

")
Publication History
Submitted: October 02, 2024
Accepted: October 20, 2024
Published: August 30, 2025
Identification
D-0484
DOI
https://doi.org/10.71017/djmi.4.8.d-0484
Citation
Prajwol Thapa (2025). The Prevalence of Factors Associated with Post Stroke Depression in Stroke Survivors. Journal of Medical Innovations, 4(08):506-523.
Copyright
© 2025 The Author(s).
506-523
The Prevalence of Factors Associated with Post Stroke Depression in Stroke SurvivorsOriginal Article
Prajwol Thapa 1*
- National Academy of Medical Sciences (NAMS), Mahaboudha, Kathmandu , Bagmati , Nepal.
* Correspondence: prajwolthapa40@gmail.com
Abstract: Post stroke depression is one of the important but under emphasized affective illness following stroke. The etiology of depression is complex because it actually consists of a multifaceted group of depressive disorders however Post stroke depression (PSD) is highly determined by specific factors including various sociodemographic factors, perceived social support for stroke survivors and amount of functional independence. A cross-sectional descriptive study was conducted in Bir hospital, neuro medicine department. Patients scoring more than 18 in mini mental state examination (MMSE) were included. Patients were initially screened with the help of Patient Health Questionnaire (PHQ – 9) and diagnosis of depression was made by International Classification of Diseases Diagnostic Criteria for Research (ICD-10 DCR) followed by assessment of severity of depression by Hamilton Depression Rating Scale (HAM- D). Functional independence of the cases along with their perceived social support was also evaluated. Out of total of N=62 patients recruited, 38.7 % (n=24) were males and 61.3% (n=38) were females. 38.7% (n= 24) were from the age group of 55 – 64 years. Majority were illiterate and were from the low socioeconomic status. Out of the total cases 43.5 % (n=27) had post stroke depression. Post stroke depression was most common after 5 years of stroke. Post stroke survivors with mild to moderate functional dependency had 43.5% of depression. Stroke survivors with highest perceived social support had depression of about 3.2% (n= 2). Presence of new onset depression in a significant number of patients following stroke highlights the importance of evaluating stroke survivors for depression which could negatively impact upon patient’s functional and social life. Presence of decreased PSD in stroke survivors with high perceived social support signify the importance of psychosocial intervention to prevent the emergence of new onset depression.
Keywords: prevalence, factors, post stroke depression, stroke survivors
- INTRODUCTION
The World Health Organization defines stroke as a condition characterized by rapidly developing clinical signs of focal or global neurological deficit, lasting more than 24 hours or leading to death, with no apparent cause other than of a vascular origin [1]. As per a worldwide estimate of WHO, every year about 15 million individuals suffer from stroke out of which around 33% (5 million) die and 33% become disabled permanently [2]. Stroke causes 9% of all deaths globally and is the second most common cause of death. In addition, stroke is the most important cause of physical disability of people over 60 years of age [3,4]. Although stroke is a world-wide problem, the burden of stroke is particularly serious in Asia along with higher mortality rates [5]. Rate of strokes in these countries has exceeded the rate of developed countries by 20% during the period from 2000 to 2008. Although the study of the epidemiology of stroke in developed Western countries (as judged from the number of relevant articles published in international medical journals) is extensive, in Asian countries it has been comparatively limited (with the exception of Japan) [6]. The two main types of strokes are ischemic and hemorrhagic, accounting for approximately 85% and 15% of the cases respectively. Ischemic strokes or cerebral infarcts (CI) are the result of development of thrombi and/or emboli leading to blockages and lead to deficiency of oxygen in vital tissues. Hemorrhagic strokes occur from rupture of cerebral vessels, often as the result of high blood pressure exerting excessive pressure on arterial walls already damaged by atherosclerosis, aneurysm, or arteriovenous malformation [6].Those who suffer ischemic strokes have much better chance of survival than those who experience hemorrhagic stroke, as hemorrhagic stroke not only damages brain but also may lead to increased pressure on the brain or spasms in the blood vessels [7].The majority of patients have symptoms and signs of unilateral motor and/or sensory disturbances associated with ipsilateral facial paresis, visual field defects, and dysphasia or aphasia if the dominant hemisphere was involved [8].About one-third of stroke survivors experience depression, anxiety or apathy, which are the most common neuropsychiatric sequelae of stroke [9].Anxiety disorders following stroke include generalized anxiety disorder, panic attacks, and post-traumatic stress disorder. Some 22% to 28% of stroke patients are affected by generalized anxiety disorder. The rate of panic disorder is not known. Post-traumatic stress reactions appear in between 10% and 30% of patients. Up to 60% of those with stroke can develop a fear of falling and this has been associated with poorer physical function and a history of falls [10]. While considering hospital-based referral for stroke, out of a total of 286 patients admitted to Neurology ward of Bir Hospital in one year period, 210 patients were diagnosed as having a stroke. Among these 124 (59.05%) were males and 86 (40.95%) were females. 19 (9.05%) were below 45 years of age, 122 (58.10%) were in the age range of 45 to 65 years age and 69(32.86%) were aged more than 65 years. Hemorrhagic strokes were 89 (42.95%) and Ischemic were 121 (57.62%). Males were more affected than females (59% vs. 41%) [11]. Depression refers to a range of mental problems characterized by loss of interest and enjoyment in ordinary experiences, low mood and associated emotional, cognitive, physical and behavioral symptoms. Depression is one of the most prevalent diseases. Globally, 6% of the population meets the major depressive disorder (MDD) criteria at any specific time point [12]. Depression fell from 22.5 to 14.0 per 1000 Person Years at Risk (PYAR). The incidence of depressive symptoms rose threefold from 5.1% to 15.5 % per 1000 PYAR [13]. Post-stroke depression is among the most common emotional disorders affecting stroke sufferers [14]. Post stroke depression (PSD) has been recognized by psychiatrists for more than 100 years, but controlled systematic studies did not begin until the 1970s [15]. The etiology of depression is complex because it actually consists of a multifaceted group of depressive disorders. Due to the multifactorial nature of major depression, there is no one simple definitive and universal cause for the disorder. Major depression has been attributed to a number of causative factors including biochemical, genetic, anatomical and psychosocial factors [16]. This amine hypothesis could be conceived as the supplement or further explanation of lesion location hypothesis when it is used to explain the pathogenesis of PSD or vascular depression. According to this hypothesis, cerebral lesions interrupt the projections ascending from midbrain and brainstem, passing through thalamus and basal ganglion, and reaching the frontal cortex and then result in the decrease or decreased bioavailability of biogenic amines, including serotonin (5-HT), dopamine (DA), and norepinephrine (NE), thus resulting in depressive symptoms [17]. It has been proposed that major depressive disorder (MDD) results from the interaction of predisposing genes and the environment. Nowadays, this relationship emerges as the gene polymorphism hypothesis of PSD. Based on the theory of biogenic amines, the serotonergic system appears as a canor genetic susceptibility to PSD. Few studies have investigated the role of serotonin genes polymorphisms in PSD. For instance, an author reported that the Serotonin Transporter Gene-Linked Promoter Region (5-HTTLPR) allele was associated with PSD in a sample of 26 stroke patients with major depression and 25 non-depressed stroke patients in the first genetic study of PSD [18]. It was suggested that left anterior cerebral lesions were associated with significantly higher depression scores than left posterior lesions. Diagnosable depressive disorders were found in approximately 70% of stroke patients with left frontal brain injuries. It is estimated that only 15% of the variance in depression could be explained by the severity of intellectual impairment, physical impairment, quality of social support, or age, whereas the site of the lesion explained 50% of the variance [19]. In addition, proinflammatory cytokines, such as interkeukin-18, tumor necrosis factor-α (TNF-α) also lead to depression [20]. Also, substantiative evidence was found regarding the role of oxidative stress in pathogenesis of depression. Reactive oxygen species generated during stroke caused oxidative stress, lipid peroxidation, protein oxidation and DNA damage in neural tissue [21]. Functional support refers to the provision of supportive functions by other persons. These functions may include emotional support; tangible, or practical, support; informational support, such as guidance or advice; and social companionship, for example, in leisure or recreational activities. A further distinction may be made between received versus perceived functional support. While received support (observed acts of support) may vary according to life circumstances, perceived support, or the subjective experience of feeling oneself to be supported, is understood to remain relatively stable. Due to disability after stroke, survivors take part in fewer social activities, family life is disrupted, and contact with friends and the wider network is vulnerable. Social isolation is a commonly reported sequel, and may disproportionately affect those with aphasia which plays an important role in precipitating post stroke depression [20]. So, stroke survivors with decreased functional independence have the higher prevalence of post stroke depression compared to stroke survivors having high functional independence. Psychiatric sequelae of stroke are often overlooked in our scenario, even when the stroke survivors are constantly at a risk. Post stroke depression is the major psychiatric event that can affect those who have had a stroke and it has significant impact not only on the quality of life of the survivors but it adversely affects the recovery process as well. Hence, present study has aimed to determine the incidence of post stroke depression and factors associated with it. This study measured the prevalence and factors associated with post stroke depression in stroke survivors attending the neurology/neuro medicine outpatient’s department at Bir hospital.
- MATERIALS & METHOD
The study was carried out after the thesis protocol was accepted by the ethical committee of NAMS (National Academy of Medical Sciences) & IRB (Institutional Review Board). This is a Cross-sectional hospital based observational study carried out at Bir Hospital for a period of 6 months. Non-Probability Convenience Sampling method was used and Sample size was 62
Z= 1.96 at 95% confidence level
P= 20% (prevalence of post stroke depression) International Journal of Stroke
q= 100 – p = 80%
d= 10% (maximum tolerable error)
N= z2pq / d2
= (1.96)2 (20) (80) / 102
= 62
The study was carried after approval of thesis proposal by IRB (Institutional Review Board), NAMS (National Academy of Medical Sciences). Patients diagnosed by consultant neurologist as stroke with MMSE (Mini Mental State Examination) score above 18 were included. Informed written consent was taken from patient and patient party before inclusion in the study. PHQ-9 (Patient Health Questionnaire) was applied as a screening tool to find depressive symptoms among sample scoring greater than 4 in PHQ. Then diagnosis of depression was made as per the ICD – 10 criteria. Severity of depression was assessed by HAM- D (Hamilton Depression Rating Scale) among those diagnosed as having a depressive episode as per ICD – 10. Barthel Index along with perceived social support for stroke survivor scale were also applied for assessing function independence in activities of daily living. This includes a semi-structured questionnaire developed specifically to record the socio-demographic data and presenting complaints of the patients concerned. Tenth Revision of International Classification of Diseases – Diagnostic Criteria for Research by the Division of Mental Health of the World Health Organization (WHO, 1992). It deals with the mental and behavioral disorders and the version is mainly used for research purposes. It gives operational criteria for the diagnosis of mental disorders. The criteria are clearly defined and are specified in more detail. MMSE test is a 30-point questionnaire that is extensively used in clinical and research settings to measure cognitive impairment. It is commonly used in medical and allied health to screen for dementia. It is also used to estimate severity and progression of cognitive impairment [21]. It is a multipurpose instrument for screening of the depression. It incorporates DSM-IV depressive diagnostic criteria with other major depressive symptoms into a brief self-report tool [22]. The Barthel scale or Barthel ADL index is a tool used to measure the personal care and movement of the patient in activities of daily living (ADL). Each performance item is rated on this scale with a given number of points assigned to each level or ranking [23]. It is mainly classified as mild, moderate and severe dependent. It is one of the tools to indicate severity of depression and as a guide to evaluate recovery by probing mood, feelings of guilt, suicide ideation, insomnia, agitation or retardation, anxiety, weight loss, and somatic symptoms [24]. MPSSS is a well validated and psychometrically rigorous 12 item concise instrument used for measurement of perceived social support from family, friends [25]. Data was collected on a semi-structured proforma covering the relevant aspects of the study using above mentioned scales and ICD-10 diagnostic criteria. Data was evaluated and diagnosis of the participant was retrieved. Analysis of data was performed after acquiring variables from the studied cases. Data was entered into computer using SPSS 20. Statistical Analysis was done by using chi square test. A 95% confidence interval was taken & P value less than 0.05 was termed as statistically significant. Results were presented in tables, graphs & diagrams. Result obtained was discussed with reference to the current world literature then inclusion was drawn based on the results. Approval of the study was obtained from the Institutional Review Board (IRB) of NAMS. Participant / guardian were explained about the disease, the study, the procedure and its significance, consequences, the expected benefit to them & to the community. A written informed consent indicating that the participant or guardian (if the patient is a minor) has understood all the information in the consent form and is willing to participate in the research was obtained from all guardians of patients included in this study. They were assured of full confidentiality during & after the study period. Participants could withdraw from study at any time without giving any reason.
- RESULTS & DISCUSSION
Out of 62 patients, there were 38.7% males (n= 24) and 61.3% females (n= 38). Mean age of presentation was 57.35 and 57.15 for males and females respectively. Majority 38.7% (n=24) were from the age group 55-64 years. Majority of the sample population was illiterate 71% (n=44). Regarding marital status 91.9% were married and rest were widowed. Among the studied cases 33.9% (n=21) were from the lower middle class followed by 32.3% (n= 20) were from the upper lower class. Among the cases 77.4% (n=48) were Hindus.
Table 01: Socio demographic profile of patients
| Age (yrs) | Sex | Total | ||||
| Male | female |
No |
% |
|||
| No | % | No | % | |||
| 25-34 | 0 | 0 | 1 | 1.6 | 1 | 1.6 |
| 35-44 | 3 | 4.8 | 6 | 9.7 | 9 | 14.5 |
| 45-54 | 6 | 9.7 | 5 | 8.1 | 11 | 17.7 |
| 55-64 | 9 | 14.5 | 15 | 24.2 | 24 | 38.7 |
| >65 | 6 | 25 | 11 | 17.7 | 17 | 27.4 |
| Total | 24 | 38.7 | 38 | 61.3 | 62 | 100 |
| Mean | 57.35 | 57.15 | 58.04 | |||
Table 02: characteristics and categories of patients
| Characteristics | Categories | Cases | |||||
| Male | Female | Total | |||||
| Number | % | Number | % | Number | % | ||
| Education | Illiterate | 18 | 29 | 26 | 41.9 | 44 | 71 |
| Primary | 2 | 3.2 | 7 | 11.3 | 9 | 14.5 | |
| Secondary | 3 | 4.8 | 4 | 6.5 | 7 | 11.3 | |
| Graduate | 1 | 1.6 | 1 | 1.6 | 2 | 3.4 | |
| Marital Status | Married | 22 | 35.5 | 35 | 56.5 | 57 | 91.9 |
| Widowed | 2 | 3.2 | 3 | 4.8 | 5 | 8.1 | |
| Occupation | Business | 2 | 3.2 | 1 | 1.6 | 3 | 4.8 |
| Farming | 9 | 14.5 | 22 | 35.5 | 31 | 50.0 | |
| Labour | 3 | 4.8 | 3 | 4.8 | 6 | 9.7 | |
| Service | 5 | 8.1 | 5 | 8.1 | 10 | 16.1 | |
| Housewife | 5 | 8.1 | 7 | 11.3 | 12 | 19.4 | |
| Types Of Family | Nuclear | 9 | 14.5 | 11 | 17.7 | 20 | 32.3 |
| Joint | 15 | 24.2 | 20 | 32.3 | 35 | 56.5 | |
| Extended | 0 | 0 | 7 | 11.3 | 7 | 11.3 | |
| Socioeconomic Status | Lower | 0 | 0 | 3 | 4.8 | 3 | 4.8 |
| Upper Lower | 8 | 12.9 | 12 | 19.4 | 20 | 32.3 | |
| Lower Middle | 8 | 12.9 | 13 | 21.0 | 21 | 33.9 | |
| Upper Middle | 7 | 11.3 | 8 | 9.7 | 13 | 21.0 | |
| Upper | 1 | 1.6 | 4 | 6.5 | 5 | 8.1 | |
| Religion | Hindu | 18 | 29.0 | 30 | 48.4 | 48 | 77.4 |
| Buddhist | 6 | 9.7 | 4 | 6.5 | 10 | 16.1 | |
| Christian | 0 | 0 | 2 | 3.2 | 2 | 3.2 | |
| Others | 0 | 0 | 2 | 3.2 | 2 | 3.2 | |
| 24 | 39.7 | 38 | 61.3 | 62 | 100 | ||
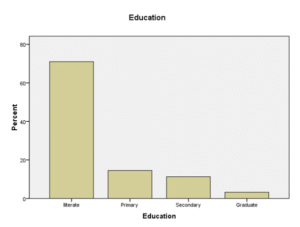
Figure 01: Educational status of studied case
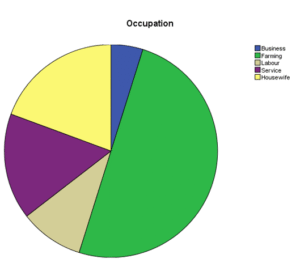
Figure 02: Occupational status of studied case
Out of total of 62 stroke patients who were evaluated, 43.5 % (n= 27) had the evidence of a depressive episode with post stroke onset. Depressive episode with the post stroke onset was seen among 19.4% (n= 12) of male and 24.2% (n= 15) of females.
Table 03: New onset depression (post stroke)
| ICD (Depressive episode) |
Total |
|||
| Depression | No Depression | |||
| Male | Frequency | 12 | 12 | 24 |
| % of total | 19.4% | 19.4% | 38.7% | |
| Female | Frequency | 15 | 23 | 38 |
| % of total | 24.2% | 37.1% | 61.3% | |
| Total | Frequency | 27 | 35 | 62 |
| Total | 43.5% | 56.5% | 100% | |
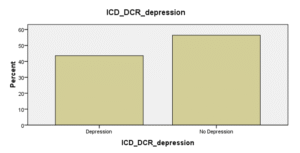
Figure 03: Post stroke depression
Among the 62 studied case, 27 had post stroke depression. Among them, the majority were females (55.6 %), were Hindus (81.5%) and were form the upper lower socioeconomic status (44.4 %). Most of them were from the joint family (37 %) and had agriculture as their main profession (63%).
Table 04: Sex of the respondents
| Frequency | Percent | |
| Male | 12 | 44.4 |
| Female | 15 | 55.6 |
| Total | 27 | 100 |
Table 05: Religion of the respondents
| Frequency | Percent | |
| Hindu | 22 | 81.5 |
| Buddhist | 4 | 14.8 |
| Christian | 1 | 3.7 |
| Total | 27 | 100 |
Table 06: Socioeconomic Status of the respondents
| Frequency | Percent | |
| Lower | 3 | 11.1 |
| Upper Lower | 12 | 44.4 |
| Lower Middle | 6 | 22.2 |
| Upper Middle | 5 | 18.5 |
| Upper | 1 | 3.7 |
| Total | 27 | 100 |
Table 07: Types Of Family
| Frequency | Percent | |
| Nuclear | 10 | 37 |
| Joint | 17 | 63 |
| Total | 27 | 100 |
Table 08: Occupation of the respondents
| Frequency | Percent | |
| Business | 3 | 11.1 |
| Farming | 14 | 51.9 |
| Labour | 5 | 18.5 |
| Service | 2 | 7.4 |
| Housewife | 3 | 11.1 |
| Total | 27 | 100 |
Table 09: Education of the respondents
| Frequency | Percent | |
| Illiterate | 21 | 77.8 |
| Primary | 2 | 7.4 |
| Secondary | 3 | 11.1 |
| Graduate | 1 | 3.7 |
| Total | 27 | 100 |
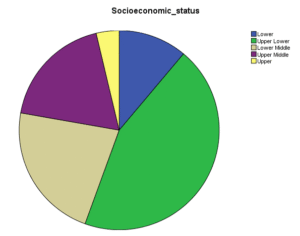
Figure 04: Socioeconomic Status of Studied case
Among the total sample comprising of 62 cases of stroke; 43.5 % (27 cases) had new onset depression whereas 56.5% (35 cases) didn’t have any evidence of depression. Out of 27 depressed patients 74.1 % (n= 20) had ischemic stroke and rest 25.9 % (n = 7) had hemorrhagic stroke. 40.8% among those with ischemic stroke had new onset depression whereas 53.9 % among those with hemorrhagic stroke had post stroke depression. Similarly, among those who had developed new onset depression, 37% had right sided stroke whereas 63 % had left sided stroke. Among those with a left sided stroke; 56.7% had an episode of new onset depression whereas this was 31.2% among those having a right sided lesion. Those with a left sided ischemic stroke had the highest overall incidence of new onset depression followed by those having a right sided ischemic stroke. The incidence of depression was lesser in those with hemorrhagic stroke.
Table 10: Types Of Strokes and Post Stroke Depression
| Depressive Episode (ICD – DCR) | Total | ||||
| Depression | No Depression | ||||
| Types Of Strokes | Ischaemic | Frequency | 20 | 29 | 49 |
| % within types of Strokes | 40.8% | 59.2% | 100% | ||
| % of total | 32.3% | 46.8% | 79% | ||
| Haemorrhagic | Frequency | 7 | 6 | 13 | |
| % within types of Strokes | 53.9% | 46.2% | 100% | ||
| % of total | 11.3% | 9.7% | 21% | ||
| Total | Frequency | 27 | 35 | 62 | |
| % within Stroke | 43.5% | 56.5% | 100% | ||
| % of total | 43.5% | 56.5% | 100% | ||
Table 11: Stroke localization and post stroke depression
| Depression (ICD – DCR) | Total | Chi Square Test | ||||||
| Depression | No Depression | Value | df | P value | ||||
| Location Of Stroke | Right | Frequency | 10 | 22 | 32 | 4.069 | 1 | 0.044 |
| % within types of Strokes | 31.2% | 68.8% | ||||||
| % of total | 16.1% | 35.5% | 51.6% | |||||
| Left | Frequency | 17 | 13 | 30 | ||||
| % within types of Strokes | 56.7% | 43.3% | ||||||
| % of total | 27.4% | 21.0% | 48.4% | |||||
| Total | Frequency | 27 | 35 | 62 | ||||
| % within Stroke | 43.5% | 56.5% | 100% | |||||
| % of total | 43.5% | 56.5% | 100% | |||||
Table 12: Stroke localization and types with post stroke depression
|
Depression
No Depression |
Stroke |
Total |
||||
| Right Ischaemic | Left Ischaemic | Right Haemorrhagic | Left Haemorrhagic | |||
| frequency | 8 | 12 | 3 | 4 | 27 | |
| % of total | 12.9% | 19.4% | 4.8% | 6.5% | 43.5% | |
| frequency | 18 | 11 | 4 | 2 | 35 | |
| % of total | 29.0% | 17.7% | 6.5% | 3.2% | 56.5% | |
| Total | Frequency | 26 | 23 | 7 | 6 | 62 |
| % of total | 41.9% | 37.1% | 11.3% | 9.7% | 100.0% | |
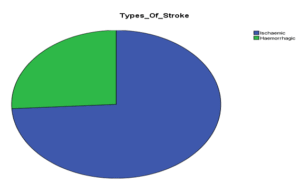
Figure 05: Stroke types and depression
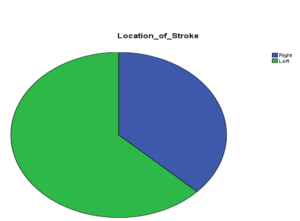
Figure 06: Localization of Stroke and Depression
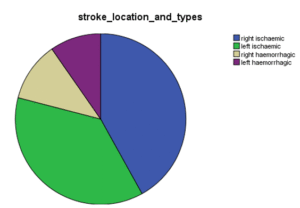
Figure 07: Stroke types and localization with depression
Among those cases in whom new onset depression was diagnosed, 70.4% (n =19) had mild depression, 22.2% (n=6) had moderate depression, whereas 7.4 % (n=2) had severe and very severe depression combined. Age group from 55 to 64 years had highest percentage of depression. Females had the highest percentage of post stroke depression mainly of mild intensity. Cases with PSD were mostly illiterate farmers. Among those with ischemic stroke (74.1%), 48.1% had mild depression whereas on among those with left sided stroke 44.4% had highest number of cases with mild depression followed by moderate and severe depression.
Table 13: Age group and severity
| Age Group | HAM D Rating Scale | ||||||||
| Mild Depression | Moderate Depression | Severe – Very severe Depression | Total | Value | df | P
value |
|||
| 35-44 | frequency | 4 | 0 | 0 | 4 | 5.05 | 6 | .536 | |
| % of total | 14.8% | 0% | 0% | 14.8% | |||||
| 45-54 | frequency | 2 | 1 | 0 | 3 | ||||
| % of total | 7.4% | 3.7% | 0% | 11.1% | |||||
| 55-64 | frequency | 6 | 3 | 2 | 11 | ||||
| % of total | 22.2% | 11.1% | 7.4% | 40.7% | |||||
| >64 years | frequency | 7 | 2 | 0 | 9 | ||||
| % of total | 25.9% | 7.4% | 0% | 33.3%% | |||||
| Total | frequency | 19 | 6 | 2 | 27 | ||||
| % of total | 70.4% | 22.2% | 7.4% | 100% | |||||
Table 14: Sex and severity of the respondents
| Sex | HAM D Rating Scale | ||||||||
| Mild Depression | Moderate Depression | Severe – very Severe Depression | Total | Value | df | P
Value |
|||
| male
|
frequency | 7 | 4 | 1 | 12 | 1.67 | 2 | .434 | |
| % of total | 25.9% | 14.8% | 3.7% | 44.4% | |||||
| Female | frequency | 12 | 2 | 1 | 15 | ||||
| % of total | 44.4% | 7.4% | 0% | 55.6% | |||||
| Total | frequency | 19 | 5 | 2 | 27 | ||||
| % of total | 70.4% | 22.2% | 7.4% | 100% | |||||
Table 15: Education and Severity
| Education | HAM D Rating Scale | ||||||||
| Mild Depression | Moderate Depression | Severe – Very Severe Depression | Total | Value | df | P
Value |
|||
| Illiterate | frequency | 14 | 5 | 2 | 21 | 2.83 | 6 | .829 | |
| % of total | 51.9% | 18.5% | 7.4% | 77.8% | |||||
| Primary | Frequency | 1 | 1 | 0 | 2 | ||||
| % of total | 3.7% | 3.7% | 0% | 7.4% | |||||
| Secondary | frequency | 3 | 0 | 0 | 3 | ||||
| % of total | 11.1% | 0% | 0% | 11.1% | |||||
| Graduate | frequency | 1 | 0 | 0 | 1 | ||||
| % of total | 3.7% | 0% | 0% | 3.7% | |||||
| Total | frequency | 19 | 6 | 2 | 27 | ||||
| % of total | 70.4% | 22.2 % | 7.4% | 100% | |||||
Table 16: Occupation and Severity
| Occupation | HAM D Rating Scale | ||||||||
| Mild Depression | Moderate Depression | Severe – Very Severe Depression | Total | Value | df | P
Value |
|||
| Business | frequency | 2 | 1 | 0 | 3 | 4.60 | 8 | .799 | |
| % of total | 7.4% | 3.7% | 0% | 11.1% | |||||
| Farming | frequency | 11 | 2 | 1 | 14 | ||||
| % of total | 40.7% | 7.4% | 3.7% | 51.9% | |||||
| Labour | frequency | 2 | 2 | 1 | 5 | ||||
| % of total | 7.4% | 7.4% | 3.7% | 18.5% | |||||
| Service | frequency | 2 | 0 | 0 | 2 | ||||
| % of total | 7.4% | 0% | 0% | 7.4% | |||||
| housewife | Frequency | 2 | 1 | 0 | 3 | ||||
| % of total | 7.4% | 3.7% | 2% | 11.1% | |||||
| Total | frequency | 19 | 6 | 7.4% | 100% | ||||
Table 17: Types Of Family and Severity
| Family | HAM D Rating Scale |
Total |
||||||||
| Mild Depression | Moderate Depression | Severe- Very Severe Depression | Total | Value | df | P
value |
||||
| Nuclear
|
frequency | 7 | 2 | 1 | 10 | 10 | 1.80 | 2 | .914 | |
| % of total | 25.9% | 7.4% | 3.7% | 37.0% | 37.0% | |||||
| Joint | frequency | 12 | 4 | 1 | 11 | 11 | ||||
| % of total | 44.4% | 14.8% | 3.7% | 63.0% | 63.0% | |||||
| Total | frequency | 19 | 5 | 2 | 27 | 27 | ||||
| % of total | 70.4% | 22.2% | 7.4% | 100% | 100% | |||||
Table 18: Depression Severity and Location of Lesion
| HAM D Rating Scale |
Total |
||||||||
| Mild | Moderate | Severe- Very Severe | Value | df | P value | ||||
| Types of Strokes | Ischaemic | Frequency | 13 | 6 | 1 | 20 | 3.020 | 2 | .221 |
| % of total | 48.1% | 22.2% | 3.7% | 74.1% | |||||
| Haemorrhagic | Frequency | 6 | 0 | 1 | 7 | ||||
| % of total | 22.2% | 0% | 3.7% | 25.9% | |||||
| Total | Frequency | 19 | 6 | 2 | 27 | ||||
| % of total | 70.4% | 22.2% | 7.4% | 100% | |||||
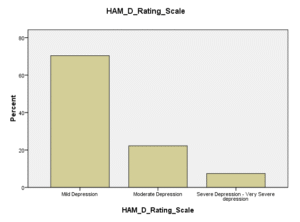
Figure 08: Types of Severity
In the studied cases, highest number of cases with post stroke depression was found in those with the stroke duration of greater than 5 years followed by those in whom stroke duration was up to 6 months i.e. 14.5% (n=9) and 12.9% (n= 8) respectively.
Table 19: Duration after stroke period after stroke and Depression
| ICD DCR |
Total |
||||
| No depression | Depression | ||||
| Duration after stroke | Up to 6months | Frequency | 9
14.5% |
8
12.9% |
17
27.4% |
| % of Total | |||||
| 6 months to 1 year | Frequency | 7
11.3% |
4
6.5% |
11
17.7% |
|
| % of Total | |||||
| 1 year to 5 years | Frequency | 11
17.7% |
6
9.7% |
17
27.4% |
|
| % of Total | |||||
| Greater than 5 years | Frequency | 8
12.9% |
9
14.5% |
17
27.4% |
|
| % of Total | |||||
| Total | Frequency | 35 | 27 | 62 | |
| % of Total | 56.5% | 43.5% | 100% | ||
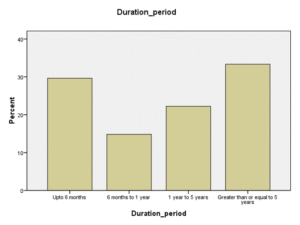
Figure 09: Duration after stroke
On assessing the functional independence in carrying out the activities of daily living among those with PSD; 41.5% had mild level of dependence followed by 55.5% with moderate dependence. Rate of PSD was lower among those with mild dependence in comparison to those with moderate dependence.
Table 20: Functional independence and depression
| Functional independence | Functional independence | Total | ||||||
| Mild Dependent | Moderate Dependent | Value | df | P Value | ||||
| Depression | Frequency | 22 | 5 | 27 | .617 | 1 | .432 | |
| % within Functional Independence | 41.5% | 55.6% | 43.5% | |||||
| No Depression | Frequency | 31 | 4 | 35 | ||||
| % within Functional Independence | 58.5 % | 44.4% | 56.5% | |||||
| Total | Frequency | 53 | 9 | 62 | ||||
| % of total | 100% | 100% | 100% | |||||
Among the studied cases only 3.2% of total (n= 2) had depression with high perceived social support whereas no depression was present in 35.5% (n= 22) of it. 24.2% of total depression had low perceived social support.
Table 21: Perceived social support for the Stroke survivors and Depression
| Perceived Social Support for the stroke survivors | Depression (ICD) | Total | ||||||
| Depression | No Depression | Value | df | P value | ||||
| High Perceived Support | Frequency | 2 | 22 | 24 | 26.057 | 2 | 0.00 | |
| % of total | 3.2% | 35.5% | 38.7%% | |||||
| Moderate Perceived Support | Frequency | 10 | 11 | 21 | ||||
| % of total | 16.1% | 17.7% | 33.9% | |||||
| Low Perceived Support | Frequency | 15 | 2 | 17 | ||||
| % of total | 24.2% | 3.2% | 27.4% | |||||
| Total | Frequency | 27 | 35 | 62 | ||||
| % of total | 43.5% | 56.5% | 100% | |||||
Among study sample, 43.5% had depression. Among those who had depression; the number of females with depression were more than males with post stroke depression. This might be due to hormonal fluctuation at perimenopausal period, strong genetic predisposition to depression or commonness of depression itself in females. The prevalence of post stroke depression was found to be higher than western or even developed Asian countries. This might be due to low economic status, decreased family support and less awareness of the illness [26,27]. Female had higher post stroke depression as per similar studies found in most of the study [28]. Among the case with PSD, 81.5% Hindus followed by Buddhists and Christians. This may be due to high Hindu population prevailing in our country. Unlike females in other Asian countries, higher rates of depression in females in this studied sample may be due to the fact that depressive episode is more common in females in the general population itself. There was higher prevalence of post stroke depression in farmers which is 51.9%. The finding was similar to similar study done in India and China. This may be due to increased financial burden, decreased family awareness regarding the disease in these population group and majority of the population engaged in agriculture as their primary profession. In this study 77.8% of those having post stroke depression were illiterates which may be due to the fact that majority of the sample population were aged more than 55 years and there was less opportunity to study during the youthful era of this age group or increased attendance of illiterate people from low socioeconomic status attending this hospital more frequently. On similar study done in Finland and several other Asian countries, those with left sided stroke i.e. 63% had significantly greater rates of post stroke depression than right sided stroke which might be due to increased prevalence of depression when left frontal lobe is involved. Similarly Ischemic lesion (74.1%) had higher amount of post stroke depression unlike hemorrhagic stroke (25.9%) which is same like other similar types of the studies. Overall left ischemic lesion (19.4 %) had the maximum number of post stroke depression followed by right ischemic (12.9 %) lesion. This might be due to proposed mechanism regarding decrease in nor epinephrine, serotonin and dopamine levels. In this study, age group from 55 years to 64 years especially had highest percentage of post stroke depression compared to other age groups. This may be due to decrement in the functionality, lack of support from the family, other chronic comorbid conditions. In this study, rates of severe depression and very severe depression were 3.7% each followed by 70.4% and 22.2% cases of mild and moderate depression respectively. Other similar studies have shown increased rates of mild depression especially in the elderly compared to others. This might be due to lesions not involving important anatomical structures contributing to increased severity of the post stroke depression and also may be due to the increased family support received after the illness [29]. In this study highest number of cases of PSD was present after 5 years of post-stroke followed by first 6 months of stroke which might be due to persistent disability, functional dependence, low economic productivity and chronicity of symptoms. In the other studies done in Europe and Asia, post stroke depression was highly prevalent in early 3 years compared to higher number of depressions after 5 years which might be due to abrupt stress, difficulty in adjusting in terms with their work [30,31]. In this study patients with high perceived social support had significantly lowest of the depression which is 3.2% followed by moderate (16.1%) and low perceived support (24.2%) of total. This could be due to sense of perceived solace from the family and friends which is similar as compared to other study [30]. In this study moderately dependent post stroke patients had highest percentage of depression (55.6 %) followed by mildly dependent (41.5 %). Like similar study done on other Asian countries, they too had high prevalence of depression in mild and moderate dependent patients. This might be due to disability and also from the decrement in the functionality [32].
- CONCLUSIONS
The study was performed to identify the relationship between stroke and depression, assess clinicodemographic factors associated with post stroke depression, evaluate relationship between stroke localization and post stroke depression and analyze the differences in the clinicodemographic factors associated with severity of post stroke depression, Study included 62 cases fulfilling the inclusion criteria. Information was obtained from patients and application of various scales were done with respect to post stroke depression. Number of females participants were higher than the males. Majority of patients were with low level of education, low socioeconomic status, married and were farmers. Post stroke depression was found to be greater than one third of total participant in the study with majority of the participants having depression with lesion located on left ischemic side. Several Sociodemographic factors were significantly associated with post stroke depression. Social support from the family members and friends too were shown to have influence on the participants regarding their progress to post stroke depression and functional independence too showed to have impact on post stroke depression.
REFERENCES
- Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 1980;58(1):113-30.
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, et al. Heart Disease and Stroke Statistics—2009 Update. Circulation [Internet]. Ovid Technologies (Wolters Kluwer Health); 2009 Jan 27;119(3):480–6
- Berg A, Depression and its assessment among stroke patients and their caregivers. 2010 Jan 29.
- Kanyal N. The science of ischemic stroke: pathophysiology & pharmacological treatment. Int J Pharm Res Rev. 2015;4(10):65-84.
- Kim JS. Stroke in Asia; A Global Disaster. Internet Journal of Stroke SAGE Publications; 2014 Sep 18;9 (7);856-7.
- Viriyavejakul A. Stroke in Asia: an epidemiological consideration. Clinical neuropharmacology. 1990 Jan 1;13:S26-33.
- Perna R, Temple J. Rehabilitation outcomes: ischaemic versus haemorrhagic strokes. Behavioural neurology. 2015 Jul 12; 2015.
- Kaste M, Waltimo O. Prognosis of patients with middle cerebral artery occlusion. Stroke [Internet]. Ovid Technologies (Wolters Kluwer Health); 1976 Sep 1;7(5):482–5
- Ferro JM, Caeiro L, Figueira ML. Neuropsychiatric sequelae of stroke. Nature Reviews Neurology [Internet]. Springer Nature; 2016 Apr 11;12(5):269–80
- Kneebone I, B. Lincoln N. Psychological Problems after Stroke and Their Management: State of Knowledge. Neuroscience and Medicine [Internet]. Scientific Research Publishing, Inc,; 2012;03(01):83–9
- Shrestha A, Shah DB, Adhikari SK, Sapkota S, Regmi PR. Retrospective Analysis of Stroke and Its Risk Factors at Bir Hospital. Post- Graduate Medical Journal of NAMS. 2011 Dec 31; 11(02 )
- Penninx BW, Milaneschi Y, Lamers F, Vogelzangs N. Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Medicine [Internet]. Springer Nature; 2013 May 15;11(1)
- Rait G, Walters K, Griffin M, Buszewicz M, Petersen I, Nazareth I. Recent trends in the incidence of recorded depression in primary care. British Journal of Psychiatry. Royal College of Psychiatrists; 2009 Dec;195(06):520–4.
- Gaete JM, Bogousslavsky J. Post-stroke depression. Expert Review of Neurotherapeutics Internet. Informa UK Limited; 2008 Jan;8(1):75–92
- Gavino S. Nuñez Ii, Chelsea Angela R. Plasencia, Blessie B. Doble, Shiena Mitchelle L. Baldoza & Maricris B. Dionson (2024). Evaluation of Self-Care Practices of Pregnant Women in Barangay Apas, Cebu City, Philippines. Dinkum Journal of Medical Innovations, 3(08):581-596.
- Robinson RG, Jorge RE. Post-stroke depression: a review. American Journal of Psychiatry. 2015 Dec 18;173(3):221-31.
- Abdu’l-Missagh Ghadirian MD. Depression: Biological, Psychosocial, and Spiritual Dimensions and Treatment; 2015.
- Feng C, Fang M, Liu XY. The neurobiological pathogenesis of poststroke depression. The Scientific World Journal. 2014 Mar 4;2014.
- Pedroso VS, Souza LC, Brunoni AR, Teixeira AL. Post stroke depression: clinics, etiopathogenesis and therapeutics. Archives of Clinical Psychiatry (São Paulo). 2015 Feb;42(1):18-24.
- Carson AJ, MacHale S, Allen K, Lawrie SM, Dennis M, House A, Sharpe M. Depression after stroke and lesion location: a systematic review. The Lancet. 2000 Jul 8;356(9224):122-6.
- Northcott, S., Moss, B., Harrison, K., & Hilari, K. . A systematic review of the impact of stroke on social support and social networks: associated factors and patterns of change. Clinical Rehabilitation, Aug 2016; 30(8), 811–831.
- Srivastava A, Taly AB, Gupta A, Murali T. Post-stroke depression: prevalence and relationship with disability in chronic stroke survivors. Annals of Indian Academy of Neurology. 2010 Apr;13(2):123.
- Santos EB, Rodrigues RA, Pontes-Neto OM. Prevalence and predictors of post stroke depression among elderly stroke survivors. Arquivos de neuro-psiquiatria. 2016 Aug;74(8):621-5.
- Sulaiman AH, Zainal NZ, Tan KS, Tan CT. Prevalence and associations of post-stroke depression. Neurol J Southeast Asia. 2002;7:71-5.
- Barker-Collo SL. Depression and anxiety 3 months post stroke: prevalence and correlates. Archives of Clinical Neuropsychology. 2007 May 31;22(4):519-31.
- Rajashekaran P, Pai K, Thunga R, Unnikrishnan B. Post-stroke depression and lesion location: A hospital based cross-sectional study. Indian journal of psychiatry. 2013 Oct;55(4):343.
- BUSH BA. Major life events as risk factors for post-stroke depression. Brain Injury . Informa UK Limited; 1999 Jan;13(2):131–7
- Leentjens AFG, Aben I, Lodder J, Verhey FRJ. General and disease-specific risk factors for depression after ischemic stroke: a two-step Cox regression analysis. International Psychogeriatrics . Cambridge University Press (CUP); 2006 Jun 29;18(04):739
- Metoki N, Sugawara N, Hagii J, Saito S, Shiroto H, Tomita T, et al. Relationship between the lesion location of acute ischemic stroke and early depressive symptoms in Japanese patients. Annals of General Psychiatry . Springer Nature; 2016 Apr 1;15(1)
- Fuller‐Thomson E, Tulipano MJ, Song M. The association between depression, suicidal ideation, and stroke in a population‐based sample. International Journal of Stroke. 2012 Apr;7(3):188-94.
- ROBINSON RG, KUBOS KL, STARR LB, RAO K, PRICE TR. MOOD DISORDERS IN STROKE PATIENTS: IMPORTANCE OF LOCATION OF LESION. Brain . Oxford University Press (OUP); 1984;107(1):81–93.
- Poynter B, Shuman Hon M, Diaz-Granados N, Kapral M, Grace SL, Stewart DE. Sex Differences in the Prevalence of Post-Stroke Depression: A Systematic Review. Psychosomatics . Elsevier BV; 2009 Nov;50(6):563–9.
- Wang Z, Zhu M, Su Z, Guan B. Post stroke depression: different characteristics based on follow up stage and gender- a cohort perspective study from Mainland China, Neurological Research; 2017 Nov;39(11):996-1005.
Publication History
Submitted: October 02, 2024
Accepted: October 20, 2024
Published: August 30, 2025
Identification
D-0484
DOI
https://doi.org/10.71017/djmi.4.8.d-0484
Citation
Prajwol Thapa (2025). The Prevalence of Factors Associated with Post Stroke Depression in Stroke Survivors. Journal of Medical Innovations, 4(08):506-523.
Copyright
© 2025 The Author(s).