

")
Publication History
Submitted: October 10, 2023
Accepted: October 24, 2023
Published: November 30, 2023
Identification
D-0154
Citation
Kamrunnahar Koli (2023). Sexually Transmitted Diseases & Infectious Diseases among Female Workers in Dhaka Export Processing Zone: A Sociological Analysis. Dinkum Journal of Social Innovations, 2(11):609-627.
Copyright
© 2023 DJSI. All rights reserved.
609-627
Sexually Transmitted Diseases & Infectious Diseases among Female Workers in Dhaka Export Processing Zone: A Sociological AnalysisOriginal Article
Kamrunnahar Koli 1* ![]()
- Department of Sociology, University of Dhaka, Bangladesh; kkoli.du15@gmail.com
* Correspondence: kkoli.du15@gmail.com
Abstract: Readymade Garment (RMG) is the leading sector in Bangladesh in terms of employment, production, and foreign exchange earnings. This sector has uplifted the neglected section of the population, i.e., women, thus radically transforming the country’s socio-economic condition through empowerment and employment generation. However, female garment workers know about menstrual hygiene. However, they need to improve their practices in order to avoid sexually transmitted diseases (STDs) and infectious diseases. This study is concerned with the status of Sexually transmitted diseases (STDs) and infectious diseases among female workers in the Dhaka Export Processing Zone (DEPZ), Bangladesh. The data has been collected with the help of secondary and primary data collection techniques from N=200 female workers. Data were analyzed, and it was found that most of the female garment workers who are infected with STDs are under the age of 25 years, and their percentage is about 66. They are not well educated; 70 % of them have a secondary level of education. It also shows that 61 % of infected females don’t have proper knowledge of STDs and infectious diseases. The female workers whom STDs and other infectious diseases infect are not willing to share their problems with others. When their health condition worsens, they go to the hospital for treatment. Those infected by the disease must go to the hospital for a routine checkup. They get free treatment and medicine from the hospital based on their economic condition. The study has provided some recommendations and suggestions to overcome the problem. In addition, some research outputs especially lead to creating an effective database of STDs and infectious diseases in the study area.
Keywords: sexually transmitted diseases, readymade garment, Bangladesh
- INTRODUCTION
Readymade Garment (RMG) is the leading sector in Bangladesh in terms of employment, production, and foreign exchange earnings. The sector contributed 9.25 per cent to GDP. Bangladesh’s overall RMG export earnings stood at USD 42613.15 million, 35.47 per cent higher than the previous fiscal year 2021. The sectoral shares of export earnings in FY22 (Bangladesh Bank, 2022). The importance of the RMG sector can hardly be overemphasized. This sector has uplifted the neglected section of the population, i.e., women, thus radically transforming the country’s socio-economic condition through empowerment and employment generation. Such empowerment and employment raised awareness regarding child education, health safety, and population control, disaster management, and so on (Sobhan & Khundker, 2001). Of the 3 million employed in the RMG sector, 2.24 million are women (BGMEA, 2018). This is mainly because the garment industry is quite susceptible to fluctuations in employment due to seasonal variations and fashion changes. These characteristics demand a highly flexible labour market, which is easily found when needed and disposed of when not wanted (Rahman et al., 2022). However, the availability of many unskilled or semi-skilled women workers for employment has been an important factor in the growth of the garment industry in Bangladesh. Most female garment workers know menstrual hygiene; however, they need to improve their practices. The rates of unwanted pregnancy and menstrual regulation (MR) are high. The poor quality of MR practice makes the situation worse. Female garment workers know little about pregnancy-related complications as well as postnatal care (Farabi et al., 2021). Their knowledge of HIV/AIDS and sexually transmitted diseases, sexually transmitted infections (STI) symptoms, and modes of transmission of STIs is poor. While usually spread by sex, some STDs can be spread by non-sexual contact with donor tissue, blood, breastfeeding, or during childbirth (Afroz et al., 2023). STD diagnostic tests are usually easily available in the developed world, but this is often not the case in the developing world. For that reason, very little is known about the conditions of garment workers because of the livelihood patterns of women workers, and awareness about them is not so high (Gourab et al., 2023). Various studies were undertaken at various times by researchers regarding garment workers’ economic, social, and health conditions. Female workers are of great importance in the socio-economic sector in Bangladesh. However, they are in the risk zone because of many known and unknown health hazards all over Bangladesh (Kayesh et al., 2023). It is significant to have sufficient knowledge about the health problems of female workers, especially STDs and infectious diseases, among the female workers in the study area to take proper action against the problem. The goal of this study is to learn about STDs and infectious diseases among female workers in the study area, as well as the causes and effects of these diseases.
- LITERATURE REVIEW
Sexually transmitted infections (STIs) are passed from person to person through intimate sexual contact. Untreated STIs may result in acute diseases, infertility, disabilities, and even death (Mahmood, 2021). They are the infections one gets from another person through sexual contact. There are more than 20 known types of STDs/STIs; sexually transmitted infections (STIs) continue to present major health, social, and economic problems in the developing world, leading to considerable morbidity, mortality, and stigma. The prevalence rates are far higher in developing countries where STI treatment is less accessible (Akter, 2022). Moreover, STIs are difficult to prevent due to difficulties accessing the groups that are particularly vulnerable to sexually transmitted diseases (STDs). These groups, so-called “unseen communities,” are particularly prevalent in South Asia, where sexual activities can be deemed distasteful and where the social stigma attached to sexual activities may be particularly strong (Huda et al., 2022). STDs may show various trends in different parts of the country and constitute a major public health problem for developing and developed countries. Their profile varies with socio-economic, cultural, geographic, and environmental changes prevalent in different parts of the country (Alam et al., 2021). The World Health Organization (WHO) has emphasized a syndromic approach for case measurement and management, particularly in high-prevalence areas with inadequate laboratory facilities, trained staff, and transport facilities (Hasnain et al., 2022). Though the syndromically diagnosed STI has many limitations, continuous analysis of risk assessment and prevalence-based screening studies are necessary to evaluate and monitor the performance of syndromic management (Islam et al., 2021). The nature of female workers’ contracts, terms and conditions, rights, and the restructuring processes of garment industries. The Bangladesh industry is located in terms of the global value chain for garments and what this location has implied for its structure, the profile of its labour force, and the terms and conditions under which it works. The implications of the industry for the broader developmental goals of economic growth, poverty reduction, and gender equality (Rahman et al., 2022). The physical status, nutrient intake, and dietary pattern of adolescent female factory workers in urban Bangladesh. Several post-menarchial girls aged 14–19 from seventeen readymade garment industries spread over Dhaka City were interviewed face-to-face on the factory premises (Farabi et al., 2021). The health and safety issues of the female workforce of garment industries in Bangladesh are based upon the industry environment, their residential environment, working conditions, age, problems of health, causes of diseases, causes of fire accidents, and their medical facilities. (Akhter et al., 2010). Discourse on the gender imbalance in the export garment industries in Bangladesh evaluated gender differences in conditions of employment and the work environment and looked at differences among the export-oriented garment industry, other export industries, and non-export industries (Majumder & Begum, 2010). A study identified morbidity patterns and durations of illness among garment workers and determined treatment-seeking behaviour during illness. The socio-demographic characteristics of the respondents were the point of investigation. Improved healthcare facilities in the garment factory may be considered for early detection and treatment of cases to avoid complications (Rahman & Rahman, 2013). The socio-economic conditions of female garment workers in Dhaka City, Bangladesh, are not so good; they work an average of 11.12 hours per day in the garment factory or industry, but they receive an average salary of less than Tk 7,000 per month. Notably, they maintain a critical life, barely managing their own and family expenses (Sikdar et al., 2014).
2.1 Social cognitive theory
The social cognitive theory places the programme application on the boundary of Sexual communication, the need for social support, and the reinforcement of behaviour change. Social cognitive theory’ helped me to continue my work systematically and progressively, and I communicate with my respondents quickly and easily (Schunk et al., 2020).
2.2 Beck’s Theory of the Risk Society of Modernity
Ulrich Beck is the contemporary theorist of modernity. He is a German sociologist who has written extensively about risk and globalization. He argues that the risk inherent in modern society would contribute to forming a global risk society. In a modern society, there is technological change. And technology produces new forms of risk, and we are constantly required to respond to and adjust to these changes. The risk society, he argues, is not limited to environmental and health risks alone; it includes a whole series of interrelated changes within contemporary social life, such as shifting employment patterns, heightened job insecurity, the declining influence of tradition and custom, the erosion of traditional family patterns, and the democratization of personal relations (Mythen, 2021).
2.3 Grid-group cultural theory
The group dimension describes how strongly people are bonded together. There are distinct and separated individuals at one end, perhaps with a common reason to be together but with less of a sense of unity and connection. Conversely, people have a connected sense of identity, relating more deeply and personally to one another. They spend more time together and have stable relationships. When people group, laws are more easily defined and enforced. Individuals must display self-restraint for society to survive when bonds are weaker and central control is less possible. In management, the low group does not manage resources, while the high group does (Maesschalck & Paesen et al., 2021).
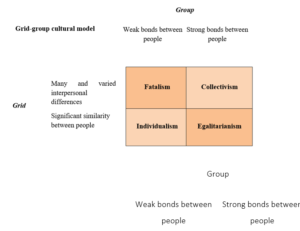
Figure 01: Grid-group cultural model
2.4 Marx’s Conflict Theory
Conflict theory states that tensions and conflicts arise when resources, status, and power are unevenly distributed between groups in society and that these conflicts become the engine for social change. In this context, power can be understood as control of material resources and accumulated wealth, control of politics and the institutions that make up society, and one’s social status relative to others (determined not just by class but by race, gender, sexuality, culture, and religion, among other things). Female garment workers are mostly deprived of material access to daily expenses. Bangladesh represents a patriarchal society where women lack education, property, social status, etc. Marriage is one of the ways of self-employment. So, because of their vulnerable marital status (migrant husband), complex strategy to get a job in a garment factory, trap of the middleman, high cost of food and housing, and low self-esteem, they have to enter into a sex zone (Moshiri, 2019).
- MATERIAL AND METHODS
3.1 Selection of the study area
This study was conducted in DEPZ, Savar, and Dhaka. It is one of the most important export processing zones in Bangladesh. It is 35 km from Dhaka city Centre. As there is a huge number of female workers in the different factories, for that reason, I chose this area for my research. DEPZ was established in 1993. The total area of the DEPZ is about 356.22 acres, and the total number of factories is above hundreds. In all the factories, about seventy thousand female workers live in the surrounding areas of DEPZ, such as Ashulia, Dendabor, Zirabo, Dhamrai, and Savar.
3.2 Study Population
The pollution of the study consists of female workers belonging to DEPZ from different age groups, regions, and religions and their marital status. Most of them are not well educated.
3.3 Data Collection & Study Instruments
In order to collect data from tangible respondents with primary data collection technique, case study and informal interview has been used. Fairly reliable sources of information on STDs and infectious diseases are available in the “Surjer Hasi Clinic.” In order to include a theoretical perspective and review the latest literature, a secondary data collection technique has been used.
3.4 Pre-testing
It is important to pre-test as it is needed to do good research, and for my research, N=40 pre-tests on the respondents to make sure that what should be included and rejected
3.5 Data Analysis
The data is analyzed and presented using different statistical techniques. The following steps (Figure 02) were followed in chronology as the methodology of this research.
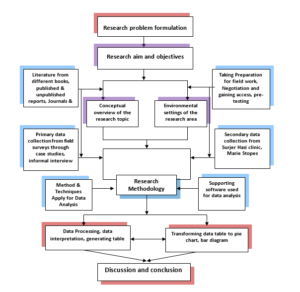
Figure 02: Methodological flow-chart of the study (Source: Field Work)
3.6 Data Processing and Analysis
All the collected and gathered data, both in primary and secondary form, has been analyzed by simple statistical techniques using Microsoft Excel 2016 software. Then, the data were presented in various ways, like tables, graphs, diagrams, etc., to get the result of the study.
- RESULT AND DISCUSSION
Sexually transmitted diseases (STDs) are infections transmitted from an infected person to an uninfected person through sexual contact. Bacteria, viruses, or parasites can cause STDs and STIs. Examples include gonorrhea, genital herpes, human papillomavirus infection, HIV/AIDS, chlamydia, and syphilis. Healthcare providers often use the term “infection” rather than “disease” because it is possible for a person to have no symptoms but still have the infection and require treatment.
4.1 Socio-Demographic Information of STD-infected female workers
The socio-demographic information about the STDs affected by female workers, such as age, educational background, religion, marital status, family structure, job position, monthly salary, etc., is presented in different tables, pie charts, bar diagrams, etc. We can easily get an idea about the affected population. The World Health Organization (WHO) estimates that there are more than 1 million new STDs acquired each day globally. People between the ages of 15 and 24 acquire half of all new STDs, and 1 in 4 sexually active adolescent females has an STD. However, STD rates among seniors are increasing.
Table 01: Age Structure of STDs affected female workers
| Age group | Number of workers | Percentage |
| 20 | 50 | 25.00 |
| 21 – 25 | 82 | 41.00 |
| 26 – 30 | 38 | 19.00 |
| 31– 35 | 15 | 7.50 |
| 36 – 40 | 7 | 3.50 |
| 8 | 4.00 | |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic
The majority of STDs and infectious female workers are in the age group of 20 to 25. But the workers under twenty also have a higher percentage, about one-fourth of the total affected study population. A few of them are over the age of forty.
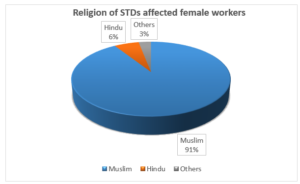
Figure 03: Religious background of the STDs affected workers (Source: Surjer Hasi Clinic)
Religious background is a very important issue regarding this research. In most cases, religion determines people’s lifestyles. This pie chart shows that 91 per cent of STD-infected female workers come from Muslim families. A few female workers belong to Hinduism or other religions.
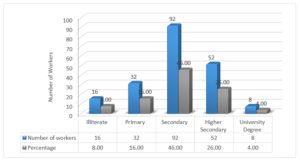
Figure 04: Educational Background of the STDs affected workers (Source: Surjer Hasi Clinic)
From the figure, we can see that most of the female workers who are affected by STDs and infectious diseases are not very educated. 46 per cent of them are enrolled in secondary school. 26 per cent of the female workers passed higher secondary. Only 4 per cent of female workers had a university degree and worked in the human resources department and a few other sections.
Table 02: Marital Status of STDs affected female workers
| Marital Status | Number of workers | Percentage |
| Unmarried | 47 | 23.50 |
| Married | 121 | 60.50 |
| Divorced | 17 | 8.50 |
| Separation | 15 | 7.50 |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic
Most female workers are married, and their percentage is about 61. There are also a few female workers who are divorced or in separation. But the fact is that unmarried, divorced, and separated females are infected by STDs and infectious diseases, which indicates a future threat to society. That means more people will be affected by this infection.
Table 03: Family Structure of STDs affected female workers
| Family Structure | Number of workers | Percentage |
| Individualistic Life | 45 | 22.50 |
| Living with Parent | 34 | 17.00 |
| Living with Husband | 95 | 47.50 |
| Living in Mess | 26 | 13.00 |
| Total | 200 | 100.00 |
Source: Fieldwork
The family structure of the STD-affected female workers is categorized into four sections. Though most of the female garment workers are living with their husbands, a large number of female workers are living in a mess or individually in a rented house. About 17 per cent of the female workers are living with their parents.
Table 04: Distribution of women workers according to their type of work performance
| Working Position | Number of workers | Percentage |
| Helper | 37 | 18.50 |
| Operator | 64 | 32.00 |
| Quality Controller | 12 | 6.00 |
| Supervisor | 23 | 11.50 |
| Line chief | 8 | 4.00 |
| Embroidery | 35 | 17.50 |
| Polyer | 8 | 4.00 |
| Folding | 6 | 3.00 |
| HRM | 3 | 1.50 |
| Support Staffs | 4 | 2.00 |
| Total | 200 | 100.00 |
Source: Fieldwork
There are many divisions in a readymade garment factory. As most of the workers are female, they work in different positions. Among them, 32% of the female workers are working as operators. Above 18% are helpers, and a few work in HRM and supporting stuff.
Table 05: Working hours and Length of services
| Working Hours | Length of Service (Years) | Total | |||
| 3 | 4 | 5 | |||
| 8 | 7 | 5 | 3 | 23 | |
| 9 | 27 | 15 | 6 | 4 | 52 |
| 10 | 67 | 13 | 6 | 5 | 91 |
| 14 | 8 | 5 | 7 | 34 | |
| Total | 116 | 43 | 22 | 19 | 200 |
Source: Fieldwork, 2018
The working hours of a female garment worker depend on their position and the duration of the job. Those working as a helper and operator who are also new to the job must work more hours than a relatively better position holder and experienced worker. In this case, those who have to work more hours are harassed by their male counterpart, or in some cases, they fall in love with their colleague, boss, or higher officials.
Table 06: Monthly Income of STDs affected female workers
| Monthly Income | Number of workers | Percentage |
| 16 | 8.00 | |
| 8000 – 10000 | 29 | 14.50 |
| 11000 – 13000 | 58 | 29.00 |
| 14000 – 16000 | 53 | 26.50 |
| 17000 – 19000 | 32 | 16.00 |
| 12 | 6.00 | |
| Total | 200 | 100.00 |
Source: Fieldwork, 2018
Most female workers are helpers and operators, so their monthly salaries are low. 29 per cent of the female workers earn 11 to 13 thousand takas. Only 6 per cent of the female workers earn more than twenty thousand takas and are in a relatively better position.
4.2 Knowledge of STDs and Infectious Diseases
Most STDs affect both men and women, but in many cases, the health problems they cause can be more severe for women. If a pregnant woman has an STD, it can cause serious health problems for the baby. But it is a matter of sorrow that our knowledge of STDs and infectious diseases is very poor.
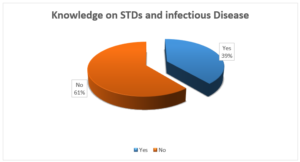
Figure 05: Female worker’s knowledge of STDs and Infectious Diseases (Source: Fieldwork)
This pie chart shows that 61 per cent of infected females don’t have proper knowledge of STDs and infectious diseases. This is because their education level is not so high. They just passed the primary level, or some passed the secondary level. 39 percent of them don’t know the term STDs properly, but they have a slight knowledge about them.
Table 07: Sharing problems with others
| Sharing problems with others | Number of workers | Percentage |
| Yes | 68 | 34.00 |
| No | 132 | 66.00 |
| Total | 200 | 100.00 |
Source: Fieldwork
Female workers whom STDs and other infectious diseases infect are not willing to share their problems with others. It is one kind of social stigma in our society.
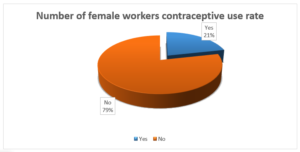
Figure 06: Contraceptive use during intercourse (Source: Surjer Hasi Clinic)
As a moderate Muslim country, most of the female workers partners are not interested in using any sort of contraceptives during sexual intercourse, and their percentage is about 79. Only 21% of the female workers and their partners used contraceptives during sexual intercourse.
4.3 The symptoms of the problem or infection
In some cases, people with STDs have no symptoms. With time, any symptoms that were present may improve. It is also possible for a person to have an STD with no symptoms and pass it on to others without knowing it.
Table 08: The Symptoms of the problem or infections
| Symptoms of the problem | Number of workers | Percentage |
| Painful or frequent urination | 37 | 18.50 |
| Unusual discharge from the vagina | 32 | 16.00 |
| Itching and redness in the genital area | 24 | 12.00 |
| Abnormal vaginal odor | 27 | 13.50 |
| Anal itching, soreness, or bleeding | 32 | 16.00 |
| Abdominal pain | 36 | 18.00 |
| Fever | 12 | 6.00 |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic, 2018
Table 09: Duration of infection (how long they suffer)
| Duration of the problem (in months) | Number of workers | Percentage |
| 25 | 12.50 | |
| 3 – 6 | 58 | 29.00 |
| 6 – 12 | 38 | 19.00 |
| 12 – 24 | 35 | 17.50 |
| 44 | 22.00 | |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic, 2018
The infected female can understand their problem after 3 months. Before that, they didn’t take it seriously. After understanding the problem, they go to the hospital or doctor for treatment. In most cases, medicine can control the infection within 6 months.
4.4 Treatment of STDs and Infectious Diseases
Antibiotics can treat STDs caused by bacteria, yeast, or parasites. There is no cure for STDs caused by a virus, but medicines can often help with the symptoms and keep the disease under control. Correct usage of latex condoms greatly reduces, but does not eliminate, the risk of catching or spreading STDs. The most reliable way to avoid infection is to not have anal, vaginal, or oral sex.
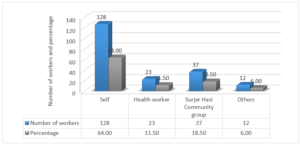
Figure 07: Reference (from whom they know about treatment) (Source: Surjer Hasi Clinic)
The above chart shows how the female workers go for treatment in the hospital and who gives them information about the hospital where they can go for treatment. This diagram shows that 64 per cent of female workers go for treatment out of their interest. About 30 per cent of the infected workers are being informed by the health assistants of different governments and NGOs.
Table 10: Routine checkup during treatment
| Duration | Number of workers | Percentage |
| After 3 days | 126 | 63.00 |
| After 7 days | 48 | 24.00 |
| After 15 days | 14 | 7.00 |
| After a month or more | 12 | 6.00 |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic
Those infected by the disease must go for routine checkups within a certain period. STD-affected people have to go for routine checkups after 3 days, but other infected female workers have to go for routine checkups after 7 days. Sometimes, they visit the hospital frequently for checkups, like after 15 days or a month.
Table 11: Statistics on Reduction of STDs and Infectious Disease
| Category | Number of workers | Percentage |
| Having Possibilities | 148 | 74.00 |
| Having 50/50 Possibilities | 35 | 17.50 |
| No Idea | 17 | 8.50 |
| Total | 200 | 100.00 |
Source: Surjer Hasi Clinic
The reduction of STDs and infectious diseases is possible by taking some medicine. A total cure is not possible, but it is possible to reduce symptoms by taking medicine. It can reduce symptoms by over 70 per cent by taking proper treatment. In less than twenty per cent of cases, there are 50–50 possibilities to cure the infection. In about 10 per cent of cases, they have no idea whether it is possible to cure.
4.5 Facilities provided by Surjer Hasi Clinic
The following chart shows the facilities provided by the Surjer Hasi Clinic. Facilities are categorized in four ways: the benefits card, the shukhi pill, the implant injection, and the condom. Benefit cards are also available in three types. The first is FCC, which applies to those with sufficient earnings for treatment. The second one is HBC, which applies to middle-income groups, and the third is the LA card, a free treatment card given by the clinic authorities. Those with LA cards get all kinds of free tests, medicine, etc.
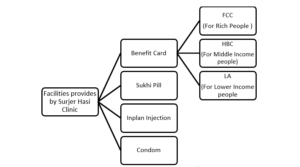
Figure 08: Facilities provided by Surjer Hasi Clinic
An effort has been made to understand the condition of STDs and infectious diseases among the female workers in the study area. This study roughly gets an idea of how STDs affect women by age, educational background, marital status, monthly income, knowledge about STDs and treatment conditions, etc. The major findings included that most of the STD-infected female workers, about 41%, are in young groups. They belong to the age group of 20–25 years. It indicates that the young generation is the most vulnerable group to infections. Many female RMG workers are infected with STDs; they are married women. But the fact is that unmarried, divorced, and separated females are infected by STDs and infectious diseases, which indicates a future threat to society. That means more people will be affected by this infection. A major portion of STD-infected females are from lower-income groups. It indicates that the lower-income group earns money for their daily necessities by engaging in sexual activities with too many people. Most of the workers are in different positions. Among them, 32% of the female workers are working as operators. Above 18% are helpers, anwork in HRM and supportpporting staff. The study shows that 61 per cent of infected females don’t have proper knowledge of infectious diseases. Only 39 per cent of them have a slight knowledge of it. It is because most of the workers are not well educated. For that reason, they are not conscious enough of their health-related infections. Female workers whom STDs and other infectious diseases infect are not willing to share their problems with others. It is one kind of social stigma in our society. Most of the female worker’s partners are not interested in using any sort of contraceptives in sexual intercourse, and their percentage is about 79. Only 21% of the female workers use contraceptives during sexual intercourse. Workers were not aware of the infection until they faced severe health problems. They have faced many health problems, but they don’t know whether they are infected with STDs and infectious diseases or not. When the health condition worsens, they go to the hospital for treatment. The infected female can understand their problem after 3 months. Before that, they didn’t take it seriously. After understanding the problem, they go to the doctor for medicine and can control the infection within 6 months. 64 percent of female workers go treatment out of their interest. About 30 per cent of the infected workers are being informed by the health assistants of different governments and NGOs. STD-affected people have to go for routine checkups after 3 days, but other infected female workers have to go for routine checkups after 7 days. Sometimes, they have to go to the hospital frequently to check their infection status, like after 15 days or after a month. A total cure is not possible, but it is possible to reduce symptoms by taking medicine. It has the potential to reduce symptoms by over 70 per cent. In about 10 percent of cases, they have no idea whether possible to cure or not. Female garment workers are mostly deprived of material access to daily expression. According to research, the majority of women earning between $11,000 and $13,000 have STD. They are working in the operator sector. 76% of married women suffer from STD-related diseases. They cannot cross the secondary level of education. So, it can be said that these data represent Marxism in such ways as:
- ”Historical materialism” ‘the history of all hitherto existing society is the history of class struggles’ (Marx and Engels, 1848words/1978:473)
- In other words, the dynamics of historical changes are rooted in opposing a product of private property distribution of private property.
- The evolution of history has been shaped by a dialectical process in which each stage of development contains within it the seeds of its destruction—its own ‘gravediggers’.
- The mode of economic production formed the ‘base’ of society that, in turn, determined a society’s ‘society ‘superstructure’ (Marx 1859/1978:4).
- ‘The ideas of the ruling class are in every epoch the ruling idea’s (Marx and Engels 1846/1978:172).
This study relates to Marx’s conflict theory. In my research results, I found that 91% of Muslim women are STD-affected. On the other hand, 60% of married women are highly infected by STDs. 47.50% of STD infected women are living with their husbands. 32% of women who work in the operator sector are highly vulnerable to STDs. 18.50% of women are infected by STDs who are working as helpers in garments. We can see that 61% of women do not know about STDs or infectious diseases. 66% of women don’t share their problems with their partners or others. Most women don’t visit the doctor to share their problems within 3–6 months. 64% of women seek treatment in their self-interest. These data show Beck’s risk theory and modernity. He argues that the risk inherent in modern society would contribute to forming a global risk society. Technological change, shifting employment patterns, job insecurity, and declining traditions and customs are the sole causes of STD infection.
- CONCLUSIONS
The study was conducted to assess the status of STDs and infectious diseases among female workers in DEPZ. Under the major objectives, it tried to reveal the socio-demographic conditions of STDs and infectious disease-infected female workers, the causes of infection, and its effect on their health, social, and economic status. The findings of the study show that 41% of female workers were affected by STDs and infectious diseases belonging to the age group of 20–25 years. Most of the female workers who are affected by STDs and infectious diseases are not well educated. It was found that about 60 percent of female workers who are married have been suffering from STDs and infectious diseases. The study also discovered that 61 percent of female workers don’t have proper knowledge about STDs and infectious diseases at all. Due to a lack of knowledge about STDs and infectious diseases, the situation has become very severe. Low levels of education among female workers are responsible for most of the problems they face. Moreover, some female workers are engaged in sexual activities for social security. It is also a disaster for them, even for society. Since a significant proportion of female workers are in Bangladesh in the RMG sector, any kind of unwanted and unusual health hazard will be a disaster for the country and its total population. Hence, measures need to be adopted to encourage the enrollment of girls, especially in secondary education and above, to improve their knowledge of health-related issues and reduce the risk of getting affected by such infectious diseases. So, all the concerned authorities must come forward to solve the problem and build a healthy nation.
REFERENCES
- Afroz, J., Jubyda, F. T., Sharmin, S., Rana, M., Dey, A. K., Farzana, T., & Sarkar, M. H. (2023). Prevalence of hepatitis B and C, and syphilis among aspirant migrant workers of Bangladesh. African Health Sciences, 23(2), 161-8.
- Ahmed, S., & Islam, N., 2014. Physical and Mental Health of the Workers in the Readymade Garment Industry of Bangladesh Pearl Journal of Management, Social Science and Humanities Vol. 1 (1), pp. 8-1 7, April, 2015 ISSN 2449-1829
- Ahmed, S., & Raihan, M. Z., 2014. Health Status of the Female Workers in the Garment Sector of Bangladesh Çankırı Karatekin Üniversitesi İktisadi ve İdari Bilimler Fakültesi Dergisi, 4(1), 43-58.
- Akhter, S., Salahuddin, A.F.M., & Iqbal, M., 2010. Health and occupational safety for female workforce of garment industries in Bangladesh Journal of Mechanical Engineering, Vol. ME 41, No. 1, June 2010 Transaction of the Mech. Eng. Div., The Institution of Engineers, Bangladesh
- Akter, R. (2022). Knowledge, awareness and prevention of sexually transmitted diseases among women in urban slums. International Journal of Research in Business and Social Science (2147–4478), 11(4), 466–472.
- Alam, N., Wahed, T., Alam, A., Dema, P., Oishi, S. N., & Nahar, Q. (2021). Condom use, symptoms of suggestive sexually transmitted infections, and health care seeking among female sex workers in Bangladesh. International Journal of STD & AIDS, 32(12), 1114-1122.
- Ali, R.N., Begum, F., Salehin, M.M., and Farid, K. S., (2008). Livelihood pattern of rural women garment workers at Dhaka city, Bangladesh Agri. Univ. 6(2): 449–456.
- Barkat, A., Majid, A. B. M., Ara, R., & Mahiyuddin, G., 2008. Change in Attitudes and Behavior of Garment Owners, Managers and Workers towards Gender and Reproductive Health Issues HDRC, UNFPA Bangladesh, Dhaka: December 2008
- Begum, N., (2016). Maintenance of Health and Safety of Women Garment Workers: A Study of South East Textile (Pvt) Limited BRAC Institute of Governance and Development, BRAC University Dhaka-1212, Bangladesh
- BGMEA (Bangladesh Garment Manufacturers and Exporters Association) Member’s Directory. 2008. Annual Report. Dhaka, Bangladesh. pp. 4-7.
- Cancer, M., & Paul, N., 2005. Predicting Health Behaviour. Berkshire, England: Open University Press, The McGraw Hill Companies.
- Chowdhury, S. (2018). Rights of Female Garments Workers in Bangladesh: A
- Case of Chittagong BRAC Institute of Governance and Development BRAC University
- Farabi, T. J., Jahangir, Y. T., Clara, A. A., Nabi, M. H., & Hawlader, M. D. H. (2021). Sexually Transmitted Infections among Street, Hotel, and Residence-Based Female Sex Workers in Dhaka, Bangladesh: Prevalence from Three HIV/STI Drop-in-Centers. Sexes, 2(1), 69–78.
- Garai, J., (2016). Gender and HIV/AIDS in Bangladesh: A review Journal of Health and Social Sciences 2016; 1,3:181-198.
- Gourab, G., Khan, M. N. M., Hasan, A. R., Sarwar, G., Irfan, S. D., Reza, M. M., … & Khan, S. I. (2019). The willingness to receive sexually transmitted infection services from public healthcare facilities among key populations at risk for human immunodeficiency virus infection in Bangladesh: a qualitative study. PloS one, 14(9), e0221637.
- Halim, S., & Kabir, A. H., 2005. Globalization, Gender and Labour Market: Some Evidence from RMG sector. A Journal of Social Science. 22(1): 29-42.
- Hasnain, M., Islam, A., Smyth, R., Tan, H. A., & Wang, L. C. (2022). Effects of a safe sex intervention on the commercial sexual behaviour of brothel sex workers in Bangladesh: Evidence from a randomized controlled trial.
- Huda, M. N., Ahmed, M. U., Uddin, M. B., Hasan, M. K., Uddin, J., & Dune, T. M. (2022). Prevalence and demographic, socio-economic, and behavioural risk factors of self-reported symptoms of sexually transmitted infections (STIs) among ever-married women: Evidence from Nationally representative surveys in Bangladesh. International Journal of Environmental Research and Public Health, 19(3), 1906.
- Islam, A., Tan, H. A., Bristow, C. C., Hasnain, M. G., Smyth, R., & Wang, L. C. (2021). Impact of Testing on Sexually Transmitted Infections among Female Brothel Sex Workers in Bangladesh: A Randomized Controlled Trial. The American Journal of Tropical Medicine and Hygiene, 104(6), 1991.
- Kabeer, N., (2000). The Power to Choose: Bangladeshi women and labour market decisions in London and Dhaka. Verso Press, London and New York.
- Kayesh, I., Huq, M., Faruk, M. O., Sahin, M. A. R., Manjur, S., & Begum, S. (2023). Sexual Risk Behaviors Predisposing Female Sex Workers (FSWs) to Sexually Transmitted Infections (STIs) in Daulatdia, Bangladesh. OIRT Journal of Scientific Research, 3(1), 1-6.
- Khan, M. R., & Ahmed, F., (2005). Physical status, nutrient intake and dietary pattern of adolescent female factory workers in urban Bangladesh Asia Pac J Clin Nutr 2005;14 (1):19–26.
- Maesschalck, J., & Paesen, H. (2021). Profiling Organizational Culture: Using Grid-Group Cultural Theory as a Lens to Take a Snapshot of an Organization’s Culture. Sage Open, 11(4), 21582440211061564.
- Mahmood, S. (2020). Female Garment Workers in Bangladesh: Violence, Gender and HIV/AIDS. AIDS (June 26, 2020). Journal of Social and Political Sciences, 3(2).
- Mahmood, S. (2021). Female Garment Workers’ Understandings of HIV in Bangladesh. American Journal of Public Health, 9(2), 81–89.
- Majumder, P. P., & Begum, A., June 2000. The Gender Imbalance in Bangladesh’s Export Oriented Garment Industry, The World Bank, Development Research Group/Poverty Reduction and Economic Management Network.
- Moshiri, F. (2019). Revolutionary conflict theory from an evolutionary perspective. In Revolutions of the Late Twentieth Century (pp. 4–36). Routledge.
- Mythen, G. (2021). The critical theory of world risk society: a retrospective analysis. Risk Analysis, 41(3), 533–543.
- Neuman, W.L., (2013). Social Research Methods: Qualitative and Quantitative Approaches.
- Paul-Majumder, P., 2003. Health Status of the Garment Workers in Bangladesh. Agrambagh, Motijheel, Dhaka: Bangladesh at Associates Printing Press.
- Rahman, A., & Rahman, M., (2013). Sickness and Treatment: A Situation Analysis among the Garments Workers AKMMC J 2013: 4(1): 10-14
- Rahman, M. M., Haq, S., Rashid, S., & Hossain, S. R. (2022). Pattern of Sexually Transmitted Infections: Treated in A Private Clinic in Dhaka, Bangladesh. Glob Acad J Med Sci, 4.
- Schunk, D. H., & DiBenedetto, M. K. (2020). Motivation and social cognitive theory. Contemporary educational psychology, 60, 101832.
- Sikdar, M.M.H., Sarkar, M.S.K., & Sadeka, S., 2014. Socio-Economic Conditions of the Female Garment Workers in the Capital City of Bangladesh International Journal of Humanities and Social Science Vol. 4 No. 3; February 2014
- Sobhan, R. & Khundker, N., 2001. Globalization and Gender. Dhaka, the University Press Limited.
Publication History
Submitted: October 10, 2023
Accepted: October 24, 2023
Published: November 30, 2023
Identification
D-0154
Citation
Kamrunnahar Koli (2023). Sexually Transmitted Diseases & Infectious Diseases among Female Workers in Dhaka Export Processing Zone: A Sociological Analysis. Dinkum Journal of Social Innovations, 2(11):609-627.
Copyright
© 2023 DJSI. All rights reserved.