
D-0339
DOI
https://doi.org/10.71017/djmi.3.10.d-0339
Citation
Ruhaima Issah Zorro & Amadu Baba (2024). High Antenatal Attendance, Low Facility Delivery: Assessment of Factors Influencing Facility Delivery in a University Hospital in Ghana. Dinkum Journal of Medical Innovations, 3(10):733-749.
Copyright
© 2024 The Author(s).