

")
Publication History
Submitted: August 15, 2025
Accepted: September 22, 2025
Published: September 30, 2025
Identification
D-0497
DOI
https://doi.org/10.71017/djmi.4.9.d-0497
Citation
Bishow Kumar Shrestha, Harish Chandra Neupane & Shital Adhikari (2025). Developing and Implementing Guidelines of Prone Position Ventilation in ARDS Patients. Journal of Medical Innovations, 4(09):638-653.
Copyright
© 2025 The Author(s).
638-653
Developing and Implementing Guidelines of Prone Position Ventilation in ARDS PatientsOriginal Article
Bishow Kumar Shrestha 1*, Harish Chandra Neupane 2, Shital Adhikari 3
- Department of Pulmonology, Critical Care and Sleep Medicine, Chitwan Medical College Teaching Hospital, Chitwan, Nepal.
- Department of Surgery, Chitwan Medical College Teaching Hospital, Chitwan, Nepal.
- Department of Pulmonology, Critical Care and Sleep Medicine, Chitwan Medical College Teaching Hospital, Chitwan, Nepal.
* Correspondence: bishow.ccm@gmail.com
Abstract: Acute respiratory distress syndrome (ARDS) is recognized as common clinical problem in intensive care unit and is associated with high mortality. Mechanical ventilation is cornerstone in the treatment of ARDS, besides treatment of the underlying cause. This was an implementation study to develop guidelines and structured training program for prone positioning and to implement prone positioning in eligible ARDS patients as per guidelines in medical ICU of Chitwan Medical College and Teaching Hospital. The single best response for all the ICU staffs along multiple-choice questions was developed based on clinical guidelines and training program, which was used for pretest and posttest assessments. A total of eight training sessions were conducted; each training session consisted of eight participants. The training session was preceded by pretest and followed by posttest. A total of 64 ICU staffs including staff nurse, senior staff nurse, post-graduate medical resident, and pulmonary and critical care fellow received the training, and participated in pretest and posttest. A total of 11 ARDS patients met criteria for prone position ventilation during the enrollment period. The causes of ARDS in this cohort of patients were aspiration pneumonia (9.1%), H1N1 pneumonia (36.4%) and lobar pneumonia (54.5%). All the patients (100%) responded to prone positioning; seven (63.6%) patients were fast responders and four (36.4%) patients delayed responders. Guidelines development and structured training program to ICU staffs provides smooth and safe execution of prone positioning. Structured training program with pretest and posttest assures satisfactory competency of trainees in execution of prone maneuver. Prone positioning performed early and for prolonged duration progressively improved oxygenation, carbon di-oxide clearance and driving pressures an all critically ill ARDS patients without significant major complications. Prone positioning is safe and beneficial if performed by properly trained ICU staffs.
Keywords: developing, implementing, guidelines, prone position, ventilation, ARDS patients
- INTRODUCTION
Acute respiratory distress syndrome (ARDS) is an acute bilateral inflammatory lung injury, associated with increased pulmonary vascular permeability, increased lung weight, and loss of aerated lung tissue [1,2]. The underlying pathological processes of this clinical syndrome include direct (pulmonary) injury to the lung parenchyma or indirect (extrapulmonary) systemic insults transmitted by circulation. These insults result in the development of diffuse alveolar damage through neutrophil activation and endothelial injury leading to non-cardiogenic pulmonary edema and atelectasis leading to rapid onset of hypoxemic respiratory failure [3]. The commonest causes of pulmonary ARDS are infective and aspiration pneumonia whereas systemic sepsis is the predominant extrapulmonary cause [4]. American and European Consensus Conference (AECC) in 1994 defined criteria for acute lung injury (ALI) and ARDS [5]. Due to limitations AECC criteria for diagnostic reliability and severity stratification of patients with ARDS/ALI, the European Society of Intensive Care Medicine (ESICM) proposed the Berlin ARDS definition in 2011. The Berlin definition defined ARDS by timing (within 1 week of clinical insult or onset of respiratory symptoms); radiographic changes (bilateral opacities not fully explained by effusions, consolidation, or atelectasis); origin of edema (not fully explained by cardiac failure or fluid overload); and severity based on the PaO2/FiO2 ratio on 5 cm of continuous positive airway pressure (CPAP), with three categories of severity as mild (PaO2/FiO2 200-300), moderate (PaO2/FiO2 100-200), and severe (PaO2/FiO2 ≤100). The Berlin ARDS definition is more specific in defining the criteria; the timing of onset of clinical insult, chest imaging abnormalities, origin of edema and oxygenation, and classified the severity of disease on the basis of the degree of hypoxemia and positive end-expiratory pressure (PEEP) or continuous positive airway pressure (CPAP) [1]. ARDS is recognized as a common clinical problem in Intensive Care Unit (ICU) across the globe. Incidence of ARDS ranges from 10 to 86 cases per 100,000, with the highest rates reported in Australia and the United States [6]. In a study conducted in 459 ICUs in 50 countries by [7], 10.4% of 29,144 patients admitted to ICU and 23% of all mechanically ventilated patients met criteria for ARDS. ARDS is associated with high mortality. In a study [8], overall ICU and hospital mortality was observed to be as high as 42.7% and 47.8% respectively. Mortality due to ARDS increases with disease severity. An author [7] reported that mortality was 34.9% for those with mild, 40.3% for those with moderate, and 46.1% for those with severe ARDS. Besides treatment of underlying cause, treatment of ARDS mainly focuses on limiting further lung injury that can result from mechanical ventilation [9]. During mechanical ventilation, multiple professional societies recommend minimizing ventilator induced lung injury (VILI) through a combination of lung-protective ventilation (tidal volume of 4 to 6 ml/Kg PBW, plateau pressure ≤ 30 cmH2O with respiratory rate adjusted up to 35/minute to maintain minute ventilation), conservative fluid therapy to prevent lung edema formation and promote lung edema re-sorption in order to maintain adequate oxygenation throughout [10]. Several mechanical ventilator and pharmacologic treatment strategies have been studied in the treatment of ARDS, such as high-frequency oscillatory ventilation (HFOV), high positive end-expiratory pressure, airway pressure release ventilation, nitric oxide, neuromuscular blockers, steroids, recruitment maneuvers, extracorporeal membrane oxygenation (ECMO) and prone positioning [11]. Despite all the efforts, the mortality from ARDS remained unacceptably high. Traditionally invasive mechanical ventilation is delivered in supine position. However, randomized, controlled trials confirmed that oxygenation was significantly better and ventilator-induced lung injury reduced when patients were in the prone position than when they were in the supine position [12-14]. These physiological benefits did not translate into survival benefit in several trials until a multicenter, prospective, randomized, controlled study by Guerin et al (PROSEVA study) demonstrated early application of prolonged sessions of prone-position combined with low tidal volume mechanical ventilation significantly decreased 28-day and 90-day mortality in severe ARDS patients [15]. The use of prone positioning is sporadic in critical care medicine practice in Nepal. Even if it is used, it is usually started late and as a final rescue maneuver when the mechanical ventilation at it’s best failed to maintain satisfactory oxygenation. The probable reason for this being the belief that placing patients in the prone position and maintaining this position for long hours, can be difficult and associated with multiple complications. Studies have found that mechanical ventilation in prone position to be nearly as safe as ventilation in supine position, if performed by trained hands [15]. In fact, if started early; prone positioning could be a cheaper method to treat severe ARDS patients. It is likely that prone positioning be increasingly used, if its advantages are disseminated to ICU staffs and training programs for the same are conducted. Unavailability of guidelines and scarce training on prone positioning could be the reasons for high threshold to perform the maneuver in select ARDS patients. In this study, prior to implementation of prone positioning, draft guidelines for the same were developed through rigorous literature search. Thus, prepared guidelines went through several sessions of presentations and critical appraisals in critical care unit meetings. After development of guidelines, a structured training program which included pretest-posttest assessments, lecture and hands-on session on prone positioning was constructed based upon the guidelines and interaction with critical care experts in Chitwan Medical College Teaching Hospital and abroad (University of Tennessee, Memphis, TN, USA). Prior to implementation of prone positioning in real world, a total of eight training sessions and pretest-posttest assessments were conducted. A total of 64 ICU health professionals including pulmonary and critical care medicine fellows, postgraduate medical residents and nurses participated in the training and pretest-posttest assessments. The goal of the training was to provide knowledge regarding timely recognition of patients who would benefit from prone positioning, and to impart among the trainees the necessary skill required for manual prone maneuver and care of the prone positioned patient. Patient enrollment started only after patient safety had been ensured through training of all the ICU staffs. Prone positioning of the eligible ARDS patients was implemented manually in medical ICU using standard ICU beds. At the end of the study, both the results of pretest and posttest assessments and outcome of prone positioning in terms of improvement in oxygenation, driving pressure and carbon di-oxide clearance, and complications associated with unique posture of the prone position were evaluated.
- MATERIALS & METHOD
This study was conducted in medical intensive unit of Chitwan Medical College Teaching Hospital. This was an Implementation study done for a period of one year. The sources of data were primary through proforma. Medical intensive care unit of Chitwan Medical College Teaching Hospital, Bharatpur, Nepal. Using non-random consecutive sampling technique, a total of eleven ARDS patients receiving invasive mechanical ventilation meeting the inclusion criteria but without contraindication to prone positioning were included during the study period. All clinical, investigational including arterial blood gas and mechanical ventilator parameters during prone and supine sessions were recorded in the proforma on a daily basis. The ethical and technical clearance was taken from Institutional Review Board (IRB) – Chitwan Medical College. Data statistical analysis was performed using Statistical Package for Social Sciences version 20 (SPSS ver. 20). Standard descriptive statistics was used for data analysis. Categorical data were expressed as absolute numbers and percentages. The numerical data were expressed as mean ± standard deviation (SD) or median (minimum – maximum) depending upon the data distribution as analyzed by Shapiro Wilk test. Fisher’s exact test was used for determining association between categorical variables. Kruskal Wallis H-test was used to compare the median values of different parameters at various time periods. Paired sample t-test was used for comparison of pre-session and post-session test scores.
- RESULTS & DISCUSSION
Clinical guidelines for prone positioning ARDS patients developed through rigorous literature search and presentations, discussions and critical appraisal. The final guidelines were approved and endorsed by the critical care unit of Chitwan Medical College and Teaching Hospital. Before implementation of prone positioning in medical ICU, a structured training program was developed based on guidelines, which consisted of lecture session, audio-visual session and hands-on session on prone maneuver for all the participants. The training session was preceded by pretest and followed by posttest assessments, which consisted of carefully prepared fifty single best response multiple choice questionnaire. A total of 64 ICU staffs including 38 (59.4%) staff nurses, 11 (17.2%) senior staff nurses, 5 (7.8%) post graduate internal medicine residents (MD residents), 2 (3.1%) FCPS residents and 8 (12.5%) pulmonary and critical care medicine (PCCM) fellows received training on prone positioning, which is shown in Table 01.
Table 01: Description of participants
| Participants | Percentage |
| Staff nurse | 38 (59.4 %) |
| Senior staff nurse | 11 (17.2 %) |
| MD residents | 5 (7.8 %) |
| FCPS residents | 2 (3.1 %) |
| PCCM fellows | 8 (12.5 %) |
The mean pretest score was significantly lower in staff nurse (15.87±3.06), and was highest in PCCM fellows (25±1.31). The lowest pretest score was 9 (18%) and the highest pretest score of 27 (54%). The posttest scores significantly improved in all the groups, with the highest improvement observed in PCCM fellows. The lowest posttest score was 26 (51%), which was observed in staff nurse. The highest posttest score of 47 (94%) was observed in PCCM fellow. The mean posttest score in staff nurse (14.05 ± 3.22) was lower compared to other groups. The mean posttest score improvement was highest in PCCM fellows (19.00 ± 1.41). The details of mean pretest and posttest scores, and improvement in test score observed in posttest are given in table 02 and figure 01.
Table 02: Details of pretest and posttest scores
| Participant group | Pretest score | Posttest score | P-value* | Improvement
in test score |
| Staff nurse (n = 38) | 15.87 ± 3.06 | 29.92 ± 2.95 |
< 0.001 |
14.05 ± 3.22 |
| Senior staff nurse (n = 11) | 20.91 ± 2.12 | 33.00 ± 1.41 | 12.09 ± 2.16 | |
| MD residents (n = 5) | 21.20 ± 0.83 | 38.80 ± 0.84 | 17.60 ± 1.14 | |
| FCPS residents (n = 2) | 20.50 ± 0.71 | 39.00 ± 1.41 | 18.50 ± 0.71 | |
| PCCM fellows (n = 8) | 25.00 ± 1.31 | 44.00 ± 2.14 | 19.00 ± 1.41 |
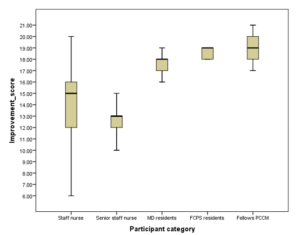
Figure 01: Distribution of test score improvement in posttest
Twenty-one (32.8 %) of the participants had posttest scores below 30 (i.e., <60 %). And all of these were staff nurse. Patient enrollment started only after all the ICU staffs, including nurses and doctors received the training on prone positioning and participated in pretest and posttest assessments. A total of 11 ARDS patients meeting criteria for prone position ventilation as per the clinical guidelines were included in the study during the study period. Six (54.5%) patients completed the prone sessions, among which 2 (33.3%) survived and the remaining 4 (66.7%) expired during treatment. Five (45.5%) patients dropped out from the study while their prone sessions were in progress citing different reasons including social issues. However, the dropped-out patients completed at least 3 prone sessions before leaving the study. Thus, they were included in the analysis of changes brought by prone positioning in oxygenation, driving pressures, carbon di-oxide clearance and complications observed. The mean age of patients who underwent prone positioning was 38.63 ± 17.76 years. All the patients in the study were female. The youngest patient was 19 years and the oldest was 56 years of age. The mean predicted body weight of the patients was 52.82 Kg; the lowest being 48 Kg and the highest 59 Kg. Similarly, the mean body mass index (BMI) was 23.82 ± 1.71 kg/m2, the lowest being 21.3 kg/m2 and the highest 26.1 kg/m2. Among total of 11 patients, 1 (9.1%) patient was current smoker and 3 patients (27.3%) were alcohol consumers. Seven (63.6%) patients did not have any comorbidity while 2 (18.2%) patients were hypertensive, 1 (9.1%) patient diabetic and 1 (9.1%) patient had connective tissue disease related interstitial lung disease. The mean left ventricular ejection fraction (LVEF) by transthoracic echocardiography on admission was 59.09 ± 2.02 %; 55% being the lowest and 60% was the highest. Among all the patients, 1 (9.1%) had chest tube, 5 (45.5%) had arterial line and 11 (100%) had central venous line inserted. The cause of ARDS in this cohort of patients was aspiration pneumonia in 1 (9.1%), H1N1 pneumonia in 4 (36.4%) and lobar pneumonia in 6 (54.5%). The mean sequential organ failure assessment (SOFA) score calculated at admission was 11 (8 – 15). The lowest SOFA score at admission was 8 and the highest was 15. None of the patients required renal replacement therapy (hemodialysis). The baseline characteristics of all the participants are depicted in table 03 below.
Table 03: The baseline characteristics of the participants
| Characteristic | N (%) |
| Age (years) | 38.63 ± 17.76 |
| Sex
Male Female |
0 (0.0 %) 11 (100.0 %) |
| Co-existing conditions
None HTN DM CTD-ILD |
7 (63.6 %) 2 (18.2 %) 1 (9.1 %) 1 (9.1 %) |
| PBW (kg) | 52.82 |
| BMI (kg/m2) | 23.82 ± 1.71 |
| Smoker | 1 (9.1%) |
| Alcohol Consumer | 3 (27.3%) |
| LVEF (%) | 59.09 ± 2.02 |
| Arterial Line | 5 (45.5%0 |
| CVP Line | 11 (100%) |
| Chest Tube | 1 (9.1%) |
| Cause of ARDS
Influenza A (H1N1) pneumonia Lobar pneumonia Aspiration pneumonia |
4 (36.4 %) 6 (54.5 %) 1 (9.1 %) |
| SOFA score at admission | 11 (8 – 15) |
| Other interventions
Vasopressors NM blockers Sedating agents Glucocorticoids RRT |
100.0 % 100.0 % 100.0 % 100.0 % 0.0% |
All the patients received mechanical ventilation in volume control mode prior to prone positioning. The mean duration of mechanical ventilation prior to prone positioning was 8 hours, with median tidal volume of 6 mL/Kg PBW, PEEP of 16 cm H2O and respiratory rate of 25 per minute. Similarly, the median PaO2/FiO2 (PF) was 53 mm Hg and pH was 7.23. Table 4 shows the various pre-prone mechanical ventilator parameters and ABG values.
Table 04: Baseline pre-prone mechanical ventilator parameters and ABG values
| Parameters | Median (Min – Max) |
| MV mode and its median duration(h) | 100 % VC mode, 8h |
| RR (per min) | 25 (22 – 28) |
| TV (ml/kg) | 6 (5.5 – 7) |
| PEEP (cm H2O) | 16 (12 – 18) |
| Plat (cm H2O) | 35 (30 – 38) |
| DP (cm H2O) | 19 (16 – 22) |
| PF (PaO2/FiO2) ratio | 53.0 (30.0 – 103.0) |
| SpO2: FiO2 ratio | 83.0 (50.0 – 134.0) |
| ABG values
pH Bicarbonate PaCO2 PaO2 |
7.23 (7.10 – 7.56) 19 (12 – 34) 50 (27 – 91) 53 (30 – 72) |
The most common cause of ARDS in this patient population was lobar pneumonia followed by Influenza A H1N1. The cause of ARDS and outcome is shown in table 05.
Table 05: Distribution of cause of ARDS and outcome
| Cause of ARDS | |||
| Lobar Pneumonia
N (%) |
Influenza A (H1N1) Pneumonia
N (%) |
Aspiration Pneumonia
N (%) |
|
| Drop out | 3 (27.3) | 1 (9.1) | 1 (9.1) |
| Survived | 0 | 2 (18.2) | 0 |
| Expired | 3 (27.3) | 1 (9.1) | 0 |
| Total | 6 (54.5%) | 4 (36.4%) | 1 (9.1%) |
All the patients (100%) responded to prone positioning. Seven (63.6%) patients responded within 30 minutes of prone positioning, while four (36.4%) patients responded within 1 to 4 hours of prone positioning. Table 6 shows the patients with respective responder status.
Table 06: Responder status
| Early responder (within 30 min) | 7 (63.6 %) |
| Delayed responder (within 1-4 h) | 4 (36.4 %) |
Three (75%) ARDS patients due to Influenza A (H1N1) pneumonia and 3 (50%) ARDS patients due to lobar pneumonia were fast responders (PaO2/FiO2 ratio increased by at least 20% or by ≥ 20 mmHg within one hour). The detail of responder status to prone positioning according to cause of ARDS is given in table 07.
Table 07: Responder status to prone positioning according to cause of ARDS
| Cause of ARDS | Responder
N (%) |
Delayed Responder
N (%) |
Total
N (%) |
| Lobar Pneumonia | 3 (50) | 3 (50) | 6 (100) |
| Influenza A (H1N1) Pneumonia | 3 (75) | 1 (25) | 4 (100) |
| Aspiration Pneumonia | 1 (100) | 0 | 1 (100) |
Both SpO2:FiO2 and PF ratios significantly increased as the prone session progressed, improving oxygenation. This improvement was observed in all consecutive prone sessions. Table 8 shows the serial changes in SpO2:FiO2 and PF ratios during consecutive prone sessions.
Table 08: SpO2:FiO2 and PF Ratios [median (min – max)] of the patients at different time intervals in consecutive prone sessions
| Session number | SpO2:FiO2 ratio | PF ratio | ||||
| Pre-prone | At 1 h | At the end of prone session | Pre-prone | At 1 h | At the end of prone session | |
| Session 1
(n = 11) |
83
(50 – 134) |
113
(88 – 141) |
136
(109 – 173) |
53
(30 – 103) |
78
(56 – 108) |
104
(76 – 161) |
| Session 2
(n = 11) |
110
(88 – 116) |
131
(108 – 157) |
136
(109 – 173) |
68
(60 – 99) |
92
(74 – 110) |
117
(92 – 195) |
| Session 3
(n = 11) |
129
(106 – 151) |
147
(115 – 168) |
175
(146 – 209) |
85
(72 – 97) |
99
(85 – 126) |
130
(106 – 197) |
| Session 4
(n = 9) |
141
(103 – 225) |
156
(134 – 173) |
188
(158 – 240) |
94
(89 – 119) |
115
(96 – 144) |
148
(117 – 225) |
| Session 5
(n = 3) |
140
(128 – 200) |
145
(145 – 158) |
173
(172 – 176) |
101
(99 – 109) |
114
(103 – 130) |
142
(131 – 156) |
| Session 6
(n = 3) |
142
(133 – 143) |
157
(157 – 162) |
190
(176 – 196) |
109
(104 – 124) |
122
(112 – 153) |
144
(142 – 178) |
| Session 7
(n = 2) |
153
(140 – 190) |
173.5
(157 – 190) |
218
(194 – 242) |
114
(112 – 116) |
128.5
(123 – 134) |
172
(154 – 190) |
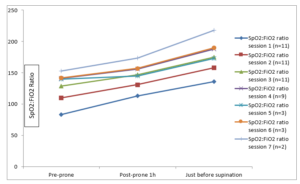
Figure 02: Serial changes in SpO2:FiO2 ratios in consecutive prone sessions
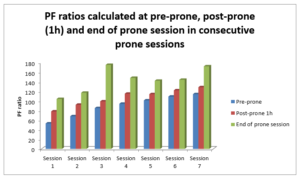
Figure 03: Serial changes in PF ratios in consecutive prone sessions
There was serial improvement in PF ratios as prone session progressed. Compared to pre-prone PF ratio, the highest PF ratio improvement was 94.2% and the lowest improvement was 47.2%, seen at the end of first and third prone sessions, respectively. Table 9 shows the mean PF ratio values (before, after 1 hour and at the end of prone positioning) over 4 consecutive prone sessions (5th session onwards not considered because of reduction in sample size due to large number of dropouts).
Table 09: Magnitude of PF ratio improvement during prone sessions
| Session number | Before prone session | At 1 hour of prone session | At the end of prone session | Median % improvement in PF ratio* |
| Session 1 (n =11) | 59.3 ± 19.4 | 79.1 ± 14.1 | 105.8 ± 21.9 | 94.2 % |
| Session 2 (n =11) | 71.5 ± 11.4 | 91.9 ± 10.6 | 121.0 ± 26.7 | 59.7 % |
| Session 3 (n =11) | 84.4 ± 7.0 | 104.3 ± 12.7 | 135.9 ± 26.4 | 47.2 % |
| Session 4 (n =9) | 98.7 ± 10.5 | 115.7 ± 16.3 | 148.0 ± 35.2 | 62.6 % |
* % improvement in a particular session was calculated by [(PF ratio at the end of the session- PF ratio before the start of session)/ PF ratio before the start of session * 100%]. The improvement in PF ratio was rapid immediately after prone positioning, thereafter the improvement was less slow but steady till the end of the session. Figure 4 shows the course of PF ratio during four consecutive prone sessions when transitioned from supine position.
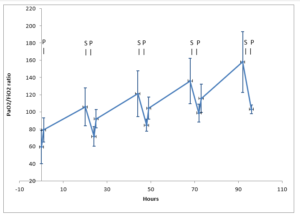
Figure 04: Course of PF ratio during four consecutive periods of prone and supine positioning; S: supine; P: prone
When the expired (n = 4) and survived group (n = 2) were compared, there was sequential and prominent fall in mean PaCO2 in the survived group after every prone session. The mean PaCO2 was either static or didn’t fall significantly in the expired group after prone session.
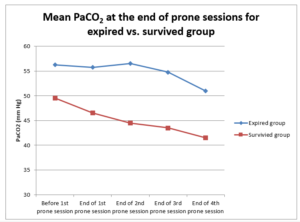
Figure 05: Relationship of mean PaCO2 between survived and expired groups
Driving pressure (P plat minus PEEP) decreased during and after every prone session compared to pre-prone state. The decrease in driving pressure (DP) was progressive during the prone session and reached the lowest value at the end of the session compared to pre-prone state. The details of changes in driving pressure are shown table 10 and figure 06.
Table 10: Driving pressures of the patients at different time intervals in consecutive prone sessions
| Session number | DP (cm H2O)
(P plat minus PEEP) |
||||
| Pre-prone | At 1h | At 4h | At 12 h | End of prone session | |
| Session 1
(n = 11) |
19 (16 – 22) | 17 (15 – 18) | 16 (13 – 17) | 16 (14 – 17) | 15 (14 – 17) |
| Session 2
(n = 11) |
18 (17 – 20) | 17 (15 – 18) | 16 (15 – 17) | 15 (14 – 17) | 14 (14 – 16) |
| Session 3
(n = 11) |
17 (16 – 21) | 16 (14 – 17) | 15 (13 – 17) | 15 (13 – 16) | 14 (12 – 16) |
| Session 4
(n = 9) |
17 (15 – 19) | 15 (13 – 18) | 15 (12 – 16) | 14 (11 – 16) | 13 (9 – 15) |
| Session 5
(n = 3) |
16 (13 – 18) | 16 (15 – 16) | 15 | 14 (13 – 14) | 13 (12 – 14) |
| Session 6
(n = 3) |
16 (16 – 17) | 16 (15 – 16) | 14 (14 – 15) | 14 | 13 (12 – 14) |
| Session 7
(n = 2) |
14 (14 – 17) | 15 (13 – 17) | 14 (12 – 16) | 13 (12 – 14) | 13 (12 – 14) |
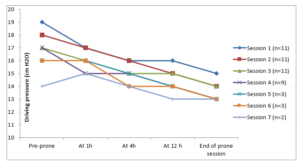
Figure 06: Changes in driving pressure in consecutive prone sessions
The average prone-session duration was 19.5 (18 – 21.5) hours and average supine session duration was 5.25 (4 – 6) hours. Out of six (54.5%) patients who stayed in the study, four (36.4%) patients met stoppage criteria and two (18.2%) patients expired while their prone sessions were on progress. All the four (36.4%) patients who met stoppage criteria were successfully liberated from mechanical ventilation. Two (18.2%) patients required post-extubation non-invasive ventilation (NIV) and one (9.1%) patient underwent tracheostomy. Two (18.2%) patients survived, while two (18.2%) patients expired during on-going prone session, and two (18.2%) expired after completion of prone session and liberation from mechanical ventilation. Table 11 shows the outcomes of the study population.
Table 11: Outcome of patients
| Patients that had unrecorded outcome (Drop-outs) | 5 (45.5 %) |
| Patients that had recorded outcome
Expired while prone ventilation was on-going Expired after stoppage of prone ventilation Improved and discharged |
6 (54.5%)
2 2* 2* |
* These patients met stoppage criteria for prone ventilation
The average duration of mechanical ventilation in those patients who completed the study was 9.5 (5 – 19) days. SOFA score at admission was highest (11.5±0.7) among survivors compared to others. There was sequential decrease in SOFA score in survivors while the SOFA score progressively increased in non-survivors and drop-outs. The changes in first three consecutive SOFA scores are shown in table 12.
Table 12: Changes in SOFA score
| Participant group | Survivors
(n = 2) |
Non-survivors
(n = 4) |
Drop outs
(n = 5) |
| SOFA 1 | 11.5 ± 0.7 | 11.0 ± 3.2 | 10.8 ± 1.8 |
| SOFA 2 | 9.5 ± 2.1 | 11.5 ± 2.5 | 12.4 ± 1.7 |
| SOFA 3 | 7.5 ± 2.1 | 12.0 ± 3.5 | 14.0 ± 2.3 |
Of the various complications observed due to prone positioning, facial swelling was the commonest observed in all patients (100%) followed by pressure sore on anterior chest in 3. (27.3%) patients, foot drop and critical illness myopathy were seen in one (9.1%) patient each. Details of all the complications observed are given in table 13.
Table 13: Complications of patients
| Swelling
Face Periorbital Lip |
11 (100.0 %) 10 (90.9 %) 4 (36.4 %) |
| Pressure sores
Anterior chest wall Cheek Anterior abdominal wall Sacrum Anterior thigh Knee Toes Heel Ear |
3 (27.3 %) 2 (18.2 %) 2 (18.2 %) 3 (27.3 %) 1 (9.1 %) 0 (0.0 %) 2 (18.2 %) 1 (9.1 %) 0 (0.0 %) |
| Foot drop | 1 (9.1 %)
[present at the time of discharge] |
| Critical illness myopathy | 1 (9.1 %) |
| VT/VF during prone session
Cardiac arrest during prone session |
0 (0.0 %)
0 (0.0 %) |
DISCUSSION
Prone positioning critically ill ARDS patients has numerous benefits. Recently a survival benefit from prone positioning has been reported [15]. This is an implementation research aimed to implement prone positioning inn medical ICU of a teaching hospital. The study began with development of guidelines of prone positioning ARDS patients. The guidelines went through several sessions of presentations, discussions and critical appraisal in critical care unit meetings, and revisions as per recommendations of the experts before being ratifies by the critical care unit of the hospital. An author [16] in a study mentioned similar method of development of clinical guidelines for prone positioning as we did in our study. Following guidelines development, a structured training program for prone positioning was developed based on the guidelines and evidence-based practice recommendations. The training program was developed in consultation with critical acre experts’ home and abroad. Though prone positioning is not an invasive procedure, it still has potential to cause complications related to its unique positioning [15,17]. All the ICU staffs were provided the training prior to implementation of prone positioning in real patients. During the training, all the participants were pre and post tested with meticulously prepared set of multiple-choice questions that consisted of fifty questions. Such assessments along with training were shown to be superior to bare training, in learning outcome of the participants [18,19]. Clinical guidelines and staff training ensure patient safety and standardize the approach to the use of this technique. A total of 64 ICU staffs including doctors and nurses participated in the training, which was conducted in eight separate sessions. Majority of the participants were nurses; 38 (59.4%) were staff nurse and 11 (17.2%) were senior staff nurse. Fifteen (23.4%) participants were doctors; 5 (7.8%) were MD internal medicine residents, 2 (3.1%) were FCPS fellow and 8 (12.5%) were PCCM fellows. The mean pretest and posttest scores were lower in staff nurse compared to other groups. The probable reason for this could be the lower educational status of staff nurse compared to other participants of this study. Staff nurses are junior health professionals. Insufficient exposure and inadequate experience of these comparatively younger staff nurses to intensive care environment and critically ill patients could have played additive role. In addition, the staff nurses are in the beginning of their career and they have yet to choose their future career. Some staff nurses might have different career goals than critical care nurse which could lower their enthusiasm to learn highly specific critical care maneuver, i.e., prone positioning, which they might not be using once they take different role as nurse in the future. There was significant improvement in posttest scores in all the groups; the highest improvement was seen in PCCM fellows. This finding is consistent with studies done by several researchers that showed improved posttest scores indicating improved knowledge following structured training program [20-23]. The PCCM fellows, on the other hand, have set career goals and they had already chosen critical care medicine as their career. In addition, the level of academic knowledge, previous experiences in dealing with ARDS and critically ill patients along with their familiarity to intensive care environment could have generated interest in them to learn this maneuver, which they will be using in the future and could add to their armamentarium to treat selected ARDS patients. Though the mean pretest score of senior staff nurse was slightly better than staff nurse, the post-training improvement in score, i.e., posttest score, was slightly better in staff nurse compared to senior staff nurse. The comparatively lower post-training improvement in score observed in senior staff nurse could have resulted from loss of interest to learn due to their additional family and house hold commitments and responsibilities they are likely to owe compared to younger staff nurses. The occupancy of mind with other responsibilities could affect learning. On the other hand, the comparatively younger staff nurses could have retained their enthusiasm to learn during the training. Out of total 11 patients who underwent prone positioning in this study for severe ARDS (PF ratio < 150 mm Hg with FiO2 ≥ 0.6 and PEEP ≥ 5 cm H2O), six (54.55%) patients continued with the treatment, while five (45.45%) patients dropped out of the study after initiation of prone session. All the dropped-out patients had completed at least three prone sessions before dropped out. The main reason for drop-out was cited as financial constraint inadequate social support. In country like Nepal where there is no provision of health insurance to citizen, financial constraint has been seen as a real big problem when patients require prolonged and sophisticated treatment. The majority of the patients in this study were of middle age group with mean age of 38.63±17.76 years. This age group is somewhat younger than prone arm patients included in PROSEVA study by [15] and Prone Supine II study by Taccone et al.83 Moreover, all the patients in this study were females. This is in contrast of other studies where both males and females were included and number of females was lesser than that of males [15,24]. The small number of samples could be the reason for all the participants being female in this study. The mean BMI of the patients in this study was 23.82±1.71 kg/m2. At the time of inclusion in the study, all the patients (100%) had septic shock and were receiving vasopressor. Only about three fourths of patients were receiving vasopressor in the study by [15] Moreover, mean SOFA score of patients at the time of inclusion in this study was 11 (8-5). This score is slightly higher than the scores in the studies by [15] and [25], indicating patients in this study were sicker at the time of inclusion. All the patients in this study received neuromuscular blockers and glucocorticoids, while 91% of patients received neuromuscular blockers and glucocorticoids in PROSEVA study by [15]. The mechanical ventilation in this study was delivered in volume-controlled mode with constant inspiratory flow. At the time of inclusion, mechanical ventilation was delivered with mean tidal volume of 6 (5.5-7) mL/Kg PBW and mean respiratory rate of 25 (22-28). This was similar to the tidal volumes and respiratory rates received by patients in the study by [15]. The patients in the study by [26] received higher tidal volumes than in our study. The mean PaO2 and PaCO2 values of patients in this study were 53 (30-72) and 50 (27-91), respectively. At the time of inclusion, patients in this study had lower PF ratio [mean PF ratio 53.0 (30.0-103.0)] and received higher PEEP [mean PEEP 16 (12-18)], and had higher plateau pressure [mean P plat 35 (30-38)] compared to the patients randomized to prone group in studies by [15] and [27]. This suggests that patients in our study were sicker at the time of inclusion. In our study, the most common cause of ARDS was lobar pneumonia followed by Influenza A (H1N1) pneumonia. All of the patients (100%) responded to prone positioning, some responded early while others were delayed responders. There were 7 (63.6%) early responders and 4 (36.4%) delayed responders. This observation is consistent with most of the randomized control trials and metanalysis that showed similar response to prone positioning [28-31]. Three (75%) patients of Influenza A (H1N1) pneumonia and one (100%) patient of aspiration pneumonia were fast responders to prone position while only three (50%) lobar pneumonia were fast responders. Studies by [32] and [33] reported early oxygenation improvement in ARDS associated with extra-pulmonary cause than that associated with pulmonary cause. In this study, the reason for the early responder status in Influenza A H1N1 could be due to its association with non-focal diffuse alveolar atelectasis with recruitable potential than in ARDS due to lobar pneumonia which is associated more with consolidated alveoli that are relatively resistant to recruitment [34,35]. The improvements in PF and SpO2:FiO2 ratios were reproducible with each consecutive prone session. The benefit in oxygenation accrued during prone session was preserved even after interruption of the prone session and returning to supine position. Similar observations were also reported by several other studies [15,36,37]. On comparing improvements in PF ratios in four sequential prone sessions, the improvement in PF ratio in this study ranged from 47.2% to 94.2%. Moreover, the improvement in PF ratio was more significant in the early period of prone session followed by slower yet study improvement. In the present study, mean partial pressure of carbon dioxide (PaCO2) decreased sequentially in survivors, while the decrease was minimal or even remained static in non-survivors. Prone positioning was reported to improve CO2 clearance through increased dorsal recruitment over ventral de-recruitment and this occurred independent of oxygenation response [38,39]. In addition, [40] also reported increased lung recruitment with decreased PaCO2 with prone positioning. Furthermore, [41] reported improved outcome with decreased PaCO2 on prone positioning. In addition, there was progressive decrease in driving pressure in all the patients during prone positioning in this study. The decrease was more during early part of the prone sessions. This finding is consistent with findings of the study by [42] that also reported decreased driving pressure with prone positioning, with mean decrease of driving pressures of 3.60 cm H2O (P=0.001) and 3.22 cm H2O (P < 0.0001) at PEEP 0 and 7 cm H2O, respectively. They attributed this decrease in driving pressure to increased chest wall elastance due to prone positioning. Several other studies reported improved respiratory system compliance with prone positioning [42,43]. The average duration of prone session in this study was 19.5 (18-21.5) hours per session. Patients in this study spent on an average of 81.25% of the time in prone position per day. This is comparable to prone position duration in the study by [35] and is as recommended by PROSEVA study by [15].
- CONCLUSIONS
In centers not practicing prone positioning in severe ARDS, development of prone guidelines and delivering structured training program to ICU staffs gives them adequate knowledge and confidence to implement the maneuver smoothly and safely. Prone positioning severe ARDS patients can be safely implemented by properly trained ICU staffs. Prone positioning thus implemented improves oxygenation, carbon dioxide clearance and driving pressure, which may ultimately translate into better patient survival. Knowledge and competency of trainee to perform prone positioning can be enhanced through structured training program with pretest and posttest. The most common position related complication observed was facial edema, followed by periorbital swelling. Four (36.4%) patients also had lip swelling. These complications subsided once the patients were turned supine. Few developed pressure sores on the anterior aspect of the body. There were no other life-threatening complications associated with prone positioning.
REFERENCES
- Ranieri, V. M., Rubenfeld, G. D., Thompson, B. T., Ferguson, N. D., Caldwell, E., Fan, E., et al. (2012). Acute respiratory distress syndrome: The Berlin definition. JAMA, 307(23), 2526–2533.
- Li Wei Zhang & Chen Yu Wang (2025). Snowman Sign in Pituitary Macroadenoma — A Contemporary Review. Journal of Medical Innovations, 4(08):557-566.
- Koulouras, V., Papathanasiou, A., & Nakos, G. (2016). Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review. World Journal of Critical Care Medicine, 5(2), 121–136.
- Agarwal, R., Aggarwal, A. N., Gupta, D., Behera, D., & Jindal, S. K. (2006). Etiology and outcomes of pulmonary and extrapulmonary acute lung injury/acute respiratory distress syndrome in a respiratory ICU in North India. Chest, 130(3), 724–729.
- Bernard, G. R., Artigas, A., Brigham, K. L., Carlet, J., Falke, K., Hudson, L., et al. (1994). The American-European Consensus Conference on ARDS: Definitions, mechanisms, relevant outcomes, and clinical trial coordination. American Journal of Respiratory and Critical Care Medicine, 149(3 Pt 1), 818–824.
- Villar, J., Blanco, J., & Kacmarek, R. M. (2016). Current incidence and outcome of the acute respiratory distress syndrome. Current Opinion in Critical Care, 22(1), 1–6.
- Kenji Sato & Ayaka Suzuki (2025). Redefining Lung Cancer Therapy — A Long-Awaited Shift in Strategy. Journal of Medical Innovations, 4(08):581-586.
- Villar, J., Blanco, J., Anon, J. M., Santos-Bouza, A., Blanch, L., Ambros, A., et al. (2011). The ALIEN study: Incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Medicine, 37(12), 1932–1941.
- Thompson, B. T., Chambers, R. C., & Liu, K. D. (2017). Acute respiratory distress syndrome. The New England Journal of Medicine, 377(6), 562–572.
- Fan, E., Del Sorbo, L., Goligher, E. C., Hodgson, C. L., Munshi, L., Walkey, A. J., et al. (2017). An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 195(9), 1253–1263.
- Phua, J., Badia, J. R., Adhikari, N. K., Friedrich, J. O., Fowler, R. A., Singh, J. M., et al. (2009). Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. American Journal of Respiratory and Critical Care Medicine, 179(3), 220–227.
- Abroug, F., Ouanes-Besbes, L., Elatrous, S., & Brochard, L. (2008). The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: A meta-analysis, areas of uncertainty, and recommendations for research. Intensive Care Medicine, 34(6), 1002–1011.
- Sud, S., Friedrich, J. O., Taccone, P., Polli, F., Adhikari, N. K., Latini, R., et al. (2010). Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Medicine, 36(4), 585–599.
- Zahirul Islam, Md. Zakir Hossain, Md. Fazle Rabby, Kuldeep Sharma, Hasan Rabbi & Md. Shakeel Ahmed (2025). Detection of Causative Agents of Acute Upper Respiratory Tract Infection by Film Array Respiratory Panel at Point of Care in a Tertiary Care Hospital . Dinkum Journal of Medical Innovations, 4(03):69-80.
- Guerin, C., Reignier, J., Richard, J. C., Beuret, P., Gacouin, A., Boulain, T., et al. (2013). Prone positioning in severe acute respiratory distress syndrome. The New England Journal of Medicine, 368(23), 2159–2168.
- Ashbaugh, D. G., Bigelow, D. B., Petty, T. L., & Levine, B. E. (1967). Acute respiratory distress in adults. The Lancet, 2(7511), 319–323.
- Riviello, E. D., Kiviri, W., Twagirumugabe, T., Mueller, A., Banner-Goodspeed, V. M., Officer, L., et al. (2016). Hospital incidence and outcomes of acute respiratory distress syndrome using the Kigali modification of the Berlin definition. American Journal of Respiratory and Critical Care Medicine, 193(1), 52–59.
- Lazzeri, C., & Peris, A. (2016). The Kigali modification of the Berlin definition: A new epidemiological tool for ARDS? Journal of Thoracic Disease, 8(6), E443–E445.
- Rubenfeld, G. D., Caldwell, E., Peabody, E., Weaver, J., Martin, D. P., Neff, M., et al. (2005). Incidence and outcomes of acute lung injury. The New England Journal of Medicine, 353(16), 1685–1693.
- Chen, W., Chen, Y. Y., Tsai, C. F., Chen, S. C., Lin, M. S., Ware, L. B., et al. (2015). Incidence and outcomes of acute respiratory distress syndrome: A nationwide registry-based study in Taiwan, 1997 to 2011. Medicine, 94(43), e1849.
- Taccone, P., Pesenti, A., Latini, R., Polli, F., Vagginelli, F., Mietto, C., et al. (2009). Prone positioning in patients with moderate and severe acute respiratory distress syndrome: A randomized controlled trial. JAMA, 302(18), 1977–1984.
- Mancebo, J., Fernandez, R., Blanch, L., Rialp, G., Gordo, F., Ferrer, M., et al. (2006). A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 173(11), 1233–1239.
- Ranieri, V. M., Rubenfeld, G. D., Thompson, B. T., Ferguson, N. D., Caldwell, E., Fan, E., et al. (2012). Acute respiratory distress syndrome: The Berlin definition. JAMA, 307(23), 2526–2533.
- Abroug, F., Ouanes-Besbes, L., Dachraoui, F., Ouanes, I., & Brochard, L. (2011). An updated study-level meta-analysis of randomized controlled trials on proning in ARDS and acute lung injury. Critical Care, 15(1), R6.
- Koulouras, V., Papathanasiou, A., & Nakos, G. (2016). Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review. World Journal of Critical Care Medicine, 5(2), 121–136.
- Agarwal, R., Aggarwal, A. N., Gupta, D., Behera, D., & Jindal, S. K. (2006). Etiology and outcomes of pulmonary and extrapulmonary acute lung injury/acute respiratory distress syndrome in a respiratory ICU in North India. Chest, 130(3), 724–729.
- Bernard, G. R., Artigas, A., Brigham, K. L., Carlet, J., Falke, K., Hudson, L., et al. (1994). The American-European Consensus Conference on ARDS: Definitions, mechanisms, relevant outcomes, and clinical trial coordination. American Journal of Respiratory and Critical Care Medicine, 149(3 Pt 1), 818–824.
- Villar, J., Blanco, J., & Kacmarek, R. M. (2016). Current incidence and outcome of the acute respiratory distress syndrome. Current Opinion in Critical Care, 22(1), 1–6.
- Bellani, G., Laffey, J. G., Pham, T., Fan, E., Brochard, L., Esteban, A., et al. (2016). Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA, 315(8), 788–800.
- Villar, J., Blanco, J., Anon, J. M., Santos-Bouza, A., Blanch, L., Ambros, A., et al. (2011). The ALIEN study: Incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Medicine, 37(12), 1932–1941.
- Thompson, B. T., Chambers, R. C., & Liu, K. D. (2017). Acute respiratory distress syndrome. The New England Journal of Medicine, 377(6), 562–572.
- Fan, E., Del Sorbo, L., Goligher, E. C., Hodgson, C. L., Munshi, L., Walkey, A. J., et al. (2017). An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 195(9), 1253–1263.
- Phua, J., Badia, J. R., Adhikari, N. K., Friedrich, J. O., Fowler, R. A., Singh, J. M., et al. (2009). Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. American Journal of Respiratory and Critical Care Medicine, 179(3), 220–227.
- Abroug, F., Ouanes-Besbes, L., Elatrous, S., & Brochard, L. (2008). The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: A meta-analysis, areas of uncertainty, and recommendations for research. Intensive Care Medicine, 34(6), 1002–1011.
- Sud, S., Friedrich, J. O., Taccone, P., Polli, F., Adhikari, N. K., Latini, R., et al. (2010). Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Medicine, 36(4), 585–599.
- Broccard, A., Shapiro, R. S., Schmitz, L. L., Adams, A. B., Nahum, A., & Marini, J. J. (2000). Prone positioning attenuates and redistributes ventilator-induced lung injury in dogs. Critical Care Medicine, 28(2), 295–303.
- Guerin, C., Reignier, J., Richard, J. C., Beuret, P., Gacouin, A., Boulain, T., et al. (2013). Prone positioning in severe acute respiratory distress syndrome. The New England Journal of Medicine, 368(23), 2159–2168.
- Ashbaugh, D. G., Bigelow, D. B., Petty, T. L., & Levine, B. E. (1967). Acute respiratory distress in adults. The Lancet, 2(7511), 319–323.
- Riviello, E. D., Kiviri, W., Twagirumugabe, T., Mueller, A., Banner-Goodspeed, V. M., Officer, L., et al. (2016). Hospital incidence and outcomes of acute respiratory distress syndrome using the Kigali modification of the Berlin definition. American Journal of Respiratory and Critical Care Medicine, 193(1), 52–59.
- Lazzeri, C., & Peris, A. (2016). The Kigali modification of the Berlin definition: A new epidemiological tool for ARDS? Journal of Thoracic Disease, 8(6), E443–E445.
- Rubenfeld, G. D., Caldwell, E., Peabody, E., Weaver, J., Martin, D. P., Neff, M., et al. (2005). Incidence and outcomes of acute lung injury. The New England Journal of Medicine, 353(16), 1685–1693.
- Chen, W., Chen, Y. Y., Tsai, C. F., Chen, S. C., Lin, M. S., Ware, L. B., et al. (2015). Incidence and outcomes of acute respiratory distress syndrome: A nationwide registry-based study in Taiwan, 1997 to 2011. Medicine, 94(43), e1849.
- Taccone, P., Pesenti, A., Latini, R., Polli, F., Vagginelli, F., Mietto, C., et al. (2009). Prone positioning in patients with moderate and severe acute respiratory distress syndrome: A randomized controlled trial. JAMA, 302(18), 1977–1984.
Publication History
Submitted: August 15, 2025
Accepted: September 22, 2025
Published: September 30, 2025
Identification
D-0497
DOI
https://doi.org/10.71017/djmi.4.9.d-0497
Citation
Bishow Kumar Shrestha, Harish Chandra Neupane & Shital Adhikari (2025). Developing and Implementing Guidelines of Prone Position Ventilation in ARDS Patients. Journal of Medical Innovations, 4(09):638-653.
Copyright
© 2025 The Author(s).