

")
Publication History
Submitted: August 03, 2023
Accepted: August 20, 2023
Published: September 01, 2023
Identification
D-0134
Citation
Sidra Liaqat & Muhammad Umar (2023). Analyzing the Durability and Efficacy of Integrating Routine Impulsive Hepatitis B and C Testing In Real-Life Situations. Dinkum Journal of Medical Innovations, 2(09):318-324.
Copyright
© 2023 DJMI. All rights reserved
318-324
Analyzing the Durability and Efficacy of Integrating Routine Impulsive Hepatitis B and C Testing In Real-Life SituationsOriginal Article
Sidra Liaqat 1*, Muhammad Umar 2
- King Edward Medical University, Mayo Hospital, Lahore, Pakistan; sidrakemu26w@gmail.com
- King Edward Medical University, Mayo Hospital, Lahore, Pakistan; muhammaduma@gmail.com
* Correspondence: sidrakemu26w@gmail.com
Abstract: Innovative testing techniques and care delivery systems are required to meet the global elimination goals for the hepatitis B virus (HBV) and the hepatitis C virus (HCV). There is minimal evidence to justify the European Centre for Disease Prevention and Control’s (ECDC) recommendation that emergency departments (EDs) in high-prevalence areas do routine blood-borne virus (BBV) testing. Our emergency room has provided free HIV testing since 2013. We modified the electronic patient record (EPR) system to include opportunistic opt-out HBV/reflexHCV tests for any routine blood test orders for ED visits older than 16 years old. A real-world service review was conducted as part of this upgrade. Initially mostly hospital-led, our approach of connecting with individuals who needed to be connected to care (new diagnoses/known but disengaged) has shifted to working with regional health and charitable organization networks. Over the course of 11 months, 40,881 patients went to the ED; 45.5% had blood testing done. In total, 75% of participants had HBV and HCV testing done. Both the seroprevalence of hepatitis B surface antigen (HBsAg) and HCV antigen (HCV-Ag) was 0.9%. 79% of the 140 HBsAg+ patients that were successfully reached required to be connected to care, and 87% of them took action. 130 HCV-Ag+ patients were able to be contacted, and 76% required linkage; 52% were engaged. Our results demonstrate the effectiveness and viability of universal ED EPR opt-out HBV/HCV testing along with complete linkage to treatment processes, enabling care provision, particularly to underprivileged at-risk groups with limited access to treatments. The findings support the ECDC’s recommendations for BBV testing and may have an impact on upcoming UK recommendations for hepatitis testing.
Keywords: Hepatitis B, hepatitis C, healthcare records, emergency department, durability, efficacy
- INTRODUCTION
According to recent Public Health England (PHE) estimates, 118,000 people in Pakistan were believed to have chronic HCV infection as of 2019 [1], which is a substantial source of sickness and mortality both internationally and in the UK. Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are also a significant cause of illness and mortality in the UK. HBV PHE data are unavailable, but according to the Polaris Observatory, 441,000 people had chronic HBV in 2016. [2] Although there are still considerable barriers, effective treatments that reduce mortality and morbidity for both viral infections are now widely accessible [3, 4]. A large number of infections go untreated, which contributes in part to this problem. In 2018, it was estimated that two-thirds of chronic HCV infections were misdiagnosed [6]. The World Health Organization (WHO) Global Health Sector Strategy on Viral Hepatitis put emphasis to the need for cutting-edge testing techniques and efficient links to care pathways in order to totally eradicate viral hepatitis as a significant public health problem by 2030 [5]. Although it acknowledges that there is little evidence to support its utility, the European Centre for Disease Prevention and Control (ECDC) advises routine blood-borne virus (BBV) testing in emergency departments (EDs) in high-prevalence areas [7]. More than 24 million individuals visited EDs in England in 2018–19. For frequently marginalized people who are at high risk of BBVs, the ED is frequently a key point of access to healthcare [9, 10]. Findings from recent multicenter studies, ED seroprevalence and pilot studies on ED viral testing with opt-out [11, 12]. The opportunity to get tested for the HIV virus is always available to adult ED visitors who are having blood work done for another medical reason [13–15]. Contrarily, this is not considered in the current Pakistani recommendations for hepatitis testing [16]. During a 1-week opt-out ED testing session in 2014, this type of testing was shown to be effective and feasible in nine EDs [17]. In this work, the model is enhanced to evaluate the concept’s applicability in the real world.
- MATERIALS AND METHODS
We assessed the growth of clinical services at King Edward Medical University, Mayo Hospital, and Lahore, Pakistan. Phases 1 and 2 of the project each lasted five and six months, respectively (October 2019 to February 2020 and December 2021 to May 2022). In contrast to traditional healthcare professional initiated testing models, the electronic patient record (EPR) system was modified to pre-select HBV and HCV tests for any blood test orders in the ED for patients 16 years of age on an opt-out basis, unless a positive viral hepatitis test result within the previous 6 months was available on the EPR system. At registration and from the clinician, patients were given bilingual explanatory leaflets. There were also posters put all over the ED. These brochures provided information on diseases, testing methods and policies, and how to treat either infection. Additionally, patients who were eligible were explicitly informed that viral hepatitis testing would be done prior to blood collection unless they disagreed (opted-out). The ED personnel was frequently trained by seasoned doctors. Researchers looked at individuals’ EPRs who had tested positive for both HBsAg and HCV-Ag. If there was proof that the patient was already receiving care and that the patient’s results were in line with accepted diagnoses, no additional action was necessary. Patients who tested positive for HCV-Ab but negative for HCV-Ag (and for whom no prior local HCV RNA status was identified) were asked to attend their general practitioner (GP) in order to rule out current infection. Patients who had an infection that had been verified and were still alive at the time of assessment qualified for contact (see below). No further action was taken for individuals who had dual infections with HIV and either HBV or HCV because there was already a connection to care pathway for patients with HIV infection. Patients whose diagnosis was verified (successfully contacted) were classified as “requiring linkage to care” if their disease had not been made clear (was unknown) at the time of contact, had been made known before but not receiving care, or had recently been confirmed. Continuous variables were described using IQR medians, or interquartile range medians. Categorical variables were described by absolute and relative frequencies. Overall and stratified seroprevalence estimates with their 95% confidence intervals were derived for the HCV-Ag and HBsAg tests. Prevalence ratios (PRs) were calculated using univariable and multivariable Poisson regression models in order to investigate factors associated with the requirement for an HCV or HBV test as well as seropositivity. For all tests, which had a two-sided 95% CI, the level of significance was set at p 0.05. All analyses were performed using StataCorp LP’s version 15 software.
- RESULTS AND DISCUSSION
235 out of 27,646 patients tested positive for HBsAg, resulting in a seroprevalence of 0.9% (95% CI 0.8-1.0; Table 1). With univariate testing, the following factors were significantly (p 0.001) associated with testing positive for HBsAg: male gender (PR 1.5, 95% CI 1.2-2.0), age between 30-49 years (PR 3.4, 95% CI 2.2-5.3), or age between 50-69 years (PR 4.0, 95% CI 2.5-6.3), ethnicity other than White British (PR >6.6), and positive HIV status (PR 6.0, 95% CI 2.9-12.8). When compared to daytime arrival, testing positive for HBsAg was more likely to occur at night (PR 0.7, 95% CI 0.6-1.0, p = 0.004). All of the aforementioned elements connected to testing positive for HBsAg remained statistically significant with multivariable analysis. Graphical representations of seropositivity by study period and age group are provided.
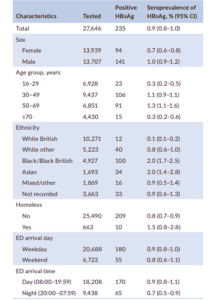
Table 1 Seroprevalence of Hepatitis B (HBsAg)
36 (15%) of the 235 patients who tested positive for HBsAg did not require any additional follow-up because local care records revealed that they were already receiving treatment at the time of testing, had a known end-of-life diagnosis (unrelated to hepatitis B), or passed away soon after testing (Figure 1). We were unable to confirm contact with 59 patients (30%) of the remaining 199 patients who were eligible for contact, however 140 patients (70%) received their hepatitis B status. The 140 patients who had successful contact had 68/140 (48%) new diagnoses, 64/140 (46%) known diagnoses, 34/64 (53%) of whom were not engaged at the time of testing, and 8/140 (6%) patients were deemed “unknown” because we were unable to learn whether they were aware of the diagnosis and/or receiving treatment at the time of contact.

Figure 1: Linkage to care in patients with positive HBsAg status
523 out of 27,657 individuals tested positive for HCV-Ab, resulting in a 1.9% (95% CI 0.7-2.0) seroprevalence of HCV-Ab. 261 patients out of the 457 HCV-Ab-positive results for which a reflex-HCV-Ag test was conducted tested positive for HCV-Ag, resulting in a seroprevalence of 0.9% (95% CI 0.8-1.0) for chronic HCV infection (Table 2).

Table 2: Seroprevalence of Hepatitis C (HCV-Ag)
The complete connection to care cascade, which includes the NHS Find and Treat program subset (discussed below), is shown in Figure 2. 3/251 (1.2%) of the 251 patients who tested positive for HCV-Ag passed away before help could reach them. Of those still alive, 130/248 (52%) were successfully reached, while 12/130 (9%) of them passed away shortly after being reached. Six patients had liver-unrelated malignancy; four had decompensated liver disease; and two had numerous comorbidities as their cause of death. 99/130 (76%) of the people who eventually reached needed linkage to care (new diagnosis or known but not engaged at time of test), while 19/130 (15%) were known and already involved. 51/99 (52%) of those who needed to be linked locally (of these, 50% had just been diagnosed), 5/99 (5%) were pointed in the direction of alternative services since they didn’t live in the area, and 41/99 (41%) declined an appointment at the time of contact. 34/51 (66%) of the patients who were connected locally attended more than one appointment, and 26/34 (76%) of them received successful treatment.
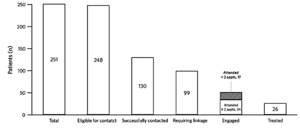
Figure 2: Linkage to care in patients with positive HCV-Ag status
According to our understanding, this 11-month service evaluation of the ED EPR opt-out HCV and HBV testing’s real-world viability is the biggest intervention of its kind in Pakistan to date. It demonstrated the viability of optout ED testing in a large metropolitan hospital setting and the ability to identify and link to care a sizable proportion of active HBV and HCV infected people from marginalized populations who have historically had limited access to healthcare. Both HBsAg and HCV-Ag seroprevalence were 0.9% in the current study. The strata-specific findings confirm those from our earlier 6-week pilot research and highlight the significant illness burden in central London [18]. The demographic traits mentioned here are consistent with those previously reported in related studies [19–21]. It is interesting that patients 50–69 years of age had a considerably greater prevalence of HCV–Ag than patients 16–49 years of age. This brings to light a possible advantage of ED opt-out testing: it can identify elderly patients who may no longer be using services for injecting drug users. Sadly, history of drug usage was not consistently recorded in patients’ notes, and as a result, formal analysis on this variable was not done. HCV-Ab and HCV-Ag seroprevalence appear to be declining over time. The system avoided repeat testing within six months of a positive result, which could be influenced by a number of factors, such as seasonal variation in attendance patterns. Therefore, we believe that any interpretation would be conjectural. It is interesting to note that the prevalence of HBsAg in the current study was over double that of the pilot; the cause of this is unknown, but it may have been accidental given the pilot’s smaller sample size. Since 141/235 of the study’s patients (60%) who tested positive for HBsAg were men, this finding may indicate that ED testing may be especially useful in identifying men who have HBV, as opposed to prenatal screening, which frequently picks up HBV infections in women [22–25]. Importantly, opt-out ED testing offers a chance to reconnect with patients who have been previously diagnosed but not connected to care, with the latter group accounting for around a quarter of HBV and half of HCV patients in our sample who need linkage to care.
- CONCLUSION
Our findings show how universal urban ED opt-out HBV and HCV testing, along with comprehensive connection to care pathways spanning secondary, primary, and community-based services, can be successful and sustainable. A sustainable high test uptake was achieved through the use of an EPR supported testing approach, and our extensive linkage network, which better connected the existing services, allowed care to be provided to traditionally underserved, at-risk groups, which would not have been possible without a significant increase in health infrastructure.
REFERENCES
- Public Health England. Hepatitis C in the UK 2020: Working to eliminate hepatitis C as a major public health threat. 2020. https:// assets.publishing.service.gov.uk/government/uploads/system/ uploads/attachment_data/file/943154/HCV_in_the_UK_2020.pdf Accessed 30 July 2021
- Razavi-Shearer D, Gamkrelidze I, Nguyen MH, et al. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. 2018;3:383-403.
- National Institute for Health and Care Excellence. Sofosbuvir– velpatasvir for treating chronic hepatitis C. Technology appraisal guidance [TA430]. 2017. https://www.nice.org.uk/guidance/ta430 Accessed 30 July 2021
- National Institute for Health and Care Excellence. Hepatitis B (chronic): diagnosis and management. Clinical guideline [CG165]. 2017. https://www.nice.org.uk/guidance/cg165 Accessed 30 July 2021
- World Health Organization. Global health sector strategy on viral hepatitis 2016–2021. 2016. https://apps.who.int/iris/handl e/10665/246177 Accessed 30 July 2021.
- Public Health England. Hepatitis C in the UK 2020. 2020. https:// assets.publishing.service.gov.uk/government/uploads/system/ uploads/attachment_data/file/943154/HCV_in_the_UK_2020.pdf Accessed 30 July 2021
- European Centre for Disease Prevention and Control. Public health guidance on HIV, hepatitis B and C testing in the EU/EEA. 2018. https://www.ecdc.europa.eu/en/publications-data/public-healt h-guidance-hiv-hepatitis-b-and-c-testing-eueea Accessed 30 July 2021
- NHS Digital. Hospital Accident & Emergency Activity 2019-20. 2020. https://digital.nhs.uk/data-and-information/publications/statistica l/hospital-accident–emergency-activity/2019-20 Accessed 30 July 2021.
- Bieler G, Paroz S, Faouzi M, et al. Social and medical vulnerability factors of emergency department frequent users in a universal health insurance system. Acad Emerg Med. 2012;19:63-68.
- Bodenmann P, Baggio S, Iglesias K, et al. Characterizing the vulnerability of frequent emergency department users by applying a conceptual framework: a controlled, cross-sectional study. Int J Equity Health. 2015;14:146.
- Hopkins MJ, Todd S, Beadsworth M, et al. Consistent high prevalence of undiagnosed blood-borne virus infection in patients attending large urban emergency departments in England. J Viral Hepat. 2020;27:88-91.
- Cieply L, Simmons R, Ijaz S, et al. Seroprevalence of HCV, HBV and HIV in two inner-city London emergency departments. Epidemiol Infect. 2019;147:e145.
- Russmann S, Dowlatshahi EA, Printzen G, Habicht S, Reichen J, Zimmermann H. Prevalence and associated factors of viral hepatitis and transferrin elevations in 5036 patients admitted to the emergency room of a Swiss university hospital: cross-sectional study. BMC Gastroenterol. 2007;7:5.
- O’Connell S, Lillis D, Cotter A, et al. Opt-out panel testing for HIV, hepatitis B and hepatitis C in an urban emergency department: a pilot study. PLoS One. 2016;11:e0150546.
- Syeda Hajra Batool, Gao Changqing & Jiang Yanyong. Aids Victims in South East Asia Endure Discrimination via Community.Dinkum Journal of Medical Innovations, 2(08):284-288.
- Alice Chen & Richa Sharma. Comparing the Maitland and Kaltenborn Mobilisation Methods to Treat Frozen Shoulder in Patients with Diabetes. Dinkum Journal of Medical Innovations, 2(08):289-295.
- Nida Zulfiqar & Irshad Hussain. A Comprehensive Review on Embolisation of Vertebral Metastasis Prior to Surgery. Dinkum Journal of Medical Innovations, 2(08):296-301.
- Marie Diack, Derak Stewart & Parshu Kirby. Prospects and Challenges of Covid-19 Vaccination Development. Dinkum Journal of Medical Innovations, 2(08):302-312.
- Sajjad Haider, Marie Diack & Derak Stewart. Association between Job Stress, Subsequent Trauma, and Secondary Trauma Self-Efficacy in Physicians Treating Covid-19 Patients. Dinkum Journal of Medical Innovations, 2(08):313-317.
- Grant C, O’Connell S, Lillis D, et al. Opt-out screening for HIV, hepatitis B and hepatitis C: observational study of screening acceptance, yield and treatment outcomes. Emerg Med J. 2020;37:102-105.
- Evans H, Balasegaram S, Douthwaite S, et al. An innovative approach to increase viral hepatitis diagnoses and linkage to care using opt-out testing and an integrated care pathway in a London emergency department. PLoS One. 2018;13:e0198520.
- Hunter L, Larbalestier N, Paparello J. Routine HIV testing in an inner city emergency department – avoiding missed opportunities for testing. In: HepHIV Conference. 2017.
- National Health Service England. Clinical commissioning policy statement: treatment of chronic hepatitis C in patients with cirrhosis. 2015. https://www.england.nhs.uk/commissioning/wp-conte nt/uploads/sites/12/2015/06/hep-c-cirrhosis-polcy-statmnt0615.pdf Accessed 30 July 2021.
- National Health Service England. University College London Hospitals: find and treat service. 2020. https://www.uclh.nhs.uk/ our-services/find-service/tropical-and-infectious-diseases/findtreat-service Accessed 30 July 2021.
- Tedder RS, Rodger AJ, Fries L, et al. The diversity and management of chronic hepatitis B virus infections in the United Kingdom: a wake-up call. Clin Infect Dis. 2013;56:951-960
Publication History
Submitted: August 03, 2023
Accepted: August 20, 2023
Published: September 01, 2023
Identification
D-0134
Citation
Sidra Liaqat & Muhammad Umar (2023). Analyzing the Durability and Efficacy of Integrating Routine Impulsive Hepatitis B and C Testing In Real-Life Situations. Dinkum Journal of Medical Innovations, 2(09):318-324.
Copyright
© 2023 DJMI. All rights reserved